Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Rita Xu and Version 1 by Mirella Profita.
Inflammation of the human lung is mediated in response to different stimuli (e.g., physical, radioactive, infective, pro-allergenic, or toxic) such as cigarette smoke and environmental pollutants. These stimuli often promote an increase in different inflammatory activities in the airways, manifesting themselves as chronic diseases (e.g., allergic airway diseases, asthma chronic bronchitis/chronic obstructive pulmonary disease, or even lung cancer). Non-coding RNA (ncRNAs) are single-stranded RNA molecules of few nucleotides that regulate the gene expression involved in many cellular processes. ncRNA are molecules typically involved in the reduction of translation and stability of the genes of mRNAs s.
- microRNAs
- asthma
- COPD
- lung cancer
1. Lung Diseases
Lung diseases are types of disorders affecting the normal pulmonary functions preventing the ability to breathe. Many respiratory diseases begin with the onset of inflammatory reactions with a key role in the pathological conditions of the lung, as the reduced airflow of asthmatic and Chronic Obstructive Pulmonary Disease (COPD) patients [1].
The causes of the asthma pathogenesis are genetic, immune, or associated with environmental factors (pollutants, allergens, and pathogens). Asthma is characterized by airway hyper-responsiveness (AHR) and leads to intermittent and usually reversible airway obstruction. The symptoms of asthma are generated by drugs, exercise, or intrinsic problems; they can be repeated wheezing, chest tightness, cough, and other symptoms all related with reversible airflow restriction. Asthma pathogenesis is regulated by the co-participation of various immune cells and cytokines that are highly heterogeneous and affect numerous aspects of asthma regarding pathologic processes and clinical manifestations. Airway inflammation is characterized by T-helper 2 cells (Th2 cells) immune response and type 2 cytokines (e.g., IL-4, IL-5 and IL-13) release, eliciting airway eosinophilia, bronchial hyperresponsiveness, mucus overproduction, airway remodeling, and immunoglobulins E (IgE) synthesis in asthma. In addition, subject with asthma show in the airway epithelial cell exfoliation, fibrosis, vasodilation of the walls, and exudation of plasma [2]. The World Health Organization described that people suffering from asthma are currently 235 million, worldwide, and children are a bigger and most vulnerable group of asthmatic population [3]. Pharmacological treatment of asthma includes its action against allergens and irritants, as well as the use of β-adrenergic receptor agonists such as bronchodilators, glucocorticoids, and antileukotrienes to suppress inflammation or immunotherapy. These conventional therapies of asthma patients keep under control the symptoms but are not able to cure completely the disease [4].
Cigarette smokers are approximately 90% of the COPD patients. Smoke habits are the first cause of risk factor for the development of COPD [5,6][5][6]. The inflammation in COPD involves the innate and adaptive immune responses. It is one of the major public health problems worldwide since it is the major cause of chronic morbidity and mortality. The subjects with COPD are older than forty years of age and had a progressive and irreversible airway obstruction, characterized by deterioration of pulmonary function time related [7], causing the destruction of the lung parenchyma. This characterizes inflammation of central and distal airways, pulmonary emphysema, respiratory bronchiolitis representing the hallmarks of COPD [5,6][5][6]. The inflammation in COPD subjects includes the recruitment of different cell types as neutrophils, macrophages, lymphocytes, and the activation of epithelial cells in the airways [5,6][5][6]. To what extent central airways may mirror events, occurring in distal lung is uncertain. β2-AR-agonist and anticholinergic drugs are as concurrent therapy used in the treatment of COPD to maximize bronchodilation and have a potential anti-inflammatory role [8]. The older compounds are modified to make novel therapeutic agents more potent, long lasting, enclosed in new inhalation devices [9].
Asthma and COPD are diseases with similarities [10]. However, they are different regarding etiology, type of inflammatory cells, mediators, consequences of inflammation, response to therapy [8] (Figure 1). COPD can originate in smoker subjects aged over 40 and its incidence increases in over 60-year-olds. Aging accelerates the decline of normal lung function in COPD patients showing a premature lung function loss.
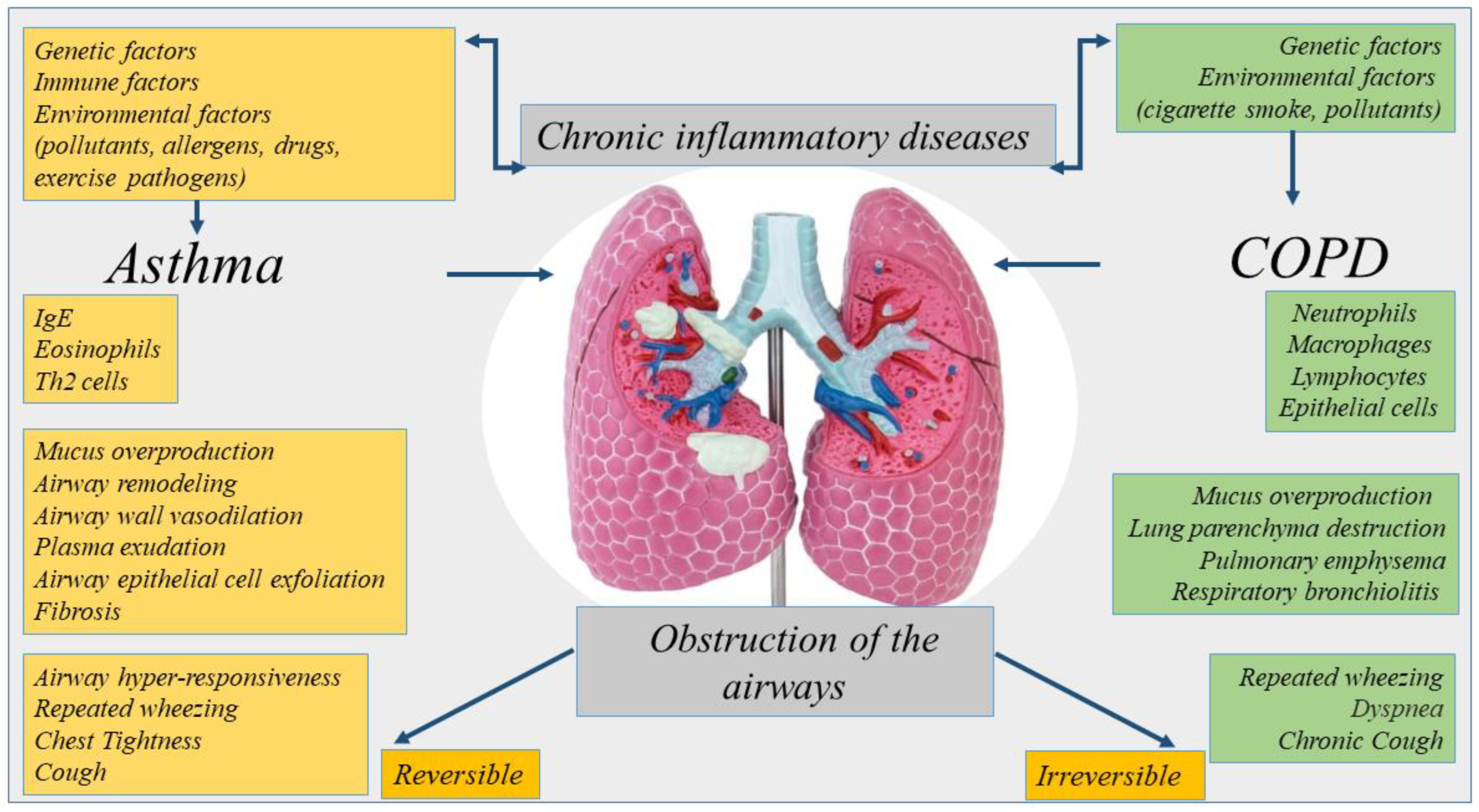
Figure 1. Representation of the etiology, inflammation, and symptoms of chronic inflammatory diseases of the lung. Asthma and COPD are diseases with similarities. However, they are different regarding etiology, type of inflammatory cells, mediators, consequences of inflammation.
