Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Jing-Xing Li and Version 2 by Dean Liu.
Inflammatory bowel disease (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic, inflammatory, polygenic, multifactorial, and multifactorial illness with unknown etiology. Studies have reported extraintestinal manifestations (EIMs) or issues in several organ systems, including musculoskeletal, dermatologic, ocular, pulmonary, renal, and hepatobiliary systems.
- ocular extra-intestinal manifestation
- uveitis
- episcleritis
- conjunctivitis
- inflammatory bowel disease
- Crohn's disease
- ulcerative colitis
- IBD
1. Introduction
Inflammatory bowel disease (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC), is a chronic, inflammatory, polygenic, multifactorial, and multifactorial illness with unknown etiology. Studies have reported extraintestinal manifestations (EIMs) or issues in several organ systems, including musculoskeletal, dermatologic, ocular, pulmonary, renal, and hepatobiliary systems [1]. Furthermore, the existing literature is inconsistent in terms of whether these EIMs are more associated with CD or UC. Ocular EIMs (O-EIMs) are reported in 4–12% of patients with IBD, and the rate was recorded up to 29% in some cohorts [2]. EIMs are more prevalent in CD than in UC. Ocular symptoms were observed from mild conjunctivitis and episcleritis to severe inflammation, such as scleritis and uveitis. Uveitis is typically more serious and causes vision loss, whereas episcleritis is a benign condition. The most prevalent ocular IBD symptoms are episcleritis (2–5%) and uveitis (0.5–3.5%) [3][4][3,4]. Uveitis is a uveal tract inflammation involving the iris, ciliary body, and choroid and may lead to visual impairments [5][6][5,6]. According to the predominant site of inflammation, uveitis can be classified as anterior, middle, posterior, or panuveitis. Patients with IBD exhibit bilateral anterior uveitis with a gradual onset [7][8][7,8] and are unrelated to IBD activity.
Nonetheless, the prevalence reported by research varies considerably, which makes it difficult to determine if O-EIMs are more prevalent in patients with CD or UC. Although a higher prevalence of O-EIMs has been demonstrated