Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Esperanza Duarte-Escalante and Version 2 by Catherine Yang.
COVID-19-associated pulmonary aspergillosis (CAPA) has had a high incidence. In addition, it has been associated with prolonged hospital stays, as well as several predisposing risk factors, such as fungal factors (nosocomial organism, the size of the conidia, and the ability of the Aspergillus spp. of colonizing the respiratory tract), environmental factors (remodeling in hospitals, use of air conditioning and negative pressure in intensive care units), comorbidities, and immunosuppressive therapies. In addition to these factors, SARS-CoV-2 per se is associated with significant dysfunction of the patient’s immune system, involving both innate and acquired immunity, with reduced CD4+ and CD8+ T cell counts and cytokine storm.
- Aspergillus
- SARS-CoV-2
- CAPA
- interaction
- coinfection
1. Comorbidities
In general, critically ill patients admitted to the ICU with comorbidities seem more susceptible to CAPA. This is very rare in non-severe cases, so the severity of COVID-19 is considered a risk factor. Among the most frequent comorbidities associated with CAPA are advanced age, diabetes, pulmonary diseases, cardiovascular diseases, hypertension, and solid organ malignancy [1][2][3][5,6,7]. However, other comorbidities associated with CAPA are also mentioned, including obesity, chronic respiratory diseases, and asthma [4][5].
Likewise, Gregoire et al. [5][8] cite other factors associated with CAPA, such as structural lung defects, severe lung damage during the course of COVID-19, and the use of broad-spectrum antibiotics. In addition, the authors found that patients with a history of cerebrovascular disease and hypertension also had a marked trend associated with CAPA [6][9]. Sagris et al. [7][10] have suggested a likely explanation for the increased severity of ischemic stroke observed in COVID-19 patients; the authors mention that a possible direct effect of SARS-CoV-2 on the brain may have a causal relationship with local brain ischemia and inflammation, in addition to brain tissue death, which causes, as a result, an excessive release of DAMP (damage associated molecular patterns), which in turn causes localized and global inflammation, and promotes the disruption of the blood–brain barrier. Thus, during the hyperinflammatory state of COVID-19, the overproduction of proinflammatory acute response proteins and adhesion molecules, together with activated circulating leukocytes, may result in the increase of the local inflammatory process in the ischemic brain. Although there are still not enough published statistical data, coinfections in SARS-CoV-2 patients have revealed that a significant number of hospitalized patients have developed secondary systemic mycoses, including aspergillosis, which cause serious complications, and even death. In severe cases, the risk of developing invasive fungal infections is high; this is not only due to the clinical situation of the patient and the need for invasive care, but also due to the immunological alterations caused by SARS-CoV-2 [8][11].
They also report that patients under treatment with immunosuppressants, as well as treatment with azithromycin (AZT) and hydroxychloroquine (HCQ), and DXM, showed a significant association with CAPA. They highlight that AZT has an immunomodulatory effect as it can inhibit neutrophils and the innate immune response, lowering the immune defense against Aspergillus. Further, its broad-spectrum antibiotic effect could alter the patients’ microbiota, thus promoting colonization by Aspergillus. In these patients, clusters of microbiomes have been observed to grow in the gut due to lymphopenia caused by infection [9][12].
Likewise, the use of corticosteroids to treat severe COVID-19 constitutes another risk factor associated with CAPA [10][6]. One study shows that long-term steroid treatment in doses greater than or equal to 16 mg/day of prednisone for at least 15 days was significantly more frequent in patients with CAPA than those without CAPA [3,13]. However, some studies have found no association between the use of these and the incidence of hospital-acquired fungal infections in patients with COVID-19. Feys et al. [10][6] and Salazar et al. [11][14] mention that the discrepancies can be attributed to the different cumulative doses of corticosteroids or the lack of statistical power to analyze the data.