The mechanisms of aging can be non-programmed or programmed. The first is related to the failure of the repair of DNA in the organs due to the increase in oxidative stress. The second is related to telomere shortening for a repeated cell division. Both aging defects are present in COPD patients per se, as physiological conditions disease. They may be involved in the progression of diseases toward lung cancer (LC). The premature aging of the lung, genetic predispositions, common pathogenic factors as growth factors, activation of intracellular pathways, or epigenetic modifications are common mechanisms that can be a cause of high prevalence of LC in patients with COPD [11].
The major risk factor for lung cancer is cigarette smoking. The smoking habit, common to COPD and LC alters the defense mechanisms regarding the antioxidant production such as superoxide dismutase, anti-proteases, and DNA repair mechanisms. If the damage to these mechanisms becomes too high in COPD patients, mutations leading to LC can occur [12]. In LC, increasing oxidative stress, reduction of DNA repair mechanisms and the resulting DNA damage, chronic exposure to pro-inflammatory cytokines, and increased cellular proliferation are common to COPD. LC is also a leading cause of morbidity and mortality in patients with COPD [13]. Mutations in oncogenes lead to an abnormal cell proliferation causing LC. The benign tumor was transformed to an invasive cancer by additional mutations that initiate spread invasiveness and anaplasia of the cells. It usually originates from the basal epithelial cells and are classified into two types, non-small-cell lung cancer (NSCLC) and small-cell lung cancer (SCLC) [14].
2. Nc-RNA Biogenesis
The nc-RNA are classified in two categories housekeeping and regulatory. The regulatory included two noteworthy ncRNA: miRNAs or miRs (transcripts of 19–25 nucleotides) and long-ncRNAs (transcripts of 200 nucleotides) (lnc-RNAs) and circular RNAs (circ-RNAs). MiRNAs generally regulate post-transcriptional gene expression in physiological and pathological processes targeting the messenger RNA (mRNA) cleavage and degradation, and/or by inducing mechanism of translational repression or mRNA degradation [16][15]. lncRNAs, interacting with DNA, RNA, or protein through various mechanisms, positively or negatively control the stage of gene expression [17,18,19][16][17][18]. Finally, circ-RNAs have multiple biological functions as miRNA sponge, transcription regulator, protein translation, interaction with protein, RNA maturation, and so on [20][19]. The biogenesis, characteristics, types, and mechanism of action ncRNAs have a relevant role in developmental and homeostasis of human tissues [17,18,19,21][16][17][18][20]. In this section we described the biogenesis of miRNA mainly reported as nc-RNA in airway diseases in this review. A conserved family of small endogenous noncoding RNA (nc-RNA) molecules (18–22 nucleotides in length) named microRNAs (miRNAs) was found in eukaryotes and have been extensively studied in human diseases and in cancer [22,23,24][21][22][23]. Many human diseases show aberrant expression of miRNAs [25,26][24][25]. MiRNAs are critical for normal animal development and are involved in a variety of biological processes such as proliferation, apoptosis, differentiation, and survival, playing an important role in gene expression regulation [27[26][27],28], also in the biological processes of the lung diseases [29][28]. MiRNA family are long transcripts called clusters, with repeated similar regions [30][29]. The discovery of new miRNAs and the description of their role in the pathogenesis of diseases are constantly evolving [31,32][30][31]. MiRNA action often suppresses expression of target gene interacting with the 3′ UTR of target mRNAs [33][32], or it has also been reported that miRNAs interact with 5′ UTR, coding sequence, and gene promoters. They shuttled between different subcellular compartments to control the rate of translation transcription [34][33]. MiRNA biogenesis is classified as canonical and non-canonical. However, the dominant pathway is the canonical miRNAs processing. The biogenesis of miRNAs starts in the nucleus with the processing of RNA polymerase II/III transcripts post- or co-transcriptionally. Pol II initiates the transcription of miRNA genes to produce pri-miRNA. Then, DiGeorge Syndrome Critical Region 8 (DGCR8), a microprocessor complex with a RNA binding protein ribonuclease III, transforms the pri-miRNA in