Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by kamar hamade and Version 2 by Sirius Huang.
The pomegranate fruit is made of white to deep purple seeds that are enclosed in a white, spongy, astringent membrane, also known as pericarp, covered by a thick red skin and a crown-shaped calyx. It contains a variety of beneficial ingredients, including flavonoids, ellagitannin, punicalagin, ellagic acid, vitamins, and minerals. Pomegranates possess numerous health benefits, and their use in disease treatment has been widely recognized since antiquity.
- pomegranate
- antioxidant
- respiratory
- diseases
1. Introduction
Phytotherapy is defined as the usage of plant-derived products in the treatment and prevention of diseases. Since the beginning of human civilization, medicinal plants have been used as pharmaceutics for the prevention and treatment of various diseases [1]. Medicinal plants play a major role in pharmaceutical industries as they contribute to the manufacturing of drugs [2]. Development of pharmaceutical drugs from plants reduces the use of synthetic antibiotics and increases life expectancy [3][4][3,4]. In the meantime, scientific interest in medicinal plants is increasing due to the high cost and side effects caused by allopathic drugs, in addition to the emergence of resistant microbial strains [5].
Pomegranate (Punica granatum L.) is derived from a deciduous tree in the Lythraceae family. According to reports, it first appeared in modern times in Iran and has since spread throughout the world. Since ancient times, it has been cultivated throughout the Mediterranean region and Northern India [6]. The pomegranate fruit is made of white to deep purple seeds that are enclosed in a white, spongy, astringent membrane, also known as pericarp, covered by a thick red skin and a crown-shaped calyx (Figure 1). This fruit is known to exhibit several biological properties, including antibacterial, anti-inflammatory, antioxidant, and anticancer activities [7][8][7,8]. The scientific studies on the health advantages of pomegranates that have been published over the past few decades demonstrate the scientific community’s intense interest in the fruit’s medicinal potential. Pomegranate has been used in a variety of medical systems for the treatment and therapy of a wide range of diseases and illnesses. For instance, it was recommended as an antiparasitic agent and as a treatment for diarrhea and ulcers in ancient Indian medicinal systems [9][10][9,10]. Its importance in the treatment of diabetes has been recognized in another traditional system, the Unani system of medicine [11].
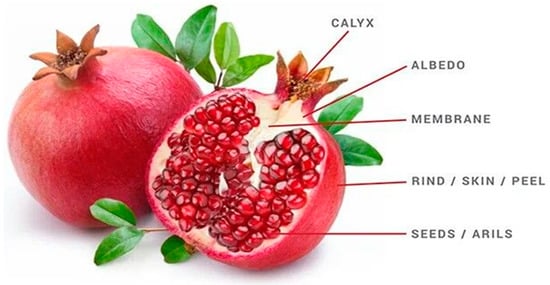
Figure 1.
Pomegranate fruit parts.
In addition, pomegranate and its constituents have been shown in studies to effectively affect a number of signaling pathways involved in inflammation, cellular transformation, hyperproliferation, angiogenesis, and the start of tumorigenesis, as well as suppressing the later stages of tumorigenesis and metastasis [12][13][12,13]. Pomegranate peel has been shown to inhibit a wide range of pathogens, including viruses, bacteria, fungi, and mold [14]. It has a great therapeutic effect on chronic inflammation, particularly digestive tract inflammation like ulcerative colitis [15]. Furthermore, all waste parts of the pomegranate fruit, such as the peel and seeds, can be processed into value-added products with industrial, medicinal, and cosmetic value [16].
Chronic respiratory diseases are one of the leading causes of death globally. Victims of lung disorders frequently experience long-term difficulties, with one of the major causes being treatment side effects as well as psychosocial struggles [17]. Respiratory diseases are characterized by unrestricted cell proliferation and no single defined cause, but they are associated with several risk factors, including tobacco use, infection, radiation exposure, air pollution, obesity, and alcohol consumption. Several epigenetic/environmental agents have been identified as key players in the development and progression of such diseases [18][19][18,19]. Despite significant advances in treatment options, the number of cases and deaths continues to rise, and millions of people die from these diseases globally [20][21][20,21].
