Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Mathumalar Loganathan Fahrni and Version 2 by Conner Chen.
The monkeypox disease is a zoonotic-infectious disease that transmits between animals and humans. It is caused by a double-stranded DNA virus belonging to the Orthopoxvirus genus that is closely related to the variola virus –the causative agent of smallpox.
- monkeypox
- outbreak
- diagnostics
- infectious diseases
1. Background
Monkeypox (MPX) is a rare zoonotic disease caused by the Monkeypox virus (MPXV), a double-stranded DNA virus belonging to the Orthopoxvirus genus. MPX is endemic to Western and Central Africa. MPXV is closely related to the variola virus, the causative agent of smallpox. In the past 20 years, deforestation, population development, encroachment on animal habitats, more human migration, and increased global interconnectedness may have led to MPXV expansion to fill the ecological niche once occupied by the closely related smallpox virus [1][2][3][1,2,3]. The World Health Organization (WHO) deemed the risk to global public health posed by the multi-country monkeypox outbreak in non-endemic countries to be “moderate” on 29 May 2022 [4]. Since then, however, monkeypox is classified as a High Consequence Infectious Disease (HCID) in the UK (https://www.gov.uk/guidance/high-consequence-infectious-diseases-hcid, accessed on 7 November 2022). On 23 July 2022, WHO declared the ongoing global monkeypox outbreak a Public Health Emergency of International Concern (PHEIC), and it is the second time in two years that the WHO has taken the extraordinary step of declaring a global emergency. There is an urgent need for instant access to clear, succinct, fact-based information as monkeypox is mostly unknown to medical professionals especially to front-line healthcare personnel in prehospital, emergency departments, hospitals, and acute care/sexual transmitted illness clinics [5]. To distinguish the current outbreak from recurrent local cases in known enzootic regions, a new nomenclature has been proposed [6], with the Congo Basin lineage as clade 1, the West African lineage as clade 2, and the clade 2 (clade 2a and clade 2b) variants are the main ones circulating in the current global outbreak. The changing epidemiology of human monkeypox presents its own challenges. However, what is known is that immunocompromised patients are more susceptible to the disease. Because monkeypox resembles smallpox, antiretroviral therapy, although it has limitations for use in the former at present, may shed some light on decelerating disease progression, particularly in immunosuppressed individuals.
2. History of Monkeypox
The virologist, Preben Christian Alexander von Magnus, discovered and named monkeypox in 1958 in Denmark while investigating two smallpox-like disease epidemics that happened in laboratory monkey (Cynomolgus) colonies [7] whose phylogenetic data revealed that it was from the West-African Clade [8]. However, some researchers have proposed that MPXV might be evolved before 1958, the year of its discovery in Denmark [9][10][9,10]. In September 1970, a 9-month-old child, who was admitted for suspected smallpox to the Basankusu Hospital in the Republic of the Congo (nowadays known as the Democratic Republic of the Congo; DRC), is considered the first known human MPX case [11]. Then, human MPXV cases were discovered in Liberia, Sierra Leone, and Nigeria [12][13][12,13]. Numerous subsequent outbreaks of human monkeypox have often been recorded in Equatorial Africa, particularly in the DRC and Nigeria [14][15][16][14,15,16]. The Central-African (Congo Basin) and Western-African clades are the two clades that currently exist. In 2003, the first monkeypox outbreak outside of Africa originated in West Africa (Ghana) and occurred in the United States. All cases resulted from contact with sick prairie dogs without reported human-to-human transmission [17] (Table 1).
Table 1.
Timeline of Monkeypox virus-related events.