The advanced age of COVID-19 patients shows significant implications for their immune systems. The most evident effect in elderly patients with cardiovascular diseases is that, due to the aging of their immune system, the imbalance within their innate and adaptive immune response generally worsens, causing a decrease in lymphocytes and an uncontrollable inflammatory reaction due to a cytokine storm. The result is an inadequate immune response, a lack of effective immune memory, and an inability to clear the virus. In addition, it causes injury to the lung epithelium and microvascular endothelium throughout the body, thus leading to ARDS and microvascular thrombosis, which could eventually favor the entry and development of Aspergillus, leading to high mortality among the elderly COVID-19 patients with cardiovascular diseases [12][13][14][15,16,17].
Additionally, various studies have shown a greater severity of COVID-19 in patients with diabetes mellitus. It is mentioned that patients infected with COVID-19 could predispose individuals to hyperglycemia, and by interacting with other risk factors, hyperglycemia could modulate the immune and inflammatory responses, predisposing patients to severe COVID-19 [15][16][17][18,19,20].
Furthermore, a study published by Sudhakar et al. [18][21] highlights obesity as a significant comorbidity in COVID-19 patients since it is a metabolic disorder with a deregulated immune and endocrine function, inferring that dysfunctional metabolism contributes to the fact that the mechanisms behind obesity are a risk factor with adverse outcomes in COVID-19 patients. The authors suggest that, in obese individuals, visceral adiposity expansion (VAT) leads to metabolic dysfunction, endoplasmic reticulum stress, immune cell infiltration, macrophage polarization to a pro-inflammatory phenotype, adipocyte cell death, and inflammation. It is also associated with the altered expression of adipokines and cytokines that cause systemic effects and dysfunction of endocrine and metabolic organs. They note that such a state of adipose tissue, particularly associated with multiple organs such as the lungs, vasculature, heart, and kidneys, may predispose obese subjects to adverse outcomes of COVID-19 infection.
In a large meta-analysis study by Wang et al. [19][22], evidence showed that COVID-19 patients with chronic obstructive pulmonary disease (COPD) have a risk of progression 5.9 times higher than patients without COPD. They also identified a higher risk of worsening in people with hypertension, diabetes, cardiovascular disease, or cerebrovascular disease, suggesting an opportunity for coinfections, including Aspergillus.
2. Changes in the Immune Response That Predispose to CAPA
Currently, there is no consensus to clearly define the risk factors associated with CAPA, and the results published to date should be taken with caution, since many studies are still under investigation. In addition, the variability in the diagnostic criteria used for the diagnosis of CAPA could lead to overdiagnosis, overtreatment, and overestimation of the true risk factors and associated outcomes, so significant predictors and prognostic factors may have been ruled out due to a lack of analyzed data [20][23].
It is known that influenza-associated pulmonary aspergillosis (IAPA) and CAPA share certain characteristics; however, IAPA has a higher incidence, most cases are observed in the first 48 h in the ICU, and it is more aggressive than CAPA. Moreover, the mechanism by which the intrinsic immune dysregulation caused by the influenza virus and SARS-CoV-2 occurs is unknown [10][6]. Recently, some hypotheses of the pathophysiology have been proposed that can explain the development of CAPA. The first hypothesis is related to the dysfunctional response of IFN (interferon) type I and III in severe COVID-19 patients (Figure 1), which has a fundamental role against Aspergillus spp., by promoting the response of type 1 T-helper cells against the fungus and driving type III IFN production, causing neutrophils to act against A. fumigatus [10][6]. The second hypothesis is related to IFN deregulation, together with cell exhaustion, particularly of alveolar macrophages, since they are the first cells to recognize inhaled conidia, being another poss ible cause of invasion by Aspergillus spp.