2. Pomegranate in the Treatment of Respiratory Diseases
2.1. Pomegranate and Asthma
Asthma is a chronic condition in which the airways, due to inflammation, become narrow and swollen and are blocked by excess mucus. Treatment of asthma by inhalers can help control and minimize the symptoms, but their adverse effects ultimately limit their long-term use [22][23][44,45]. Studies have shown that pomegranate can play an effective medicinal role in asthma treatment. Eosinophils are involved in the development of asthma exacerbation and that IL-5 plays an important role in the activation and maturation of eosinophils [24][46]. Oliveira et al. revealed that the micro-encapsulated leaf extract from Punica granatum inhibited eosinophil recruitment to bronchoalveolar fluid and reduced the production of inflammatory cytokines such as IL-1b and IL-5 in the lungs of BALB/c mice used as asthma models [25][47]. Another study revealed that tannins extracted from the flower buds of P. granatum display an anti-histaminic activity that could contribute to its role as a traditional treatment for asthma [26][48]. This antihistaminic activity may open the door for future research studies that could evaluate the cumulative effect between pomegranate extracts and other antihistaminic drugs. All these findings depicted the effective role of pomegranate as a therapy for asthma; more studies are needed for exploring the exact mechanism behind this therapeutic effect.2.2. Pomegranate and COPD
Chronic obstructive pulmonary disease (COPD) is a respiratory disorder that causes airflow blockage and breathing-related problems. COPD is the third leading cause of mortality worldwide [27][28][49,50]. Cigarette smoking, indoor air pollution, and occupational dusts, fumes, and chemicals are important risk factors of COPD [29][51]. The exposure to cigarette smoke leads to severe oxidative damage to the lungs and to neutrophils recruitment via IL-1β and TNF-α. Neutrophils secrete proteases such as neutrophil elastase, caspases, and matrix metalloproteinases (MMPs), which break down the connective tissue in the lungs, resulting in emphysema [30][52]. Pomegranate has proven to be effective in treating COPD, even though the study done by Cerda et al. showed that pomegranate juice supplementation had no benefit in treating patients with stable COPD due to the metabolism of its polyphenols by the colonic microflora [31][53]. In fact, variations in polyphenol bioavailability and absorption could be possibly due to differences between individual and between species in gut microflora as well as differences in polyphenol structure [32][33][54,55]. Furthermore, in vitro research suggests that certain polyphenols in the colon may induce the production of conjugation enzymes, whereas in vivo research suggests that the composition of microbiota influences the capacity for producing enzymes required for conjugation [34][35][56,57]. External factors such as the food matrix in which polyphenols are consumed and health status can also influence polyphenol absorption efficiency. Age-related changes and metabolic disorders in the host have been shown to influence the distribution of intestinal microbiota, as well as the host’s ability to metabolize specific polyphenols and the types of conjugated forms produced [36][37][38][58,59,60] Other research studies had proven the effectiveness of pomegranate in treating COPD. Husari et al., 2016, proved that pomegranate juice supplementation in animal models exposed to cigarette smoke reduced the emphysematous changes and attenuated the expression of inflammatory mediators such as IL-1β, IL-6, and TNF-α [39][61]. Accordingly, pomegranate reduces apoptosis and oxidative stress induced by cigarette smoke exposure in the lungs. In vitro, pomegranate juice inhibited the devastating effects of cigarette smoke on cultured human alveolar cells [39][61]. In conclusion, these studies proved that pomegranate can act as a potential treatment for COPD as it attenuates the damaging effects of cigarette smoke on the lungs.2.3. Pomegranate and Influenza