| Year | Event | References |
|---|---|---|
| 3500 years ago | Separation of MPXV within Old World Orthopoxviruses took place. | [18] |
| 600 years ago | MPXV West African subtype appeared | [18][19][18,19] |
| 1899 | Identification of MPXV in five species of African rope squirrel (Funisciurus sp.) collected across Central Africa. | [20] |
| 1958 | MPXV was first identified in Denmark following an outbreak of the pustular disease in a macaque colony (cynomolgus monkeys). The macaques had been imported from Singapore. | [7] |
| 1959–1964 | MPXV, which was reported among colonies of captive monkeys, were also described in the USA (1959 and 1962) and Rotterdam Zoo, the Netherlands (1964). | [21] |
| 1970 1972 |
The first human monkeypox case was identified in the Democratic Republic of Congo (DRC, then Zaire). | [11] |
| 1970–1979 | A reported outbreak of human MPXV in Nigeria. | [1][22][1,22] |
| 1980 | Vaccination laid the basis for the eradication of Variola (genetically related to MPXV) | [23] |
| 1996–1997 | A major outbreak of human monkeypox occurred in Katako-Combe, Zaire (DRC). A total of 73% of cases reported contact with another human case while 27% had known contact with a wild animal. | [24] |
| 2003 | An outbreak of human monkeypox occurred in the USA (more than 71 infected people). It was initiated by rodents (small mammals) imported from Ghana to be sold as exotic pets and have been transmitted by pet prairie (Cynomys spp.). These infected mammals were kept near prairie dogs that were later sold as pets. | [25] |
| 2017 | The largest West-African monkeypox outbreak began in September 2017 in Nigeria following very heavy rainfall and flooding. Active surveillance confirmed human monkeypox, and as of September 2019, a total of 176 human-monkeypox cases had been confirmed from 18 states. | [15][26][15,26] |
| 2018 | Four individuals traveling from Nigeria to the United Kingdom (UK) (n = 2; travel from Nigeria, bush meat possible for one case—Secondary Exposure during healthcare), Israel (n = 1; rodent carcasses in Nigeria), and Singapore (n = 1; travel to Nigeria and attended a wedding and eat bushmeat) became the first human-monkeypox cases exported from Africa and a related nosocomial-transmission event in the UK became the first confirmed human-to-human monkeypox transmission event outside of Africa. This explains the role travelers play in the spread of infectious-disease epidemics in new regions globally. | [27][28][29][27,28,29] |
| 2019 | A further case of human monkeypox was confirmed in the UK, again imported from Nigeria. Contact tracing was initiated and the smallpox vaccine (Imvanex) was procured. In 2019, a Nigerian travelling to Singapore for a training course developed skin lesions shortly after arrival and was diagnosed with human monkeypox. | [24][27][24,27] |
| 2021 | Reported human-monkeypox cases in the UK. Another case was reported in a returning traveler from Nigeria to Maryland, and another case in Texas in the USA. |
[30] |
| 2022 | MPXV outbreak outside Africa starting from UK in early May 2022 MPXV outbreak in Africa in endemic and non-endemic African countries |
[31] |
3. Pathogenesis and Infection Mechanism
The nasopharynx, or oropharynx, along with subcutaneous portals, can be exploited by the MPXV to infect its host. MPXV multiplies at the entry site before spreading to nearby lymph nodes. The virus spreads to certain other organ systems after an early phase of virus infection. MPXV resembles other-recognized Orthopoxviruses in terms of appearance. The outer membrane of MPXVs, which are oval or brick-shaped, is made of lipoproteins [1]. Despite being a DNA virus, the MPXV completes its life cycle in the cytoplasm. During viral DNA replication, transcription, and virion packaging, a number of proteins are necessary [32][57]. MPXV can enter or penetrate the host cell through fusion and macropinocytosis [33][34][58,59]. The occurrence of two separate viral types, intracellular mature virus (IMV) and extracellular enveloped virus (EEV), which are enclosed by various different lipid membranes and also exhibit specific surface proteins, complicates the entrance and release of MPXV [35][60] (Figure 12). Additionally, the Congo clade of the MPXV might differ from the West African clade as the Congo clade exhibit more virulence and pathogenicity [36][61].