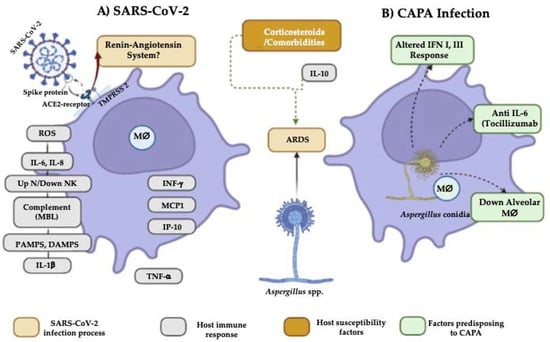
Figure 1. COVID-19-associated pulmonary aspergillosis (CAPA) infectious process. (A) Dysregulation of the renin-angiotensin system creates a pro-inflammatory environment in the host through reactive oxygen species (ROS), IL-6 and IL-8, pulmonary cell infiltrate by neutrophils, complement activation, and recognition of viral RNA through pathogen-associated molecular patterns (PAMPS), while damage-associated molecular patterns (DAMPS) stimulate large amounts of IL-1β and TNF-α. In addition, IFNγ, MCP1, and IP-10 are produced. This process causes acute respiratory distress syndrome (ARDS), which, together with corticosteroids, patient comorbidities, and Aspergillus in the environment, facilitates the fungal invasion of the host. (B) In addition, a deficient immune response from the host alters the IFN I and III production; likewise, medications and decreased alveolar macrophages favor susceptibility to CAPA.
In IAPA, it is known that the effectiveness of phagocytosis against Aspergillus spp., associated with LC3 (Light Chain 3B) (which is a pathway for phagosome–lysosome fusion), is altered by the use of corticosteroids such as dexamethasone, hindering the activity of alveolar macrophages and consequently the production of anti-inflammatory cytokines such as IL-10 [21][24]; this alteration can also predispose the host to acquire CAPA [10][6]. Moreover, it is known that in severe cases of COVID-19, as well as in aspergillosis caused by A. fumigatus [22][25], in addition to CAPA, there are elevated levels of IL-6, which contributes to an increase in lung damage. Particularly in CAPA, tocilizumab (IL-6 receptor antagonist) has been used to reduce its expression; however, its administration has not shown efficacy in resolving the disease since it does not regulate the basal production of this cytokine and prevents the Th17 protective response and effector functions of phagocytes [11][23][24][25][1,2,4,14].
Other risk factors that predispose to CAPA are deregulation of the renin-angiotensin system and/or the kallikrein-kinin system produced by the binding of SARS-CoV-2 to the ACE2 receptor; however, its mechanism is unknown [23][1]. As part of the innate immune response, pathogen-associated molecular patterns (PAMPS), damage-associated molecular patterns (DAMPS), and pattern recognition receptors (PRR) are present in macrophages, dendritic cells, and neutrophils, and constitute the first line of defense against the virus. In this sense, a risk factor is due to cellular deterioration caused in NK cells, whose function is the direct elimination of fungal pathogens and stimulation of other cells such as neutrophils [26], which has been related to increased susceptibility to co-infections [11][14]. Platelets represent another predisposing factor since they are considered key regulators of the innate immune response, and it has been shown that an increase in the platelet count is associated with the severity of the disease in patients with COVID-19. This is due to the fact that platelets express ACE2; furthermore, in vitro exposure to SARS-CoV-2 has been observed to potentiate platelet activation and aggregation, resulting in vascular complications seen in patients with COVID-19 and increased susceptibility to co-infections [11][14].
Moreover, the production of IL-1β in high concentrations leads to a pro-inflammatory environment, making fungal pathogenesis permissible. This is due to the production of DAMPS, which are proposed as a possible immunomodulatory strategy in CAPA because they promote and exacerbate the immune and inflammatory response leading to lung injury, particularly due to an increase in the inflammatory reaction in experimental aspergillosis [23][1], predisposing COVID-19 patients to secondary Aspergillus infection.
Another host susceptibility factor is lymphopenia, which, together with the pro-inflammatory environment and the cytosine storm, can have an impact on the functionality and efficacy of the immune response [27], which leads to, as a result, the development of CAPA in individuals who present some type of comorbidity. Although efforts have allowed us to learn a little more about this coinfection, the pathophysiological processes that originate it have yet to be discovered.