pre-miRNA. Subsequently, DGCR8 targets N6-methyladenylated GGAC and other motifs into pri-miRNA, Drosha cleaves the pri-miRNA duplex in the hairpin structure of pri-miRNA [35][34]. Subsequently, by the exportin 5 (XPO5)/RanGTP complex action, pre-miRNA translocated from the nucleus to the cytoplasm and was transformed in mature miRNA/miRNA duplex by RNase III endonuclease Dicer and the RNA-binding protein TRBP the action. Then helicases separate the duplex by Argonaute (AGO2), and the strand guide of miRNA incorporates RISC to form a complex that recognizes specific mRNA by sequence complementarity leading to either mRNA degradation or translational inhibition [36,37][35][36] (Figure 2).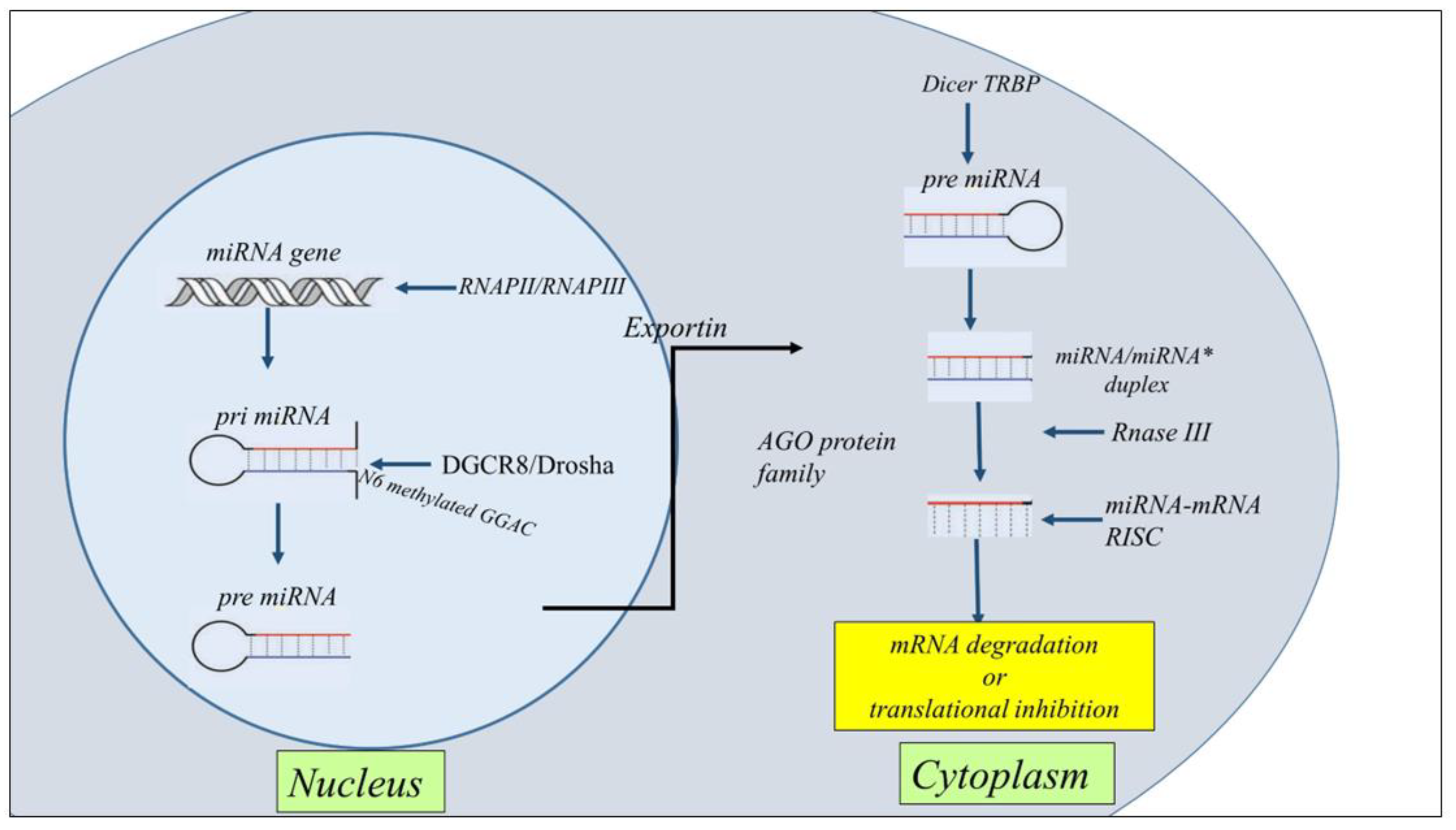
Figure 2. Schematic representation of the general steps of miRNA biogenesis. The biogenesis of miRNAs starts in the nucleus with the processing of RNA polymerase II/III transcripts post- or co-transcriptionally into pri-miRNAs. Then, a ribonuclease III enzyme transforms the pri-miRNAs in pre-miRNAs, which are transported into the cytoplasm by Exportin 5 (XPO5)/RanGTP complex action. Reaching the cytoplasm pre-miRNA is transformed in mature miRNA/miRNA* duplex by RNase III endonuclease Dicer and the RNA-binding protein TRBP the action. miRNA then forms a miRNA-mRNA RISC complex to induce mRNA degradation or translational repression.
3. Nc-RNAs in Asthma
The throughput epigenetic analysis technologies, together with traditional biological function and clinical studies improved the genetic knowledge and finding epigenetic biomarkers of asthma provided new frontiers in the precision medicine of the lung [38][37]. The knowledge of nc-RNA regulatory networks opens new perspectives for the understanding the pathogenesis of asthma [39][38]. Asthma is a heterogeneous chronic inflammatory disorder in which different endotypes contribute to defining clinical inflammatory phenotypes. It is classified as mild, moderate, and severe. Nc-RNAs, in particular microRNA profiling in asthma is involved in the definition of subtyping asthma as potential biomarkers and therapeutic targets [40][39]. Altered expression of nc-RNAs in blood, in exhaled breath condensate, or in induced sputum condensate of sputum indicate the progression of asthma and the immune response in the lung. Nc-RNAs regulate the gene expression at the post-transcriptional level and by targeting mRNAs affect the synthesis of cytokines and signaling pathways in airway inflammation [41,42][40][41]. mRNAs induce the activation of structural cells (bronchial epithelial cells, fibroblasts, endothelial cells, and smooth muscle cells) and immune cells playing an essential role in cell proliferation, differentiation, signal transduction, stress response, cell apoptosis, and other cellular and molecular aspects of asthma diseases. MiRNAs might be considered as novel biomarkers of disease [42][41]. For examples miR-21 and miR-155 are important regulators of gene expression of many immunological molecules. Higher levels of miR-21 and miR-155 are detected in the serum of asthmatic patients compared to control subjects. Both miRNAs might be considered as potential non-invasive biomarkers useful for the diagnosis and response to the therapy in eosinophilic asthma [43][42]. The inflammatory processes of asthma are regulated by the activation and differentiation of Th2 cells, secretion of cytokines, and functions of eosinophils. let-7 family, miR-193b, miR-375 (downregulated), and miR-21, miR-223, miR-146a, miR-142-5p, miR-142-3p, miR-146b and miR-155 (upregulated) represent a core set of nc-RNA involved in asthma. Many of them are involved in T-cell differentiation increasing Th2 cell phenotype and Th2 cytokines secretions active in the origin of hyperplasia and hypertrophy of bronchial smooth muscle cells [44,45,46][43][44][45]. miR-21 is involved in the switch of Th1 versus Th2 responses, and defines the mechanisms of immunoinflammatory responses, limiting in vivo immune response-mediated activation of the IL-12/IFN-gamma pathway [47][46]. miR-146a is a candidate molecule with an association with impact of genetic variation in asthma [48][47]. It together with miR-26a and miR-31 is increased in the lung tissues of asthma mice, and in bronco alveolar lining fluid (BALF) of asthma children [49][48]. Furthermore, miR-146a define endotypes of asthma in moderate asthma (MA) and severe asthma (SA). MiR-146a and lower production of resolvin D1 create a dysregulation of inflammation in