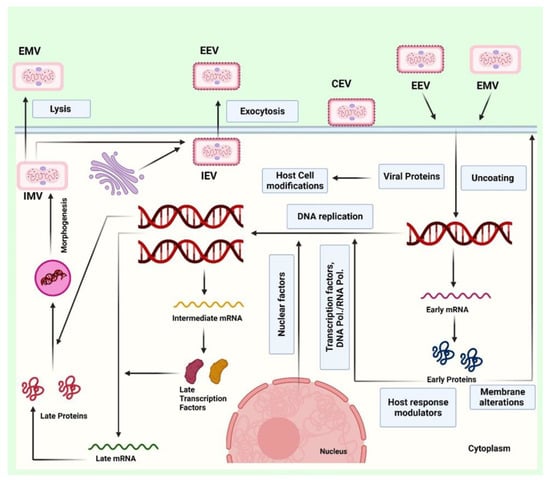
Figure 12. The figure represents the infection mechanism by which extracellular mature virion (EMV) or extracellular enveloped virus (EEV) infect the human cell and hijack the host machinery. The viral particles enter or penetrate the host cell through fusion and macropinocytosis, then replicate and infect the host cells. The genetic material replicates in the host cell and transcribes to produce the viral proteins with the help of host translation proteins. The genetic material and the viral proteins assemble in the host cell and are lysed through exocytosis. The assembled viral particles excytosed in the form of EMV and EEV.
After the DNA replication, transcription, and translation events in the host cytoplasm, IMVs are formed within the cytoplasm. Additionally, enclosed viruses can finish viral assembly by budding through the plasma membrane in the form of EEV. IMV becomes EEV via encapsulation by intracellular membranes and is carried to the cell surface on microtubules and exposed on the cell surface via exocytosis, or they are released upon cell lysis (Figure 12). Furthermore, the enveloped virion is known as a cell-associated enveloped virus (CEV) if it stays affixed to the cell surface. CEV spreads into neighboring cells by developing actin tails below the plasma membrane. A different option is to release the surface virion as EEV [35][37][38][60,62,63], which can further infect the neighboring cells.
According to the serological analysis of cytokine responses to human MPXV infection, human-monkeypox illness is thought to be accompanied by a cytokine storm. Following MPXV infection, researchers also discovered indications of a strong T helper 2 (Th2) response and a weakened Th1 response. IL-4 (and the related IL-13), IL-5, and IL-6 levels were increased above the normal human range, while IL-10 levels were high in severe instances. These cytokines are linked with Th2-mediated immune response. Tumor necrosis factor-alpha (TNF-alpha), interferon-alpha (IFN-alpha), interferon-gamma (IFN-gamma), and IL-2 were shown to have lower serum concentrations [39][64]. Hence, the dysregulation in the Th1-mediated immune response can be associated with the severity of the infection. It is interesting to note that the generation of inflammatory cytokines is suppressed in the human cells that have already contracted the monkeypox virus.
4. Diagnostic Management
If a person exhibits the aforementioned symptoms, monkeypox may be suspected, especially if that person has a history of contact or travel to monkeypox-endemic regions. Once clinical suspicion exists, diagnostic evaluation of monkeypox should be initiated (Figure 23). Importantly, diagnosis of the monkeypox during the current outbreak differs from what is mentioned in the classic descriptions in the West African region due to atypical transmission, sustained human-to-human transmission, and history of sexual contact. Therefore, even if the rash is localized and not (yet) extensive, monkeypox should be considered in the differential diagnosis when a patient appears with STI-associated or STI-like rash [40][74] and also when evaluating genital-ulcer diseases [41][75]. Monkeypox and varicella (chickenpox) are sometimes mistaken in countries where these infections are prevalent.
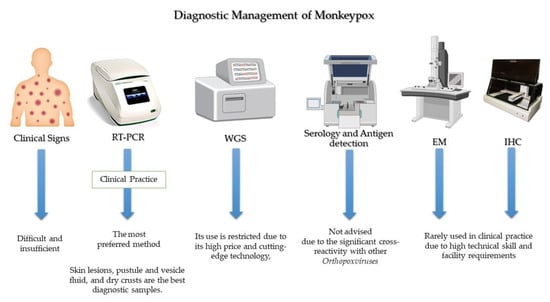
Figure 23.
General lines for diagnosis of monkeypox.
Based on clinical diagnosis, the detection of monkeypox may be misdiagnosed with some sexually transmitted infections (STIs), such as syphilis, herpes simplex, and disseminated-gonococcal infection. Further, monkeypox is most easily recognized by its propensity to cause moderate to severe lymphadenopathy. Typically, monkeypox cannot be clinically distinguished from other pox-like viruses, such as varicella, herpes zoster, measles, and arboviruses (Dengue, Zika and chikungunya), making a diagnosis based only on clinical observation difficult and insufficient. Therefore, it could not be used as a fast-track infection control strategy. Hence, nucleic-acid-amplification testing for the monkeypox virus from vesicles or genital lesions using real-time or conventional real-time polymerase chain reaction (RT-PCR) is used to confirm the diagnosis because of its high accuracy and sensitivity approaching 100%.