3. Influence of Antifungals on the Aspergillus-SARS-CoV-2 Interaction
In invasive aspergillosis (AI), it is known that early intervention with an appropriate antifungal agent can contribute to patient improvement, so the use of voriconazole is recommended as the first line of defense [23][1]. Voriconazole has been widely used in CAPA; however, the interaction between voriconazole and drugs used in the treatment of COVID-19 (hydroxychloroquine, azithromycin, and protease inhibitors, such as lopinavir/ritonavir) has been reported to cause cardiac events [28][29][28,29]. As a result, the treatment is not effective for patients [30], demonstrating its low effectiveness, which has also been reported for itraconazole [23][1].
Furthermore, Aspergillus fumigatus and A. flavus are the opportunistic pathogens most commonly reported as etiological agents of CAPA [24][2]. Likewise, it is known that A. flavus has less sensitivity to voriconazole, amphotericin B, and 5-fluorocytosine [31], so the use of a single antifungal is not the best approach to show good results; particularly in the case of CAPA, the combination with other antifungals is promising [32]. Moreover, antifungals such as isavuconazole show a more favorable pharmacokinetic profile, and the toxicity is lower compared to voriconazole [23][1]. However, more studies are required to evaluate the usefulness of isavuconazole in CAPA.
Echinocandins have also been used for the treatment of CAPA, particularly caspofungin, which produced better results in these patients [33]. In addition, it is proposed that its use can prevent fungal infections and reduce severe cases of COVID-19, mainly in patients with hematological malignancies and who are in the ICU [34].
Due to the resistance to antifungals of some species of Aspergillus spp., clinical trials of new antifungals are currently being studied as therapeutic tools, which can be very useful in treating CAPA [35]. These antifungals include opelconazole, fosmanogepix, ibrexafungerp, olorofim, and rezafungin [11][14]. However, most are in phase III, so they are not yet available on the market. In addition, the efficacy of prophylactic treatment in the first days of stay of COVID-19 patients in the ICU has been evaluated, highlighting the efficiency of prophylaxis with posaconazole, which allows the reduction of CAPA cases by >90% [36]. No significant impact on survival was demonstrated; however, it could be considered an option since the drug–drug interaction, as occurs with voriconazole, is less due to the fact that it is metabolized by a different pathway.
References
- Pasquier, G.; Bounhiol, A.; Robert Gangneux, F.; Zahar, J.; Gangneux, J.P.; Novara, A.; Bougnoux, M.; Dannaoui, E. A review of significance of Aspergillus detection in airways of ICU COVID-19 patients. Mycoses 2021, 64, 980–988.Arastehfar, A.; Carvalho, A.; van de Veerdonk, F.L.; Jenks, J.D.; Koehler, P.; Krause, R.; Cornely, O.A.; SPerlin, D.; Lass-Flör, C.; Hoenig, M. COVID-19 associated pulmonary aspergillosis (CAPA)-From Immunology to Treatment. J. Fungi Basel Switz. 2020, 6, 91. [CrossRef] [PubMed]
- Feys, S.; Almyroudi, M.P.; Braspenning, R.; Lagrou, K.; Spriet, I.; Dimopoulos, G.; Wauters, J.A. Visual and comprehensive review on COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Fungi 2021, 7, 1067.Lai, C.C.; Yu, W.L. Covid-19 associated with pulmonary aspergillosis: A literature review. J. Microbiol. Immunol. Infect. 2021, 54, 46–53. [CrossRef]