Influenza is a viral disease that affects the upper and lower respiratory tract. It is caused by a wide range of influenza viruses. Some of these viruses infect humans, while others are specific to other species [40][41][62,63]. Some medicinal plants have been identified for use in treating influenza due to the failure of some synthetic drugs because of side effects [42][43][64,65]. Pomegranate has been shown to possess a therapeutic effect against influenza virus infections. Pomegranate polyphenol juice extract showed anti-influenza properties, as it had inhibited the replication of influenza A virus in Madin-Darby canine kidney cells (MDCK). Punicalagin was found to have virucidal effects, being the most effective anti-viral component of polyphenol extract. Punicalagin suppressed viral RNA replication and blocked the agglutination of chicken RBCs by the virus. Moreover, combining oseltamivir, an anti-influenza drug, with pomegranate polyphenol extract showed a synergistic effect [44][66]. Another study revealed that pomegranate polyphenols inhibited influenza virus infectivity. Electron microscopic analysis revealed that viral inactivation by pomegranate polyphenols was due to virion structural damage, with small changes in envelope glycoproteins [45][67]. Moradi et al. showed that the ethyl alcohol extract of pomegranate peel can suppress the replication of influenza A virus through inhibiting viral adsorption and internalization and viral RNA transcription [46][47][68,69]. Hence, pomegranate extracts must be further analyzed for therapeutic and prophylactic potential against influenza epidemics and pandemics.2.4. Pomegranate and COVID-19
The extremely contagious respiratory illness COVID-19 is brought on by a new strain of coronavirus known as SARS-CoV-2 (severe acute respiratory syndrome-coronavirus-2) [48][70]. Coronavirus causes infections in the respiratory tract ranging from mild colds to severe acute respiratory distress syndrome [49][71]. The interaction of SARS-CoV-2 spike (S) transmembrane glycoprotein with the angiotensin-converting enzyme 2 (ACE-2) receptor on host cells is an essential step for virus entry and onset of infection [50][72]. Attenuating the binding ability of S-glycoprotein to ACE-2 receptor was one of the primary targets for treating COVID-19 disease [51][73]. Pomegranate was shown to be potential candidate for possible therapeutic application against COVID-19. A recent study showed that pomegranate peel extract significantly blocked the binding of S-glycoprotein to ACE-2 receptor [52][74]. Another computational study showed that punicalagin and punicalin from pomegranate peel extract inhibited the SARS-CoV-2 internalization process [53][75]. Punicalagin alone or its combination with Zn particles inhibited the activity of SARS-CoV-2 3CL protease in vitro [54][76]. 3CL protease is indispensable for disease progression and viral replication, as it cleaves the viral polyprotein to give a single useful protein [55][56][77,78]. Other studies had also shown that some anthocyanins and hydrolysable tannins may inhibit viral replication via binding with catalytic dyad residues of 3CL protease [57][58][59][79,80,81]. Medicinal plants rich in anthocyanins and tannins, such as pomegranate, can be used as natural anti-COVID-19 therapeutic agents (Figure 24). Moreover, a clinical case study revealed that the consumption of fresh pomegranate juice showed prophylactic and therapeutic effects against COVID-19 [60][82]. These findings support the efficacy of P. granatum L. as a therapeutic drug in the treatment of COVID-19 (Figure 24).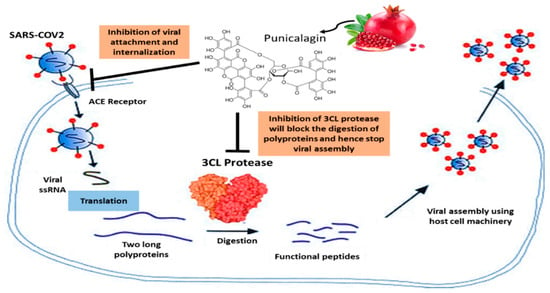
Figure 24.
Pomegranate’s role in COVID-19.