in CD patients compared with UC patients [9], the results are controversial [10][11][10,11]. CD and UC represent two separate disease entities. CD can affect any part of the GI tract, but the large and small intestines are most affected, while UC mainly affects the colon and rectum. CD is more severe than UC, yet UC is significantly more prevalent worldwide. Moreover, the risk factors of CD and UC were substantially distinct [12].
2. Association of O-EIMs with IBD
Figure 12 shows the forest plot of the prevalence of O-EIMs in patients with CD or UC. Some studies provided information on indeterminate IBD, which was excluded from the meta-analysis because it could not be categorized into CD or UC. The meta-analysis demonstrated an association between uveitis and CD, and adults with CD have a significantly elevated risk of uveitis (pooled OR 1.603, 95% CI 1.254–2.049, p < 0.001) (Figure 12A). Cochran’s chi-square test (p < 0.001) and I2 statistic (I2 = 76.116%) revealed significant heterogeneity among studies. Nonetheless, the prevalence of episcleritis and conjunctivitis had no significant difference between CD and UC (Figure 12B,C).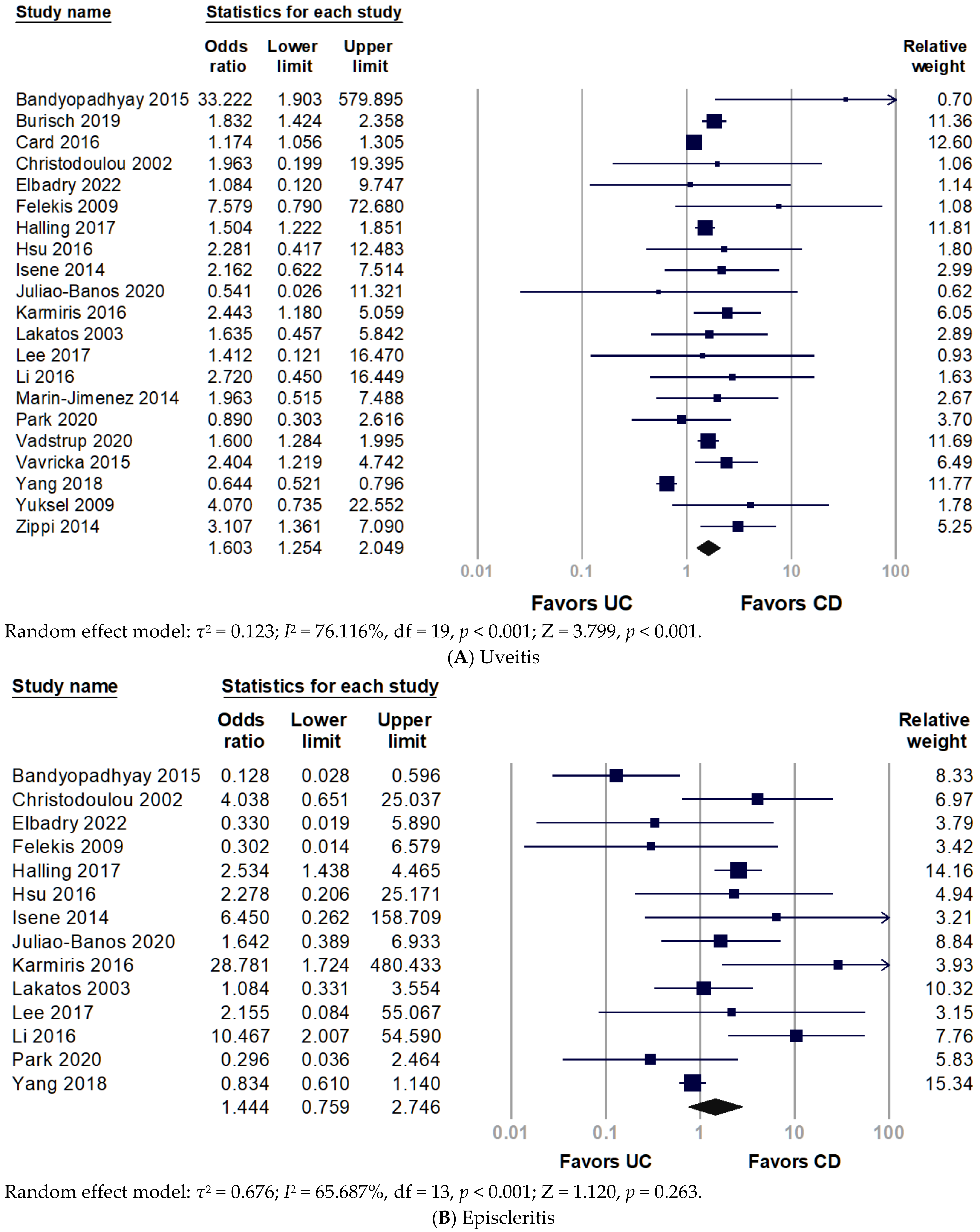