- Janssen, N.A.F.; Nyga, R.; Vanderbeke, L.; Jacobs, C.; Ergün, M.; Buil, J.B.; van Dijk, K.; Altenburg, J.; Bouman, C.S.C.; van der Spoel, H.I.; et al. Multinational observational cohort study of COVID-19-associated pulmonary aspergillosis. Emerg. Infect. Dis. 2021, 27, 2892–2898.Bartoletti, M.; Pascale, R.; Cricca, M.; Rinaldi, M.; Maccaro, A.; Bussini, L.; Fornaro, G.; Tonetti, T.; Pizzilli, G.; Francalanci, E.; et al. Epidemiology of invasive pulmonary Aspergillosis among intubated patients with COVID-19: A prospective study. Clin. Infect. Dis. 2021, 73, e3606–e3614. [CrossRef]
- Pasquier, G.; Bounhiol, A.; Robert Gangneux, F.; Zahar, J.; Gangneux, J.P.; Novara, A.; Bougnoux, M.; Dannaoui, E. A review of significance of Aspergillus detection in airways of ICU COVID-19 patients. Mycoses 2021, 64, 980–988. Machado, M.; Valerio, M.; Álvarez-Uría, A.; Olmedo, M.; Veintimilla, C.; Padilla, B.; De la Villa, S.; Guinea, J.; Escribano, P.; Ruiz-Serrano, M.J.; et al. Invasive pulmonary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2020, 64, 132–143. [CrossRef] [PubMed]
- Gregoire, E.; Pirotte, B.F.; Moerman, F.; Altdorfer, A.; Gaspard, L.; Firre, E.; Moonen, M.; Fraipont, V.; Ernst, M.; Darcis, G. Incidence and risk factors of COVID-19-associated pulmonary aspergillosis in intensive care unit-A monocentric retrospective observational study. Pathogens 2021, 10, 1370. Pasquier, G.; Bounhiol, A.; Robert Gangneux, F.; Zahar, J.; Gangneux, J.P.; Novara, A.; Bougnoux, M.; Dannaoui, E. A review of significance of Aspergillus detection in airways of ICU COVID-19 patients. Mycoses 2021, 64, 980–988. [CrossRef]
- Xu, J.; Yang, X.; Lv, Z.; Zhou, T.; Liu, H.; Zou, X.; Cao, F.; Zhang, L.; Liu, B.; Chen, W.; et al. Risk factors for invasive aspergillosis in patients admitted to the intensive care unit with coronavirus disease 2019: A multicenter retrospective study. Front. Med. 2021, 8, 753659. Feys, S.; Almyroudi, M.P.; Braspenning, R.; Lagrou, K.; Spriet, I.; Dimopoulos, G.; Wauters, J.A. Visual and comprehensive review on COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Fungi 2021, 7, 1067. [CrossRef]
- Sagris, D.; Papanikolaou, A.; Kvernland, A.; Korompok Frontera, E.J.A.; Troxe, A.B.; Gavriatopoulou, M.; Milionis, H.; Lip, G.Y.H.; Michel, P.; Yaghi, S.; et al. COVID-19 and ischemic stroke. Eur. J. Neurol. 2021, 28, 3826–3836. Janssen, N.A.F.; Nyga, R.; Vanderbeke, L.; Jacobs, C.; Ergün, M.; Buil, J.B.; van Dijk, K.; Altenburg, J.; Bouman, C.S.C.; van der Spoel, H.I.; et al. Multinational observational cohort study of COVID-19-associated pulmonary aspergillosis. Emerg. Infect. Dis. 2021, 27, 2892–2898. [CrossRef] [PubMed]
- Videla, C.G.; Agustina, M.; de la Iglesia Niveyro, P.X.; Ciarrocchi Nicolas, M. Muerte cerebral debida a aspergilosis cerebral en un paciente de COVID-19. Rev. Esp. Anestesiol. Y Reanim. 2022; 69, 592–596. Gregoire, E.; Pirotte, B.F.; Moerman, F.; Altdorfer, A.; Gaspard, L.; Firre, E.; Moonen, M.; Fraipont, V.; Ernst, M.; Darcis, G. Incidence and risk factors of COVID-19-associated pulmonary aspergillosis in intensive care unit-A monocentric retrospective observational study. Pathogens 2021, 10, 1370. [CrossRef] [PubMed]