The diagnosis of human MPX is made on the basis of a clinical suspicion backed by typical skin and mucosal lesions, which is then verified by molecular testing [42][76]. The preferred strategy for diagnosing an active monkeypox case is the identification of viral DNA in swabs taken from crusts of vesicles or ulcers [43][77]. The RT-PCR assays target various Orthopoxvirus genes. DNA polymerase (E9L) and envelope protein (B6R), two distinct viral gene targets used in combination, showed 100% specificity for monkeypox in RT-PCR assays. This finding suggests that using two distinct viral-gene targets in combination could provide a reliable and sensitive method for rapid diagnosis [44][78].
Numerous types of skin lesions, including as macular, pustular, vesicular, and crusted lesions, as well as lesions in various stages that manifest at the same time, have been linked to MPX [45][46][79,80]. For monkeypox diagnostic tests, skin lesions, pustule and vesicle fluid, and dry crusts are the best diagnostic samples. Sterile-dry polyester, nylon, or Dacron swabs can be used to acquire two swab specimens from a minimum of three lesions. In samples of lesion crusts, dry lesion swabs in viral-transport media (VTM) are allowed [47][81].
The Center for Disease Control and Prevention (CDC) advises clinicians to obtain two specimens for each patient to make an accurate diagnosis. Each sample should be collected from multiple lesions, ideally from several different body sites [48][82]. The FDA advises clinicians to swab the lesion since blood and saliva could produce inaccurate results [49][83] because monkeypox virus remains in blood for only a short period of time. Samples of urine, semen, rectal fluid, and/or genital tissue may also be collected, depending on the clinic.
Within an hour after collection, specimens should be refrigerated (2–8 °C) or frozen (−20 °C or lower), and they should be brought as quickly as possible to the lab. Samples should be stored for a longer period of time at 70 °C and repeated freeze-thaw cycles should be avoided. When a cold chain is not readily available, viral DNA from skin-lesion material can be considered since it is relatively stable when stored in a dark, cool environment [50][84]. For the time being, testing for monkeypox continues to be heavily concentrated in facilities with qualified staff mainly handling the specimens in Biosafety Level 2 (BSL-2) facilities.
Diagnosis of monkeypox starts with suspicion in cases suffering from pox-like lesions and a history of contact or travel to monkeypox-endemic regions. However, PCR is the preferred method to confirm the diagnosis. Whole-genome sequencing (WGS) is the gold standard for characterizing the monkeypox virus, but its use is restricted, particularly in developing countries. Low blood urea nitrogen (BUN), increased transaminase levels, hypoalbuminemia, leukocytosis, and thrombocytopenia are some of the laboratory findings reported in monkeypox. The methods of serology and antigen detection are not advised because it is insufficiently specific due to the significant cross-reactivity with other Orthopoxviruses [51][52][85,86]. Additionally, immunohistochemical (IHC) staining for Orthopoxvirus antigens and visualization on electron microscopy (EM) are among diagnostic methods [53][87]; however, they are rarely used in clinical practice due to high technical skills and facility requirements. Monkeypox culture-based testing should not be done frequently in diagnostic or clinical laboratories [48][82].
Additional TaqMan probe-based RT-PCR assays have been described as a generic monkeypox assay that targets both monkeypox clades [54][88]. But its access remains limited. Li et al. [55][89] developed Cepheid GeneXpert (a self-contained cartridge) to provide an alternative to traditional PCR detection methods. Regardless of the type of specimen obtained (crust versus vesicular swab), the GeneXpert assay demonstrated high sensitivity, specificity, negative predictive value, and positive predictive value in suspicious specimens [55][89], but it requires high costs. Chelsky et al. [56][90] validated a direct RT-PCR protocol for monkeypox viral identification to increase the scalability of monkeypox testing. The test eliminates the need for nucleic acid extraction kits, cuts down on lab tech time per sample, and reduces exposure to an infectious agent while maintaining the sensitivity and accuracy of the indirect assay.