children, promoting remodeling processes and leading to lung function impairment [50][49]. MiR-155 and miR-221 are associated with Th2 responses [51][50] and with cells involved in allergic response (eosinophils, macrophages mast cells) in asthma and rhinitis [39,52,53,54][38][51][52][53]. Follicular helper (Th) and regulatory T (Treg) cells are involved in allergic asthma [55][54]. MiR-17 affects T-cell-like characteristics and via the de-repression of genes encoding effector cytokines transform them in Treg cells. It modulates regulatory T-cell function through targeting eosinophils and by targeting co-regulators of the Foxp3 transcription factor Foxp3 co-regulators [56][55]. PU.1 transcription factor is a negative regulator of Th2 cytokine release. It is upregulated in the airways of allergen-challenged miR-155 knockout mice. These data underline that miR-155 regulates Th2 responses in allergic airway inflammation by transcription factor PU.1 [53][52]. Furthermore, miR-155 regulates type 2 innate lymphoid cells ILC2s and IL-33 signaling in allergic airway inflammation [57][56]. Remodeling and oxidative stress in asthma are regulated by many miRNAs. MiR-26, −133a, −140, −206, and −221, are associated with an effect on smooth muscle cell function and proliferation [39][38]. MiR-143-3p inhibits airway remodeling in asthma, suppressing transforming growth factor (TGF)-β1-induced cell proliferation and protein deposition of extracellular matrix (ECM) production proliferation via negative regulation of nuclear factor of activated T cells 1 (NFATc1) signaling [58][57]. MiR-192-5p is down-regulated in asthmatics and attenuates airway remodeling and autophagy in asthma by targeting MMP-16 and ATG7 [59][58]. The action of miRNAs can favor the progression of asthma phenotype from mild to severe stage [60][59]. However, despite the relevant role of miRNAs in asthma, few studies define their immunological activity in severe asthma. It is observed that miR-221 downregulates the action of TGF-β, on the aberrant airway smooth muscle proliferation and size, and consequently proinflammatory effects [61][60]; miR-28–5p and miR-146a/b downregulation led to circulating CD8+ T-cell activation in severe asthma [62][61]; and miR-223–3p, miR-142–3p, and miR-629–3p are well correlated with neutrophils in severe asthma [63][62]. All these findings facilitate the conclusions in this field [64][63] underlining that miRNA expression profiles might represent a risk factor for the development of a severe stage of asthma disease [28][27]. MiR-1278 inhibited inflammation in asthmatic mice and counteracted the effect of TGF-β1 in the cell proliferation and reduced apoptosis in airway smooth muscle cells (ASMCs). In particular this restudyearch showed that miR1278/SHP-1/STAT3 pathway is involved in airway smooth muscle cell proliferation in a model of severe asthma [28][27]. Recent overviews underline the emerging role of ncRNAs in childhood asthma. For instance, lncRNA CASC2 and BAZ2B are increased in the serum of childhood asthma [65,66][64][65]. CASC2 is involved in childhood asthma through inhibiting ASMCs proliferation, migration, and inflammation via miR-31-5p activity [65][64]. BAZ2B correlates with M2 macrophage activation and inflammation in children with asthma, and positively correlates with the exacerbating progression of diseases [66][65]. Circulating miRNAs such as miR-155-5p and miR-532-5p are predictive of asthma ICS treatment response over time and are significantly associated with changes in dexamethasone-induced trans-repression of NF-κB. Accordingly miR-155-5p and miR-532-5p might be considered as predictive of ICS response in clinical trial [67][66]. MiRNA-155 and Let-7a are differentially expressed in the plasma asthmatics than in control children, and levels well correlate with the degree of asthma severity. MiRNA-155 and let-7a could be used as serological non-invasive biomarkers for diagnosis of asthma and degree of severity [68][67]. Furthermore, it is underlined that circulating miR-146b, miR-206, and miR-720 are predictive of clinical exacerbation in asthmatic children, representing diagnostic biomarkers and therapeutic targets in childhood asthma [69][68] (Figure 3).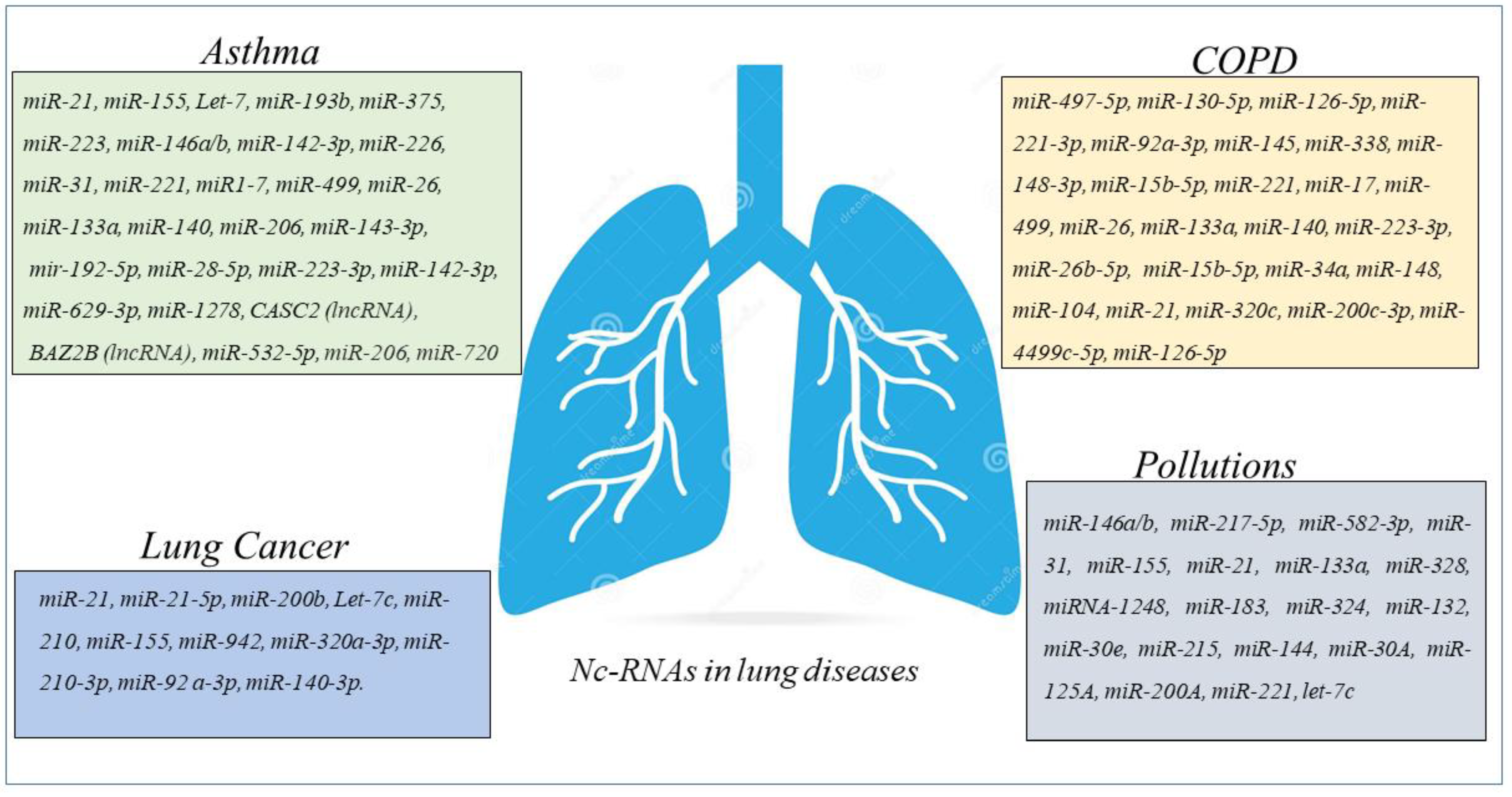
Figure 3. Schematic panel describing nc-RNAs involved in airway diseases and indicated in the revisewarch. The miRNAs and lnc-RNAs are expressed in lung diseases such as asthma, COPD, LC, or in lung diseases associated with environmental pollution.
