Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Kyu-ho Yi and Version 2 by Amina Yu.
The platysma muscle is a thin superficial muscle that covers the entire neck and lower part of the face. The platysma muscle is the primary target muscle for botulinum neurotoxin injection therapy aimed at treating platysmal band and lower facial lifting. In the procedure of botulinum neurotoxin injection therapy, a lack of knowledge of the anatomy of the platysma muscle and the properties of botulinum neurotoxin can lead to side effects such as dysphagia, dysphonia, and weakness of the neck muscles. Anatomically safe injection sites have been proposed for the platysma muscle, and the appropriate injection technique has been reviewed.
- botulinum neurotoxin
- platysma band
- platysma muscle
- dermotoxin
- injection point
- face lifting
1. Introduction
Clostridium botulinum produces botulinum neurotoxin (BoNT), which prevents the release of acetylcholine at the motor end plate [1][2][1,2]. In aesthetic settings, BoNT is frequently used to target the platysma muscle to diminish the platysmal band or jawline lifting (Figure 1A). Platysma bands are two strips of muscle bands that are found in the hypercontraction status of the platysma muscle (Figure 1B). The bands get more prominent with age and become an aesthetic concern [3].
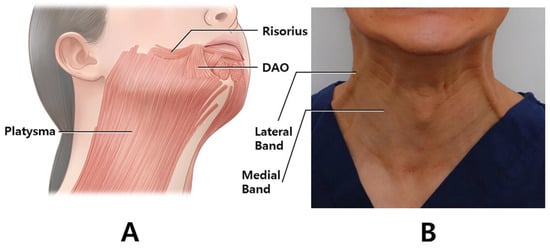
Figure 1. The image of the playsmal bands. The posterior and anterior platysmal bands are targeted for botulinum neurotoxin (A). Schematic image of the platysma muscle in oblique view. The muscle intermingles with the depressor anguli oris, depressor labii inferioris, mentalis, risorius, and orbicularis oris muscles (B). (DAO; depressor anguli oris).
awline lifting is also an aesthetic treatment conducted with BoNT injection in the jawline, which is given in the platysma muscle [4].
The platysma muscle acts by pulling down the modiolus, corners of the mouth, and lower third of the face. Therefore, BoNT injection into the platysma muscle results in lifting of the lower third of the face and jawline contour, which improves the esthetic appearance by correcting the drooping corners of the mouth and jowls.
However, an overdose of BoNT may paralyze nearby muscles, causing dysphonia, dysphagia, and an asymmetrical appearance [5]. Inadvertent diffusion of BoNT into the depressor labii inferioris or risorius muscle may result in an asymmetric smile (Figure 1B). To prevent these undesirable results, anatomy-based precise injection in the platysma muscle and beginning the primary treatment on a lower quantity of BoNT are recommended. Recent studies on BoNT injection in specific locations for anatomical assessments of particular muscles have been conducted on the basis of external anatomical features [6][7][6,7].
Clinicians treating the platysma muscle need to have a good understanding of the anatomy of the jaw and neck. However, few anatomical findings have been reviewed with clinical application (location, injection technique, and dosage).
2. Anatomy of the Platysma Muscle
The platysma is a superficially located thin and broad muscle underneath the subcutaneous fatty layer, which covers most of the neck region (Figure 2A) [8]. The superior part of the platysma muscle, involved in expression, pulls the cheilion inferiorly and widens the lips. The inferior part of the platysma muscle acts by pulling the skin of the neck superiorly. Neural innervation is facilitated by the cervical branch of the facial nerve, and blood supply is facilitated by branches of the submental and suprascapular arteries. The platysma muscle originates from the fascial structure of the pectoralis major and ends at the anterior deltoid (Figure 3A). The muscle fibers superiorly blend medially into the depressor anguli oris, depressor labii inferioris, and lower lip, and laterally form the superficial musculoaponeurotic system (Figure 3B).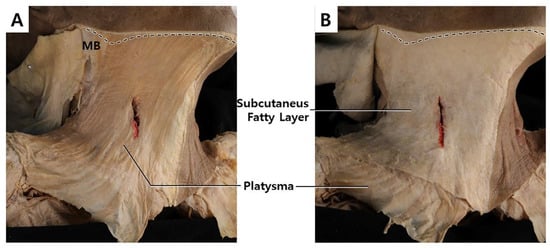
Figure 2. The dissected image of the platysma muscle in a cadaver (A) and revealing platysma muscle by removing subcutaneous tissue (B).
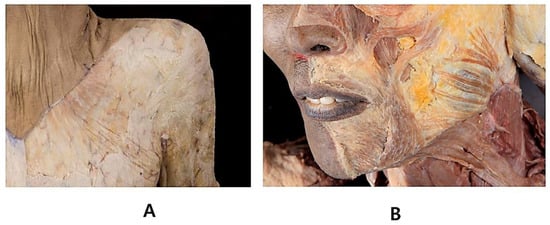
Figure 3. Platysma muscle continuously extends to the fascial structure of pectoralis major and anterior deltoid (A). The platysma also extends to mid-face region (B).
3. Platysmal Band Injection Points and Methods
Two units (U) are injected per point, and five points are injected for each band, approximately 2 cm from each other along the muscular band. A total of 40 units are used on both sides of the medial and lateral bands. The type of the botulinum toxin proposed are type A, ona-botulinum toxins. The ona-botulinum toxin A was set as the gold standard since it was first approved and commercialized as BoNT. There are conversion rate to other dosing unit and dilution rate. [9] The author dilutes with 2.5 mL of normal saline to use at a concentration of 4 U/0.1 mL. Platysmal bands should be assessed primarily. First, patients are asked to make a gloomy face by pulling down hard on the mouth angle, such that the platysma muscle is hyperactivated. Then, the BoNT is directly injected into the muscular bands 5 points below the jawline to the clavicle. Following that, 2 U each is injected at 5 points along the medial and lateral bands (Figure 4).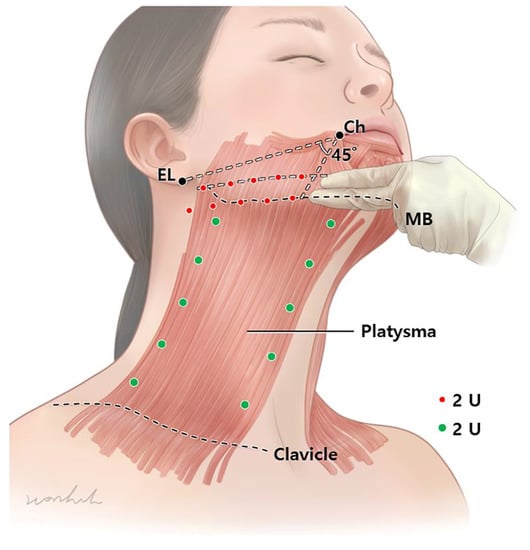
Figure 4. The jawline lifting, 2 U is injected per point. A total of 20 U of botulinum neurotoxin per side is injected. The injection should be in two lines (distance of two finger width), one right above the mandibular lower border and one below the line connecting the cheilion and ear lobule. For the platysmal bands, 2 U is injected per point (green dots). For injection, 5 points are placed for each band approximately 2 cm from each other along the muscular band. A total of 40 units are used for both sides of medial and lateral bands. (EL, ear lobe; Ch, Cheilion; MB, Mandibular border.).