The gold standard for characterizing monkeypox virus and other Orthopoxviruses is the next-generation WGS methods. Because of its high price and cutting-edge technology, its use is restricted, particularly in developing countries.
Quality services to the public can be provided with documented guidelines for collecting and forwarding biological materials. Integrating monkeypox screening into routine surveillance systems is now indispensable. Varicella, herpes simplex, and syphilis could lead to misdiagnosis because these conditions can mimic monkeypox in pregnant women. Additionally, there is a need for developing diagnostics home-based test kits.
5. Therapeutics and Vaccination
The mainstay of clinical management for typical a MPX infection is supportive and symptomatic treatment [57][95]. Limiting non-steroidal anti-inflammatory drugs (NSAIDs) is reasonable due to the concern of developing hemorrhagic lesions [58][96]. Currently, there are no specific treatments for monkeypox disease; however, experience with smallpox suggests that the vaccinia vaccine, cidofovir, tecovirimat, and vaccinia immune globulin (IVG) may have a use in monkeypox treatment [59][97]. As per the WHO guidelines, tecovirimat was developed for smallpox and was licensed by the European Medicines Agency (EMA) for monkeypox in 2022. Current antivirals, tecovirimat, brincidofovir, cidofovir, and vaccinia immune globulin intravenous (VIGIV), which are approved for smallpox infection, can also be used for monkeypox treatment, which could potentially outweigh their harm to those with severe diseases or poor prognosis, such as immunocompromised patients, pediatrics, pregnant and breastfeeding women, complicated lesions, and when lesions appear near the mouth, eyes, and genitals [60][98]. Stability testing and safe- dosing studies for these antiretrovirals have been conducted in humans, but evidence for their efficacy is limited [60][98].
A clean fluid composed up of highly concentrated IgG antibody against the vaccinia virus that were obtained from healthy individuals who had previously received a vaccination against the live vaccinia virus is known as vaccine immune globulin (VIG) [61][99]. The CDC permits the use of VIG to treat an epidemic of MPX. The treatment of Orthopoxvirus infection with VIGIV was documented in many investigations [62][63][100,101]. However, there is no information on how well VIG works to treat MPXV infection. In serious situations, doctors could think about utilizing it. In those cases with a severe impairment in T cell functioning, for whom smallpox immunization is contraindicated following exposure to MPXV, the VIG is also appropriate for preventive usage [64][102].
The CDC-held Emergency Access Investigational New Protocol allows the use of tecovirimat for non-variola Orthopoxvirus infections, such as MPX. The protocol also includes an allowance for opening an oral capsule and mixing its content with liquid or soft food for pediatric patients weighing less than 13 kg. Tecovirimat (orally, 600 mg BD for 2 weeks) is available through the Strategic National Stockpile as an oral-capsule formulation or an intravenous vial. Tecovirimat (formerly ST-246, with the trade name TPOXX®) inhibits the highly conserved p37 Orthopoxvirus protein responsible for the development of virions, inhibiting the spread of the virus within an infected host [65][103]. It is indicated for the treatment of smallpox in adults and pediatric patients weighing at least 3 kg. Tecovirimat has demonstrated efficacy against smallpox in both human and animal models [66][104]. Despite the fact that its effectiveness against monkeypox in humans has not been proven, investigations on animals treated with tecovirimat at various phases of the disease have shown better survival from lethal monkeypox-virus infections, compared to animals treated with placebo [66][67][104,105]. Tecovirimat was initially authorized in oral form in 2018; an IV formulation was authorized in 2022. Dual therapy may be used in severe diseases where brincidofovir is added. Both tecovirimat and brincidofovir are available in the Strategic National Stockpile. The European Medicines Agency has approved tecovirimat for monkeypox. Tecovirimat and vaccinia-immune globulin can be considered for treating pregnant women who are severely ill [68][72].