4. ncRNAs in COPD
Many studies show that miRNAs production is increased in the pathogenesis of COPD [70][69]. MiRNAs involved in the myogenesis (proliferation and differentiation of satellite cells) alleviate the negative impact of skeletal muscle dysfunction and mass loss in COPD regardless of the degree of the airway obstruction [71][70]. miRNA-mRNA regulatory network is identified by GEO2R tool in the circulating plasma of COPD patients. Hub genes are potentially modulated by miR-497-5p, miR-130b-5p, and miR-126-5p and among the top 12 hub genes, MYC and FOXO1 expressions are consistent with that in the GSE56768 dataset [72][71]. Recent studies describe increased levels of miR-221-3p and miR-92a-3p in the serum of COPD patients than in healthy subjects, suggesting that both miR-221-3p and miR-92a-3p might be considered molecular markers to discriminate stable COPD and COPD with acute exacerbations. In addition, the same reseauthorchers underline that miR-221-3p and miR-92a-3p are involved in the description of CSE-induced hyperinflammation of COPD [27][26]. Asthma-COPD overlap syndrome is an inflammatory disease of the airways that describe a new phenotype including both asthma and COPD characteristics. miRNA molecular pathways can help the scientists to better understand the pathophysiological features in many diseases. MiRNA expression profile of serum and sputum supernatants shows the increased expression of miRNA-338 in the sputum supernatants of patients with different obstructive diseases than in peripheral blood, while miRNA-145 increases only in the sputum supernatants of asthmatic subjects. However, both miRNAs are higher in the sputum supernatants of patients with asthma and COPD compared with control subjects. These data describe miRNAs as potential biomarkers in the discrimination of asthma-COPD overlap syndrome, asthma, and COPD [73][72]. The expression of five miRNAs (miR-148a-3p, miR-15b-5p, miR-223-3p, miR-23a-3p, and miR-26b-5p) is lower in patients with asthma-COPD overlap syndrome. Moreover, these miRNAs might be able to discriminate patients with asthma-COPD overlap and patients with either asthma or COPD. Between these miRNAs, miR-15b-5p is the most accurate and associated with the levels of Periostin and chitinase-3-like protein 1 (YKL-40) in the serum of patients representing a potential marker to identify asthma-COPD overlap patients [74][73]. The mechanism of cellular senescence is important to drive pathogenesis of COPD. MiRNA-34a is involved in this cell mechanism and reduces sirtuin-1/6 as markers of senescence through PI3K–mTOR signaling. In this manner its activity reduces secretory phenotype associated with senescence, and reverses cell cycle arrest in epithelial cells from peripheral airways of COPD patients [75][74]. MiRNA data analysis was performed using the TAC software, and reveals 148 miRNAs that are differentially expressed in PBMCs from patients with COPD compared with normal controls. Among the 148 miRNAs, 104 miRNAs are upregulated, and 44 miRNAs are downregulated [76][75]. The data show that miRNAs differentially expressed might be involved in the regulation of cell processes playing a fundamental role in the pathogenesis of COPD. Accordingly, it is possible to think that future investigation in this direction might provide further insight into the mechanism of COPD. The miRNAs analyses show increased levels of miRNA-21 in airway epithelium and lung macrophages of the lungs of mice with CS-induced experimental COPD. miRNA-21 inhibitor (Antago-miR21) reduces the miRNA-21 expression in CS-induced lung of mice, suppressing the infiltration of inflammatory cells (macrophages, neutrophils, and lymphocytes). Furthermore, the treatment of with Antago-miR21 CS-induced mice decreases hysteresis, transpulmonary resistance, and tissue damping improving lung function in the mouse models of COPD [77][76]. Accordingly, it is observed that COPD patients with periodically experience acute exacerbation have increased levels of miR-21 inversely correlated with FEV1. These data support the concept that systemic levels of miR-21 can be involved in the pathogenesis of airway diseases and represent a therapeutic target to control the physiology of the lung [78][77]. In a little cohort of subjects, classified as COPD, smokers, and non-smokers, joint upregulation in miR-320c, miR-200c-3p, and miR-449c-5p levels in the miRNA profiling of BAL samples is detected. These findings might suggest that 3-miRNA signature might be potentially used as biomarkers useful to distinguish COPD patients from smokers and non-smoker subjects [79][78]. The high-throughput RNA sequencing describes a differential expression of 282 mRNAs, 146 lncRNAs, 85 miRNAs, and 81 circRNAs in peripheral blood of COPD patients compared with control. GSEA analysis shows that these differentially expressed RNAs correlate with several critical biological processes such as “ncRNA metabolic process”, “ncRNA processing”, “ribosome biogenesis”, “rRNAs metabolic process”, “tRNA metabolic process”, and “tRNA processing”. All of them might participate in the progression of COPD. These data determine the construction of the lncRNA-mRNA co-expression network, and the constructed circRNA-miRNA-mRNA in COPD opens new perspective in the nc-RNA involvement as potential regulatory roles in COPD [80][79]. lncRNA-proliferation, apoptosis, inflammation, migration, and epithelial-mesenchymal transition (EMT) are cell processes controlled by miRNA-mRNA network. Many lncRNA-miRNA-mRNA are biomarker indicators of comorbidities and may be considered as therapeutic targets for chronic inflammatory diseases of the airways of both COPD and asthma [81][80]. Numerous biological processes are due to the irreversible molecular changes caused by cigarette smoking in COPD patients. Several studies show its direct correlation with the dysregulation of different miRNAs suggesting the diagnostic/prognostic potential of miRNA-based biomarkers and their efficacy as therapeutic targets [82][81] (Figure 3). In conclusion a relevant number of recent studies support the concept about the potential role of miRNAs network in the regulation of different cellular processes, such as proliferation, apoptosis, inflammation, migration, and EMT in COPD patients. These data support the concept of their biological activities in the relevant pathophysiological processes of chronic inflammatory airway diseases. In this scenario, wresearchers comprehensively underline the miRNA network activities in different cell types and their potential roles as biomarkers, indicators of comorbidities, or therapeutic targets for COPD (Figure 3).References
- Dey, S.; Eapen, M.S.; Chia, C.; Gaikwad, A.V.; Wark, P.A.B.; Sohal, S.S. Pathogenesis, Clinical Features of Asthma COPD Overlap, and Therapeutic Modalities. Am. J. Physiol. Lung Cell. Mol. Physiol. 2022, 322, L64–L83.
- Russell, R.J.; Brightling, C. Pathogenesis of Asthma: Implications for Precision Medicine. Clin. Sci. 2017, 131, 1723–1735.
- Zahran, H.S.; Bailey, C.M.; Damon, S.A.; Garbe, P.L.; Breysse, P.N. Vital Signs: Asthma in Children—United States, 2001–2016. MMWR. Morb. Mortal. Wkly. Rep. 2018, 67, 149–155.
- Kwah, J.H.; Peters, A.T. Asthma in Adults: Principles of Treatment. Allergy Asthma Proc. 2019, 40, 396–402.
- Barnes, P.J. Inflammatory Mechanisms in Patients with Chronic Obstructive Pulmonary Disease. J. Allergy Clin. Immunol. 2016, 138, 16–27.
- Barnes, P.J.; Burney, P.G.J.; Silverman, E.K.; Celli, B.R.; Vestbo, J.; Wedzicha, J.A.; Wouters, E.F.M. Chronic Obstructive Pulmonary Disease. Nat. Rev. Dis. Prim. 2015, 1, 15076.
- Negewo, N.A.; Gibson, P.G.; McDonald, V.M. COPD and Its Comorbidities: Impact, Measurement and Mechanisms. Respirology 2015, 20, 1160–1171.