- Bhotla, H.K.; Balasubramanian, B.; Meyyazhagan, A.; Pushparaj, K.; Easwaran, M.; Pappusamy, M.; Robert, A.A.; Arumugam, V.A.; Tsibizova, V.; Alfalih, A.M.; et al. Opportunistic mycoses in COVID-19 patients/survivors: Epidemic inside a pandemic. J. Infect. Public Health 2021, 14, 1720–1726. Xu, J.; Yang, X.; Lv, Z.; Zhou, T.; Liu, H.; Zou, X.; Cao, F.; Zhang, L.; Liu, B.; Chen, W.; et al. Risk factors for invasive aspergillosis in patients admitted to the intensive care unit with coronavirus disease 2019: A multicenter retrospective study. Front. Med. 2021, 8, 753659. [CrossRef
- Feys, S.; Almyroudi, M.P.; Braspenning, R.; Lagrou, K.; Spriet, I.; Dimopoulos, G.; Wauters, J.A. Visual and comprehensive review on COVID-19-Associated Pulmonary Aspergillosis (CAPA). J. Fungi 2021, 7, 1067. Sagris, D.; Papanikolaou, A.; Kvernland, A.; Korompok Frontera, E.J.A.; Troxe, A.B.; Gavriatopoulou, M.; Milionis, H.; Lip, G.Y.H.; Michel, P.; Yaghi, S.; et al. COVID-19 and ischemic stroke. Eur. J. Neurol. 2021, 28, 3826–3836. [CrossRef] [PubMed]
- Salazar, F.; Bignell, E.; Brown, G.D.; Cook, P.C.; Warris, A. Pathogenesis of respiratory viral and fungal coinfections. Clin. Microbiol. Rev. 2022, 35, e00094-21. Videla, C.G.; Agustina, M.; de la Iglesia Niveyro, P.X.; Ciarrocchi Nicolas, M. Muerte cerebral debida a aspergilosis cerebral en un paciente de COVID-19. Rev. Esp. Anestesiol. Y Reanim. 2022, 6, 592–596. [CrossRef]
- Aiello, A.; Farzaneh, F.; Candore, G.; Caruso, C.; Davinelli, S.; Gambino, C.M.; Ligotti, M.E.; Zareian, N.; Accardi, G. Immunosenescence and its hallmarks: How to oppose aging strategically? A review of potential options for therapeutic intervention. Front. Immunol. 2019, 10, 2247. Bhotla, H.K.; Balasubramanian, B.; Meyyazhagan, A.; Pushparaj, K.; Easwaran, M.; Pappusamy, M.; Robert, A.A.; Arumugam, V.A.; Tsibizova, V.; Alfalih, A.M.; et al. Opportunistic mycoses in COVID-19 patients/survivors: Epidemic inside a pandemic. J. Infect. Public Health 2021, 14, 1720–1726. [CrossRef]
- Kadambari, S.; Klenerman, P.; Pollard, A.J. Why the elderly appear to be more severely affected by COVID-19: The potential role of immunosenescence and CMV. Rev. Med. Virol. 2020, 30, e2144. Verweij, P.E.; Brüggemann, R.J.M.; Azoulay, E.; Bassetti, M.; Blot, S.; Buil, J.B.; Calandra, T.; Chiller, T.; Clancy, C.J.; Cornely, O.A.; et al. Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis. Intensiv. Care Med. 2021, 47, 819–834. [CrossRef] [PubMed]
- Wang, Y.; Pang, S.C.; Yang, Y. A potential association between immunosenescence and high COVID-19 related mortality among elderly patients with cardiovascular diseases. Immun. Ageing 2021, 18, 25. Salazar, F.; Bignell, E.; Brown, G.D.; Cook, P.C.; Warris, A. Pathogenesis of respiratory viral and fungal coinfections. Clin. Microbiol. Rev. 2022, 35, e00094-21. [CrossRef] [PubMed]
- Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. Aiello, A.; Farzaneh, F.; Candore, G.; Caruso, C.; Davinelli, S.; Gambino, C.M.; Ligotti, M.E.; Zareian, N.; Accardi, G. Immunose nescence and its hallmarks: How to oppose aging strategically? A review of potential options for therapeutic intervention. Front. Immunol. 2019, 10, 2247. [CrossRef]