Cidofovir, the nucleotide analog, can inhibit the progression of both smallpox and monkeypox [69][106]. As of 6 June 2022, the US FDA has not given cidofovir approval to cure monkeypox. Since there is an outbreak, cidofovir may be administered under the proper regulatory authority, such as an IND procedure or an emergency use authorization (EUA). Intravenous-normal saline and probenicid therapy must be given concurrently with cidofovir. Brincidofovir has been approved for the treatment of smallpox in the US since June 2021. Brincidofovir (oral) is an analog of the intravenous-drug cidofovir, and may have an improved safety profile, namely less renal toxicity, compared to cidofovir [70][107]. These drugs work by inhibiting the viral DNA polymerase [71][108].
Based on the clinical presentation and other diagnostic information, clinicians should weigh the risks and advantages of starting a particular treatment. Compared with adults, paediatric patients suffer from more severe diseases and higher mortality. Challenges for managing them are unique and warrant a careful multidisciplinary approach. Safety and dosing of the different antiviral agents are still not confirmed for paediatric patients [72][109]. Because Tecovirimat has no embryotoxic and teratogenic effects detected in animal studies. Additionally, the US Centers for Disease Control and Prevention allow the use of the live-smallpox vaccination ACAM2000 in emergency situations, which provides 85% cross-protective immunity against monkeypox. However, ACAM2000 has a rare risk represented in preterm delivery, stillbirth, neonatal death, and potential adverse maternal reactions. The third-generation smallpox vaccination MVA-BN, which was recently licensed in the USA, Canada, and the EU, may be safer because it contains a virus that cannot replicate and has not been shown to cause problems during pregnancy [68][72].
The smallpox vaccine has been reported to provide 85% cross protection against Monkeypox. Moreover, in the 1980s, contact tracing of monkeypox cases revealed an overall attack rate of 7.2% and 0.9% for contacts unvaccinated versus those vaccinated, respectively. Additionally, ring vaccination i.e., vaccinating close contacts of confirmed cases can be successful if infectious cases are promptly diagnosed. The benefits of ring vaccination are double-fold: it can break the chain of virus transmission and bring to a halt the course of a severe disease [73][110]. With fading immunity among populations and non-availability of first generation smallpox vaccine for the public, newer generation vaccines have been developed. ACAM2000 and MVA-BN (modified vaccinia Ankara-Bavarian Nordic) are two vaccines licensed for use in the USA. MVA-BN is specifically developed for Monkeypox and is a live, non-replicating vaccine based on modified vaccinia Ankara, a live attenuated form of vaccinia virus. It is available in the US as Jynneos, in Europe under the brand name Imvanex, and Imvamune in Canada [74][111]. Modified vaccinia Ankara (MVA) is available as a third-generation smallpox vaccine [75][112]. MVA-BN (IMVANEX/IMVAMUNE/JYNNEOSTM) stain has been licensed in multiple countries for protection from smallpox or monkeypox. In non-human primate studies, two doses of MVA-BN provided 100% protection against a lethal challenge of aerosolized monkeypox [76][113]. MVA-BN® can also be considered for post-exposure prophylaxis in selected patients, ideally within 4 days of high-grade exposure [77][114]. As live vaccines are contraindicated in immunocompromised patients, vaccinia immunoglobulin may be considered, although data on its effectiveness are unclear [78][65]. The CDC recommends vaccination within four days of exposure to prevent disease or up to 14 days after exposure to reduce the severity of the disease. More than 36,000 doses of the JYNNEOS vaccine are currently in the US Strategic National Stockpile. Although the CDC has recommended that the JYNNEOS vaccine be offered to close contacts of patients with monkeypox, this vaccine is currently not easy to access.
In the USA, the currently approved vaccines include ACAM2000, the purified clone of the Dryvax vaccine by Sanofi, and the modified vaccinia Ankara by Bavarian Nordic (JYNNEOSTM in the USA, IMVANEXTM in Europe, IMVAMUNETM in Canada). JYNNEOSTM is FDA-approved for both smallpox and monkeypox, and the USA Strategic National Stockpile contains both JYNNEOSTM and ACAM2000. The immunocompromised and those with atopic dermatitis should not be vaccinated with a second-generation vaccine, such as ACAM2000, but can receive a third-generation vaccine, such as JYNNEOSTM/IMVANEX/IMVAMUNE.