- Mathioudakis, A.G.; Vanfleteren, L.E.G.W.; Lahousse, L.; Higham, A.; Allinson, J.P.; Gotera, C.; Visca, D.; Singh, D.; Spanevello, A. Current Developments and Future Directions in COPD. Eur. Respir. Rev. Off. J. Eur. Respir. Soc. 2020, 29, 200289.
- Hillas, G.; Papaporfyriou, A.; Dimakou, K.; Papaioannou, A.I. Pharmacological Treatment of Stable COPD: Need for a Simplified Approach. Postgrad. Med. 2020, 132, 126–131.
- Alshabanat, A.; Zafari, Z.; Albanyan, O.; Dairi, M.; FitzGerald, J.M. Asthma and COPD Overlap Syndrome (ACOS): A Systematic Review and Meta Analysis. PLoS ONE 2015, 10, e0136065.
- Barnes, P.J.; Adcock, I.M. Chronic Obstructive Pulmonary Disease and Lung Cancer: A Lethal Association. Am. J. Respir. Crit. Care Med. 2011, 184, 866–867.
- Durham, A.L.; Adcock, I.M. The Relationship between COPD and Lung Cancer. Lung Cancer 2015, 90, 121–127.
- Wilson, R.; Anzueto, A.; Miravitlles, M.; Arvis, P.; Haverstock, D.; Trajanovic, M.; Sethi, S. Prognostic Factors for Clinical Failure of Exacerbations in Elderly Outpatients with Moderate-to-Severe COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 10, 985–993.
- Reck, M.; Heigener, D.F.; Mok, T.; Soria, J.-C.; Rabe, K.F. Management of Non-Small-Cell Lung Cancer: Recent Developments. Lancet 2013, 382, 709–719.
- Tubita, V.; Callejas-Díaz, B.; Roca-Ferrer, J.; Marin, C.; Liu, Z.; Wang, D.Y.; Mullol, J. Role of MicroRNAs in Inflammatory Upper Airway Diseases. Allergy 2021, 76, 1967–1980.
- Zhang, P.; Wu, W.; Chen, Q.; Chen, M. Non-Coding RNAs and Their Integrated Networks. J. Integr. Bioinform. 2019, 16.
- Statello, L.; Guo, C.-J.; Chen, L.-L.; Huarte, M. Gene Regulation by Long Non-Coding RNAs and Its Biological Functions. Nat. Rev. Mol. Cell Biol. 2021, 22, 96–118.
- Kopp, F.; Mendell, J.T. Functional Classification and Experimental Dissection of Long Noncoding RNAs. Cell 2018, 172, 393–407.
- Dong, H.; Zhou, J.; Cheng, Y.; Wang, M.; Wang, S.; Xu, H. Biogenesis, Functions, and Role of CircRNAs in Lung Cancer. Cancer Manag. Res. 2021, 13, 6651–6671.
- Fatica, A.; Bozzoni, I. Long Non-Coding RNAs: New Players in Cell Differentiation and Development. Nat. Rev. Genet. 2014, 15, 7–21.
- Maoz, R.; Garfinkel, B.P.; Soreq, H. Alzheimer’s Disease and NcRNAs. Adv. Exp. Med. Biol. 2017, 978, 337–361.
- Zhou, R.; Wu, Y.; Wang, W.; Su, W.; Liu, Y.; Wang, Y.; Fan, C.; Li, X.; Li, G.; Li, Y.; et al. Circular RNAs (CircRNAs) in Cancer. Cancer Lett. 2018, 425, 134–142.
- Zhang, S.-J.; Chen, X.; Li, C.-P.; Li, X.-M.; Liu, C.; Liu, B.-H.; Shan, K.; Jiang, Q.; Zhao, C.; Yan, B. Identification and Characterization of Circular RNAs as a New Class of Putative Biomarkers in Diabetes Retinopathy. Investig. Ophthalmol. Vis. Sci. 2017, 58, 6500–6509.
- Ullah, S.; John, P.; Bhatti, A. MicroRNAs with a Role in Gene Regulation and in Human Diseases. Mol. Biol. Rep. 2014, 41, 225–232.
- Tüfekci, K.U.; Oner, M.G.; Meuwissen, R.L.J.; Genç, S. The Role of MicroRNAs in Human Diseases. Methods Mol. Biol. 2014, 1107, 33–50.
- Shen, Y.; Lu, H.; Song, G. MiR-221-3p and MiR-92a-3p Enhances Smoking-Induced Inflammation in COPD. J. Clin. Lab. Anal. 2021, 35, e23857.
- Li, J.; Chen, R.; Lu, Y.; Zeng, Y. The MicroRNA-1278/SHP-1/STAT3 Pathway Is Involved in Airway Smooth Muscle Cell Proliferation in a Model of Severe Asthma Both Intracellularly and Extracellularly. Mol. Cell. Biochem. 2022, 477, 1439–1451.
- Soni, D.K.; Biswas, R. Role of Non-Coding RNAs in Post-Transcriptional Regulation of Lung Diseases. Front. Genet. 2021, 12, 767348.
- Tanzer, A.; Stadler, P.F. Molecular Evolution of a MicroRNA Cluster. J. Mol. Biol. 2004, 339, 327–335.
- de Rie, D.; Abugessaisa, I.; Alam, T.; Arner, E.; Arner, P.; Ashoor, H.; Åström, G.; Babina, M.; Bertin, N.; Burroughs, A.M.; et al. An Integrated Expression Atlas of MiRNAs and Their Promoters in Human and Mouse. Nat. Biotechnol. 2017, 35, 872–878.
- Alsop, E.; Meechoovet, B.; Kitchen, R.; Sweeney, T.; Beach, T.G.; Serrano, G.E.; Hutchins, E.; Ghiran, I.; Reiman, R.; Syring, M.; et al. A Novel Tissue Atlas and Online Tool for the Interrogation of Small RNA Expression in Human Tissues and Biofluids. Front. Cell Dev. Biol. 2022, 10, 804164.
- Ha, M.; Kim, V.N. Regulation of MicroRNA Biogenesis. Nat. Rev. Mol. Cell Biol. 2014, 15, 509–524.
- Makarova, J.A.; Shkurnikov, M.U.; Wicklein, D.; Lange, T.; Samatov, T.R.; Turchinovich, A.A.; Tonevitsky, A.G. Intracellular and Extracellular MicroRNA: An Update on Localization and Biological Role. Prog. Histochem. Cytochem. 2016, 51, 33–49.
- Munjas, J.; Sopić, M.; Stefanović, A.; Košir, R.; Ninić, A.; Joksić, I.; Antonić, T.; Spasojević-Kalimanovska, V.; Prosenc Zmrzljak, U. Non-Coding RNAs in Preeclampsia-Molecular Mechanisms and Diagnostic Potential. Int. J. Mol. Sci. 2021, 22, 10652.
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of MicroRNA Biogenesis, Mechanisms of Actions, and Circulation. Front. Endocrinol. 2018, 9, 402.
- Fan, R.; Xiao, C.; Wan, X.; Cha, W.; Miao, Y.; Zhou, Y.; Qin, C.; Cui, T.; Su, F.; Shan, X. Small Molecules with Big Roles in MicroRNA Chemical Biology and MicroRNA-Targeted Therapeutics. RNA Biol. 2019, 16, 707–718.