2.5. Pomegranate and Lung Cancer
Lung cancer remains the leading cause of cancer-related mortality worldwide. The year 2020 recorded 2.2 million new lung cancer cases, accounting for 11.4% of the global cancer burden [61][62][83,84]. Many technical and pharmacological advances have been made in the staging and treatment of lung cancer, with the approval of newly synthesized chemotherapeutic drugs that improve the prognosis of patients diagnosed with metastatic tumors [63][85]. Yet these drugs are linked to many undesired side effects, which can be avoided by their substitution with natural products that have historically been invaluable as an origin of therapeutic agents [64][65][86,87]. Pomegranate has been shown to exhibit anti-cancerous effects against lung cancer in cell culture and in vivo studies. Punicalagin, an ellagitannin found in pomegranate peel, acts as an anti-proliferative agent on the A549 human lung carcinoma cell line. Punicalagin treatment induced apoptosis in A549 cells through mitochondria-mediated pathways without having any effect on normal lung fibroblast cells (MRC-5 cell line) [66][88]. Aqil et al. showed that punicalagin displays a strong anti-oxidant potential protecting against oxidative DNA damage and exhibits a strong anti-proliferative activity against lung cancer cells [67][89]. Punicalagin and its hydrolytic product (ellagic acid) showed cytotoxic effects on both human lung cancer cell lines A549 and H1299 [68][90]. Punicalagin inhibited STAT-3 translocation and accordingly induced apoptosis of A549 cells by inhibiting the expression of anti-apoptotic proteins (Bcl-2) and increasing the expression of the pro-apoptotic proteins (Bax, cytochrome C, caspase 9, and caspase 3) [69][91]. Another study investigated the anti-tumoral properties of pomegranate peel extract on A549 lung cancer cells. The authors showed that the peel extract reduced the cell viability, with a maximum growth inhibition of 80% at 250 µg/mL dose [70][92]. Moreover, the treatment of A549 cells with pomegranate fruit extract leads to a decrease in the viability of A549 cells with only minimal effects on normal human bronchial epithelial NHBE cells. Pomegranate fruit extract treatment leads to the G1 phase cell cycle arrest through the induction of WAF1/P21 and KIP1/P27, with consequent inhibition of cyclins D1, D2, and E as well as cyclin-dependent kinases cdk2, cdk4, and cdk6 [71][93]. In addition, treating A549 cells with pomegranate fruit extract resulted in the inhibition of MAPK and PI3K pathways as well as the NF-Kb pathway [71][93]. Yali Li et al. showed that pomegranate leaf extract exhibits anticancer effects through inhibiting the proliferation of A549 and H1299 non-small-cell lung carcinoma cell lines and mouse Lewis lung carcinoma cell line LL/2. Pomegranate leaf extract blocked the migration and invasion of H1299 cells via reducing the expression of metalloproteinases (MMPs), suggesting the effectiveness of pomegranate leaf extract in impairing metastasis [72][94]. Urothilin A, a major metabolite from pomegranate ellagitannins, was found to inhibit epithelial-to-mesenchymal transition (EMT) in lung cancer cells via decreasing the expression and activity of snail protein, an inducer of EMT [73][95]. Husari et al. showed that pomegranate juice supplementation to an animal model reduced the expression of HIF-1α and prevented the formation of lung nodules secondary to chronic cigarette smoke exposure, therefore decreasing the incidence of lung cancer [74][96]. These studies highlight the potential role of pomegranate fruit in the treatment of lung cancer (Figure 35).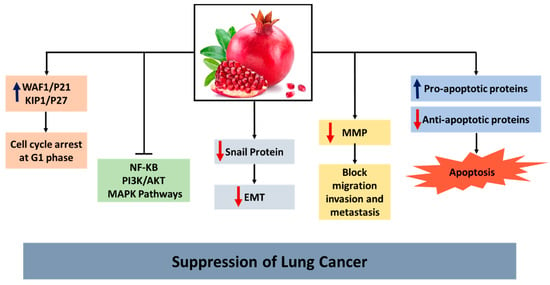
Figure 35.
Pomegranate activity in lung cancer.