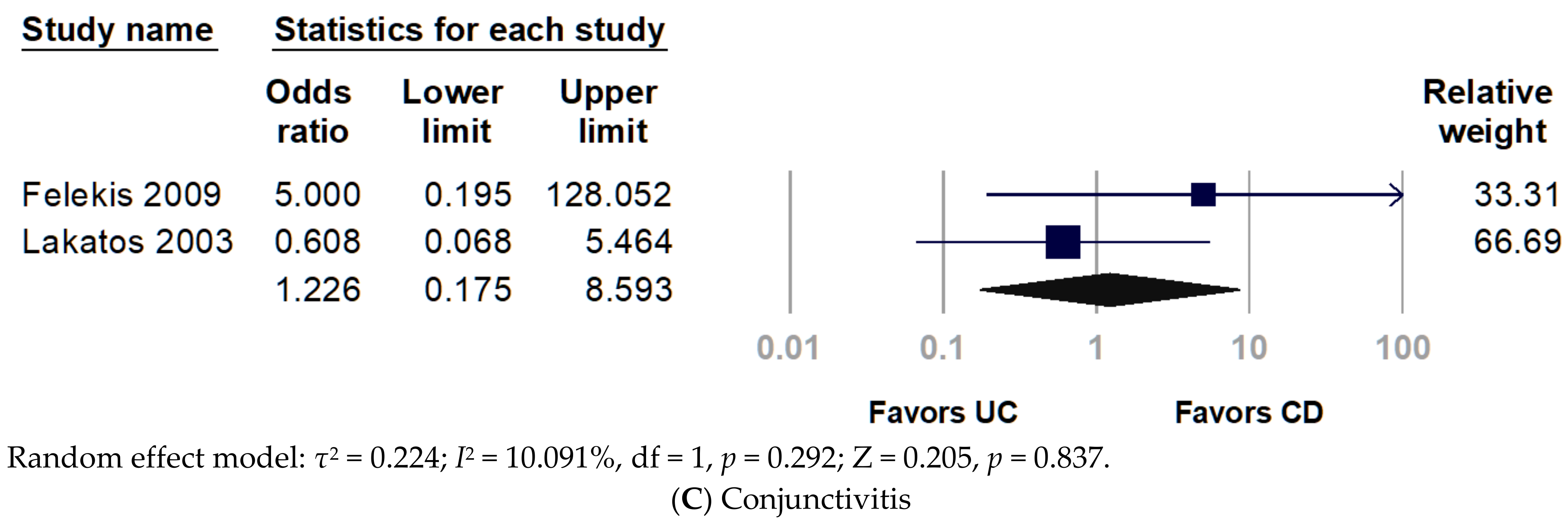
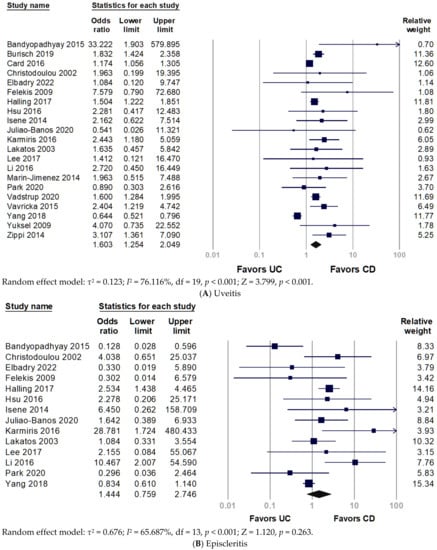
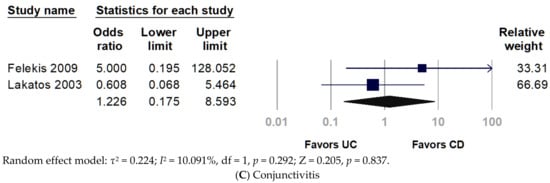
Figure 12. Forest plot for prevalence of ocular extra-intestinal manifestation among adult patients with inflammatory bowel disease: (A) uveitis; (B) episcleritis; (C) conjunctivitis. CD, Crohn’s disease; UC, ulcerative colitis.
3. Stratification with World Regions
To investigate the disparity between world region and race, rwesearchers divided included studies into Asia, Central Asia, and Europe. Figure 23 presents the subgroup analyses by region of the study population. The pooled analysis of the Asian population revealed non-significantly increased odds of uveitis in patients with CD (pooled OR 1.428, 95% CI 0.612–3.334, p = 0.410). Only two studies in Central Asia were involved in the analysis, without significant results, but they presented a trend that uveitis favored in patients with CD over UC (pooled OR 2.468, 95% CI 0.640–9.525, p = 0.190). Conversely, European studies indicated a