- Zhang, T.; Huang, P.; Qiu, C. Progresses in Epigenetic Studies of Asthma from the Perspective of High-Throughput Analysis Technologies: A Narrative Review. Ann. Transl. Med. 2022, 10, 493.
- Gomez, J.L. Epigenetics in Asthma. Curr. Allergy Asthma Rep. 2019, 19, 56.
- Heffler, E.; Allegra, A.; Pioggia, G.; Picardi, G.; Musolino, C.; Gangemi, S. MicroRNA Profiling in Asthma: Potential Biomarkers and Therapeutic Targets. Am. J. Respir. Cell Mol. Biol. 2017, 57, 642–650.
- Farmanzadeh, A.; Qujeq, D.; Yousefi, T. The Interaction Network of MicroRNAs with Cytokines and Signaling Pathways in Allergic Asthma. MicroRNA 2022, 11, 104–117.
- Wang, X.; Chen, H.; Liu, J.; Gai, L.; Yan, X.; Guo, Z.; Liu, F. Emerging Advances of Non-Coding RNAs and Competitive Endogenous RNA Regulatory Networks in Asthma. Bioengineered 2021, 12, 7820–7836.
- ElKashef, S.M.M.A.E.; Ahmad, S.E.-A.; Soliman, Y.M.A.; Mostafa, M.S. Role of MicroRNA-21 and MicroRNA-155 as Biomarkers for Bronchial Asthma. Innate Immun. 2021, 27, 61–69.
- Specjalski, K.; Niedoszytko, M. MicroRNAs: Future Biomarkers and Targets of Therapy in Asthma? Curr. Opin. Pulm. Med. 2020, 26, 285–292.
- Specjalski, K.; Jassem, E. MicroRNAs: Potential Biomarkers and Targets of Therapy in Allergic Diseases? Arch. Immunol. Ther. Exp. (Warsz). 2019, 67, 213–223.
- Polikepahad, S.; Knight, J.M.; Naghavi, A.O.; Oplt, T.; Creighton, C.J.; Shaw, C.; Benham, A.L.; Kim, J.; Soibam, B.; Harris, R.A.; et al. Proinflammatory Role for Let-7 MicroRNAS in Experimental Asthma. J. Biol. Chem. 2010, 285, 30139–30149.
- Lu, T.X.; Hartner, J.; Lim, E.-J.; Fabry, V.; Mingler, M.K.; Cole, E.T.; Orkin, S.H.; Aronow, B.J.; Rothenberg, M.E. MicroRNA-21 Limits in Vivo Immune Response-Mediated Activation of the IL-12/IFN-Gamma Pathway, Th1 Polarization, and the Severity of Delayed-Type Hypersensitivity. J. Immunol. 2011, 187, 3362–3373.
- Dong, J.; Sun, D.; Lu, F. Association of Two Polymorphisms of MiRNA-146a Rs2910164 (G > C) and MiRNA-499 Rs3746444 (T > C) with Asthma: A Meta-Analysis. J. Asthma Off. J. Assoc. Care Asthma 2021, 58, 995–1002.
- Shi, Z.-G.; Sun, Y.; Wang, K.-S.; Jia, J.-D.; Yang, J.; Li, Y.-N. Effects of MiR-26a/MiR-146a/MiR-31 on Airway Inflammation of Asthma Mice and Asthma Children. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 5432–5440.
- Gagliardo, R.; Ferrante, G.; Fasola, S.; Di Vincenzo, S.; Pace, E.; La Grutta, S. Resolvin D1 and MiR-146a Are Independent Distinctive Parameters in Children with Moderate and Severe Asthma. Clin. Exp. Allergy J. Br. Soc. Allergy Clin. Immunol. 2021, 51, 350–353.
- Marques-Rocha, J.L.; Samblas, M.; Milagro, F.I.; Bressan, J.; Martínez, J.A.; Marti, A. Noncoding RNAs, Cytokines, and Inflammation-Related Diseases. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2015, 29, 3595–3611.
- Martinez-Nunez, R.T.; Louafi, F.; Sanchez-Elsner, T. The Interleukin 13 (IL-13) Pathway in Human Macrophages Is Modulated by MicroRNA-155 via Direct Targeting of Interleukin 13 Receptor Alpha1 (IL13Ralpha1). J. Biol. Chem. 2011, 286, 1786–1794.
- Malmhäll, C.; Alawieh, S.; Lu, Y.; Sjöstrand, M.; Bossios, A.; Eldh, M.; Rådinger, M. MicroRNA-155 Is Essential for T(H)2-Mediated Allergen-Induced Eosinophilic Inflammation in the Lung. J. Allergy Clin. Immunol. 2014, 133, 1429–1438.e7.
- Mayoral, R.J.; Deho, L.; Rusca, N.; Bartonicek, N.; Saini, H.K.; Enright, A.J.; Monticelli, S. MiR-221 Influences Effector Functions and Actin Cytoskeleton in Mast Cells. PLoS ONE 2011, 6, e26133.
- Yao, Y.; Chen, C.-L.; Yu, D.; Liu, Z. Roles of Follicular Helper and Regulatory T Cells in Allergic Diseases and Allergen Immunotherapy. Allergy 2021, 76, 456–470.
- Yang, H.-Y.; Barbi, J.; Wu, C.-Y.; Zheng, Y.; Vignali, P.D.A.; Wu, X.; Tao, J.-H.; Park, B.V.; Bandara, S.; Novack, L.; et al. MiR-17 Resulted in Enhanced Suppressive Activity. Ectopic of Genes Encoding Effector Cytokines. Thus, MiR-17 Provides a Potent Layer of Treg Cell Control Expression of MiR-17 Imparted Effector-T-Cell-like Characteristics to Treg Cells via the de-repression. Immunity 2016, 45, 83–93.
- Johansson, K.; Malmhäll, C.; Ramos-Ramírez, P.; Rådinger, M. MicroRNA-155 Is a Critical Regulator of Type 2 Innate Lymphoid Cells and IL-33 Signaling in Experimental Models of Allergic Airway Inflammation. J. Allergy Clin. Immunol. 2017, 139, 1007–1016.e9.
- Cheng, W.; Yan, K.; Xie, L.Y.; Chen, F.; Yu, H.C.; Huang, Y.X.; Dang, C.X. MiR-143-3p Controls TGF-Β1-Induced Cell Proliferation and Extracellular Matrix Production in Airway Smooth Muscle via Negative Regulation of the Nuclear Factor of Activated T Cells 1. Mol. Immunol. 2016, 78, 133–139.
- Lou, L.; Tian, M.; Chang, J.; Li, F.; Zhang, G. MiRNA-192-5p Attenuates Airway Remodeling and Autophagy in Asthma by Targeting MMP-16 and ATG7. Biomed. Pharmacother. 2020, 122, 109692.
- Maneechotesuwan, K. Role of MicroRNA in Severe Asthma. Respir. Investig. 2019, 57, 9–19.
- Perry, M.M.; Baker, J.E.; Gibeon, D.S.; Adcock, I.M.; Chung, K.F. Airway Smooth Muscle Hyperproliferation Is Regulated by MicroRNA-221 in Severe Asthma. Am. J. Respir. Cell Mol. Biol. 2014, 50, 7–17.
- Tsitsiou, E.; Williams, A.E.; Moschos, S.A.; Patel, K.; Rossios, C.; Jiang, X.; Adams, O.-D.; Macedo, P.; Booton, R.; Gibeon, D.; et al. Transcriptome Analysis Shows Activation of Circulating CD8+ T Cells in Patients with Severe Asthma. J. Allergy Clin. Immunol. 2012, 129, 95–103.
- Maes, T.; Cobos, F.A.; Schleich, F.; Sorbello, V.; Henket, M.; De Preter, K.; Bracke, K.R.; Conickx, G.; Mesnil, C.; Vandesompele, J.; et al. Asthma Inflammatory Phenotypes Show Differential MicroRNA Expression in Sputum. J. Allergy Clin. Immunol. 2016, 137, 1433–1446.
- Kyyaly, M.A.; Sanchez-Elsner, T.; He, P.; Sones, C.L.; Arshad, S.H.; Kurukulaaratchy, R.J. Circulating MiRNAs-A Potential Tool to Identify Severe Asthma Risk? Clin. Transl. Allergy 2021, 11, e12040.
- Yang, Y.; Sun, Z.; Ren, T.; Lei, W. Differential Expression of LncRNA CASC2 in the Serum of Childhood Asthma and Its Role in Airway Smooth Muscle Cells Proliferation and Migration. J. Asthma Allergy 2022, 15, 197–207.
- Xia, L.; Wang, X.; Liu, L.; Fu, J.; Xiao, W.; Liang, Q.; Han, X.; Huang, S.; Sun, L.; Gao, Y.; et al. Lnc-BAZ2B Promotes M2 Macrophage Activation and Inflammation in Children with Asthma through Stabilizing BAZ2B Pre-MRNA. J. Allergy Clin. Immunol. 2021, 147, 921–932.e9.
- Li, J.; Panganiban, R.; Kho, A.T.; McGeachie, M.J.; Farnam, L.; Chase, R.P.; Weiss, S.T.; Lu, Q.; Tantisira, K.G. Circulating MicroRNAs and Treatment Response in Childhood Asthma. Am. J. Respir. Crit. Care Med. 2020, 202, 65–72.
- Karam, R.A.; Abd Elrahman, D.M. Differential Expression of MiR-155 and Let-7a in the Plasma of Childhood Asthma: Potential Biomarkers for Diagnosis and Severity. Clin. Biochem. 2019, 68, 30–36.
- Kho, A.T.; McGeachie, M.J.; Moore, K.G.; Sylvia, J.M.; Weiss, S.T.; Tantisira, K.G. Circulating MicroRNAs and Prediction of Asthma Exacerbation in Childhood Asthma. Respir. Res. 2018, 19, 128.
- Zhuang, Y.; Hobbs, B.D.; Hersh, C.P.; Kechris, K. Identifying MiRNA-MRNA Networks Associated With COPD Phenotypes. Front. Genet. 2021, 12, 748356.
- Barreiro, E. The Role of MicroRNAs in COPD Muscle Dysfunction and Mass Loss: Implications on the Clinic. Expert Rev. Respir. Med. 2016, 10, 1011–1022.
- Zhu, M.; Ye, M.; Wang, J.; Ye, L.; Jin, M. Construction of Potential MiRNA-MRNA Regulatory Network in COPD Plasma by Bioinformatics Analysis. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 2135–2145.
- Lacedonia, D.; Palladino, G.P.; Foschino-Barbaro, M.P.; Scioscia, G.; Carpagnano, G.E. Expression Profiling of MiRNA-145 and MiRNA-338 in Serum and Sputum of Patients with COPD, Asthma, and Asthma-COPD Overlap Syndrome Phenotype. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1811.
- Hirai, K.; Shirai, T.; Shimoshikiryo, T.; Ueda, M.; Gon, Y.; Maruoka, S.; Itoh, K. Circulating MicroRNA-15b-5p as a Biomarker for Asthma-COPD Overlap. Allergy 2021, 76, 766–774.
- Barnes, P.J.; Baker, J.; Donnelly, L.E. Cellular Senescence as a Mechanism and Target in Chronic Lung Diseases. Am. J. Respir. Crit. Care Med. 2019, 200, 556–564.
- Wang, L.; Zhao, H.; Raman, I.; Yan, M.; Chen, Q.; Li, Q.-Z. Peripheral Blood Mononuclear Cell Gene Expression in Chronic Obstructive Pulmonary Disease: MiRNA and MRNA Regulation. J. Inflamm. Res. 2022, 15, 2167–2180.
- Kim, R.Y.; Sunkara, K.P.; Bracke, K.R.; Jarnicki, A.G.; Donovan, C.; Hsu, A.C.; Ieni, A.; Beckett, E.L.; Galvão, I.; Wijnant, S.; et al. A MicroRNA-21-Mediated SATB1/S100A9/NF-ΚB Axis Promotes Chronic Obstructive Pulmonary Disease Pathogenesis. Sci. Transl. Med. 2021, 13, eaav7223.
- Ferraro, M.; Di Vincenzo, S.; Sangiorgi, C.; Leto Barone, S.; Gangemi, S.; Lanata, L.; Pace, E. Carbocysteine Modifies Circulating MiR-21, IL-8, SRAGE, and FAGEs Levels in Mild Acute Exacerbated COPD Patients: A Pilot Study. Pharmaceuticals 2022, 15, 218.
- Cerón-Pisa, N.; Iglesias, A.; Shafiek, H.; Martín-Medina, A.; Esteva-Socias, M.; Muncunill, J.; Fleischer, A.; Verdú, J.; Cosío, B.G.; Sauleda, J. Hsa-Mir-320c, Hsa-Mir-200c-3p, and Hsa-Mir-449c-5p as Potential Specific MiRNA Biomarkers of COPD: A Pilot Study. Pathophysiol. Off. J. Int. Soc. Pathophysiol. 2022, 29, 143–156.
- Liu, P.; Wang, Y.; Zhang, N.; Zhao, X.; Li, R.; Wang, Y.; Chen, C.; Wang, D.; Zhang, X.; Chen, L.; et al. Comprehensive Identification of RNA Transcripts and Construction of RNA Network in Chronic Obstructive Pulmonary Disease. Respir. Res. 2022, 23, 154.
- Qiao, X.; Hou, G.; He, Y.-L.; Song, D.-F.; An, Y.; Altawil, A.; Zhou, X.-M.; Wang, Q.-Y.; Kang, J.; Yin, Y. The Novel Regulatory Role of the LncRNA-MiRNA-MRNA Axis in Chronic Inflammatory Airway Diseases. Front. Mol. Biosci. 2022, 9, 927549.
- Paul, S.; Ruiz-Manriquez, L.M.; Ambriz-Gonzalez, H.; Medina-Gomez, D.; Valenzuela-Coronado, E.; Moreno-Gomez, P.; Pathak, S.; Chakraborty, S.; Srivastava, A. Impact of Smoking-Induced Dysregulated Human MiRNAs in Chronic Disease Development and Their Potential Use in Prognostic and Therapeutic Purposes. J. Biochem. Mol. Toxicol. 2022, 36, e23134.
More