significantly increased prevalence of uveitis in patients with CD (pooled OR 1.683, 95% CI 1.377–2.056, p < 0.001). For episcleritis, the frequency of episcleritis did not differ between CD and UC (Figure 12B). Nonetheless, European populations had a significantly higher prevalence of episcleritis in patients with CD than UC (pooled OR 2.401, 95% CI 1.112–5.184, p = 0.026) (Figure 23B).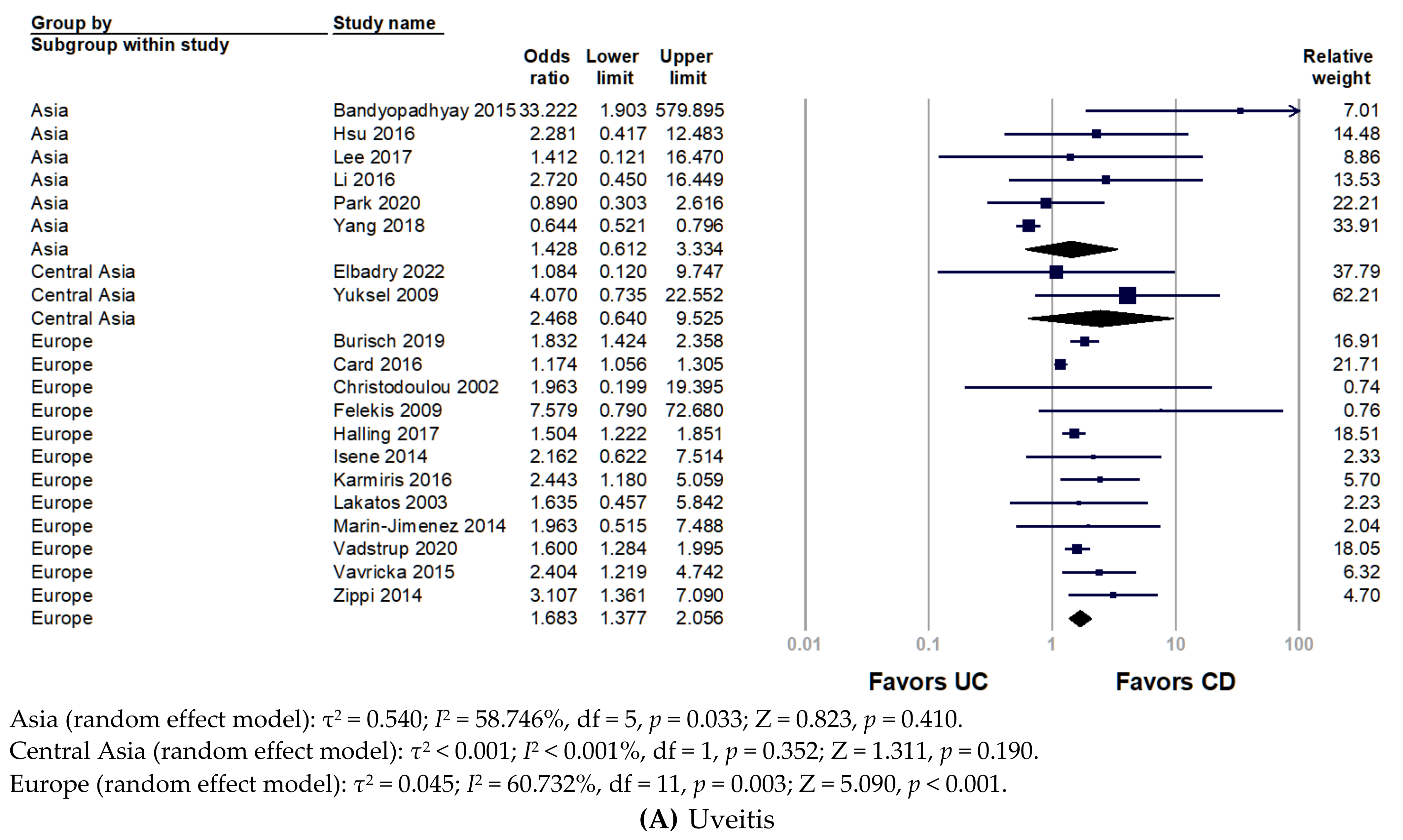
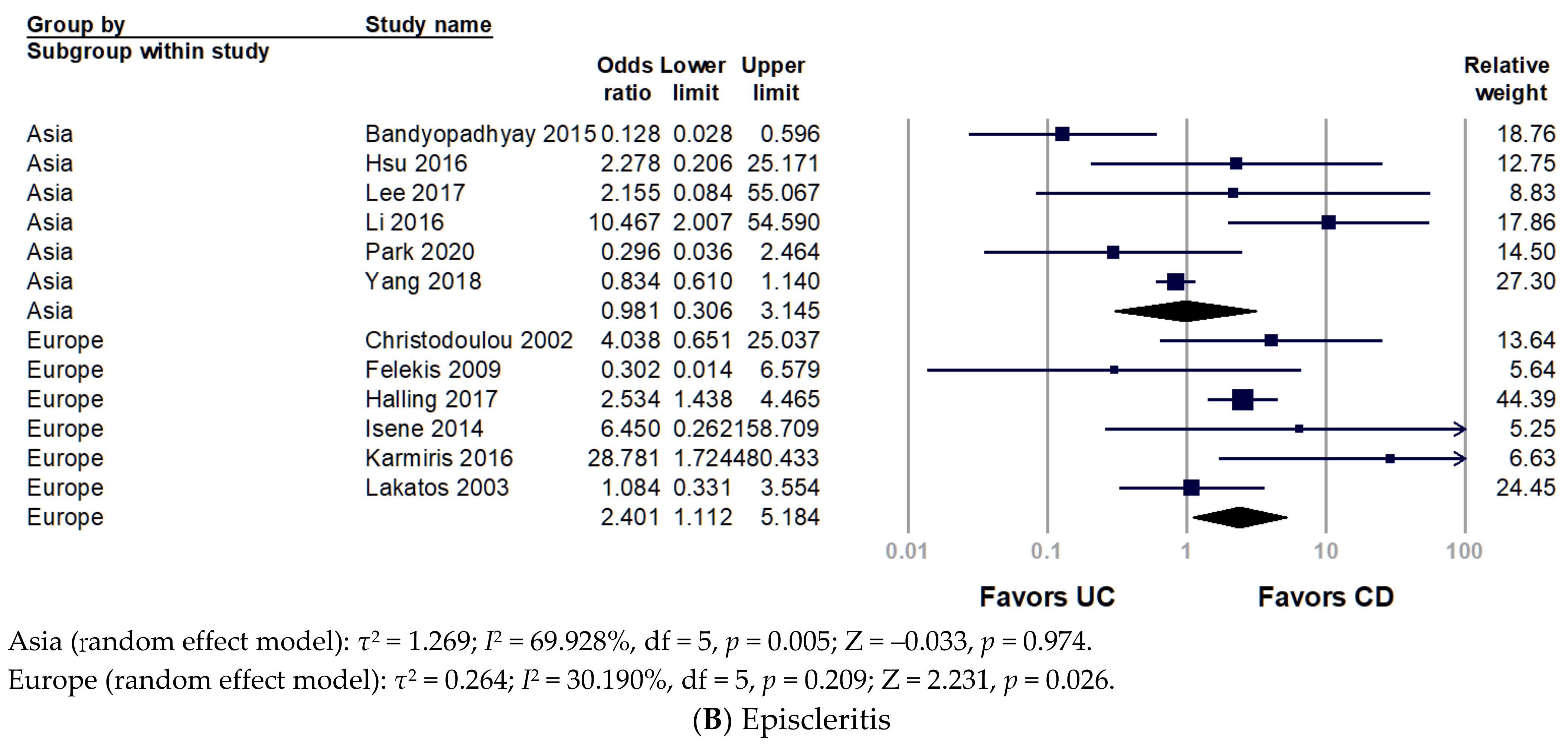
Figure 23. Forest plot for the prevalence of ocular extra-intestinal manifestation among adult patients with inflammatory bowel disease stratified by world region: (A) uveitis; (B) episcleritis. CD, Crohn’s disease; UC, ulcerative colitis.
4. Chronological Analysis
Only two studies showed uveitis before and after IBD diagnosis. The pooled analysis indicated no significant finding (pooled OR 2.152, 95% CI 0.136–33.964, p = 0.586) since extreme heterogeneity (I2 = 99.516%) (Figure 4).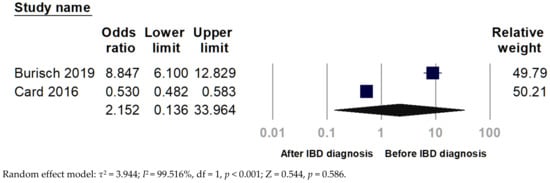
Figure 34.
Forest plot for the chronological relationship between uveitis and inflammatory bowel disease (IBD).
5. Period Prevalence of O-EIMs
Figure 45 illustrates the overall prevalence of uveitis, episcleritis, and conjunctivitis. The period prevalence of uveitis in CD and UC ranged from 0–21.57% and 0–4.76%, respectively. While the period prevalence of episcleritis in CD and UC was 0–5.41% and 0–24.14%, respectively.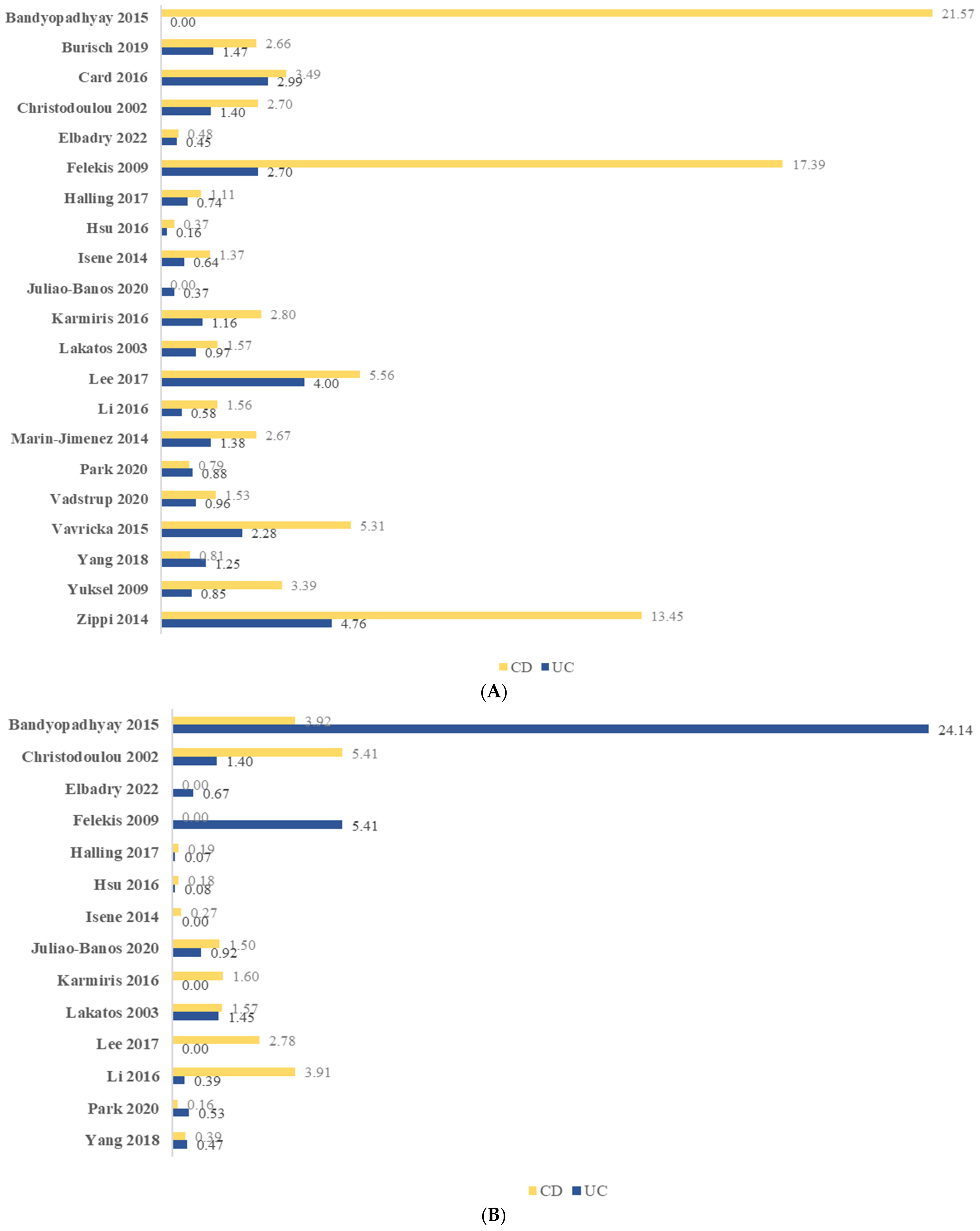


Figure 45. Period prevalence (%) of ocular manifestation among adult patients with inflammatory bowel disease: (A) uveitis; (B) episcleritis; (C) conjunctivitis. CD, Crohn’s disease; UC, ulcerative colitis.