- Lim, S.; Bae, J.H.; Kwon, H.S.; Nauck, M.A. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2021, 17, 11–30. Kadambari, S.; Klenerman, P.; Pollard, A.J. Why the elderly appear to be more severely affected by COVID-19: The potential role of immunosenescence and CMV. Rev. Med. Virol. 2020, 30, e2144. [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. Wang, Y.; Pang, S.C.; Yang, Y. A potential association between immunosenescence and high COVID-19 related mortality among elderly patients with cardiovascular diseases. Immun. Ageing 2021, 18, 25. [CrossRef]
- Sudhakar, M.; Winfred, S.B.; Meiyazhagan, G.; Venkatachalam, D.P. Mechanisms contributing to adverse outcomes of COVID-19 in obesity. Mol. Cell Biochem. 2022, 477, 1155–1193. Holman, N.; Knighton, P.; Kar, P.; O’Keefe, J.; Curley, M.; Weaver, A.; Barron, E.; Bakhai, C.; Khunti, K.; Wareham, N.J.; et al. Risk factors for COVID-19-related mortality in people with type 1 and type 2 diabetes in England: A population-based cohort study. Lancet Diabetes Endocrinol. 2020, 8, 823–833. [CrossRef]
- Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. Lim, S.; Bae, J.H.; Kwon, H.S.; Nauck, M.A. COVID-19 and diabetes mellitus: From pathophysiology to clinical management. Nat. Rev. Endocrinol. 2021, 17, 11–30. [CrossRef]
- Chong, W.H.; Saha, B.K.; Neu, K.P. Comparing the clinical characteristics and outcomes of COVID-19-associate pulmonary aspergillosis (CAPA): A systematic review and meta-analysis. Infection 2022, 50, 43–56. Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [CrossRef]
- Apostolopoulou, A.; Garrigos, Z.E.; Vijayvargiya, P.; Lerner, A.H.; Farmakiotis, D. Invasive pulmonary aspergillosis in patients with SARS-CoV-2 infection: A systematic review of the literature. Diagnostics 2020, 10, 807. Sudhakar, M.; Winfred, S.B.; Meiyazhagan, G.; Venkatachalam, D.P. Mechanisms contributing to adverse outcomes of COVID-19 in obesity. Mol. Cell Biochem. 2022, 477, 1155–1193. [CrossRef] [PubMed]
- Borger, P.; Koeter, G.H.; Timmerman, A.J.; Vellenga, A.; Tomee, J.F.; Kauffman, H.F. Protease from Aspergillus fumigatus induce interleukin (IL)-6 and IL-8 producin in airway epithelial cell lines by transcriptional mechanisms. J. Infect. Dis. 1999, 180, 1267–1274. Wang, B.; Li, R.; Lu, Z.; Huang, Y. Does comorbidity increase the risk of patients with COVID-19: Evidence from meta-analysis. Aging 2020, 12, 6049–6057. [CrossRef] [PubMed]
- Arastehfar, A.; Carvalho, A.; van de Veerdonk, F.L.; Jenks, J.D.; Koehler, P.; Krause, R.; Cornely, O.A.; SPerlin, D.; Lass-Flör, C.; Hoenig, M. COVID-19 associated pulmonary aspergillosis (CAPA)-From Immunology to Treatment. J. Fungi Basel Switz. 2020, 6, 91. Chong, W.H.; Saha, B.K.; Neu, K.P. Comparing the clinical characteristics and outcomes of COVID-19-associate pulmonary aspergillosis (CAPA): A systematic review and meta-analysis. Infection 2022, 50, 43–56. [CrossRef]
- Lai, C.C.; Yu, W.L. Covid-19 associated with pulmonary aspergillosis: A literature review. J. Microbiol. Immunol. Infect. 2021, 54, 46–53. Apostolopoulou, A.; Garrigos, Z.E.; Vijayvargiya, P.; Lerner, A.H.; Farmakiotis, D. Invasive pulmonary aspergillosis in patients with SARS-CoV-2 infection: A systematic review of the literature. Diagnostics 2020, 10, 807. [CrossRef]
- Machado, M.; Valerio, M.; Álvarez-Uría, A.; Olmedo, M.; Veintimilla, C.; Padilla, B.; De la Villa, S.; Guinea, J.; Escribano, P.; Ruiz-Serrano, M.J.; et al. Invasive pulmonary aspergillosis in the COVID-19 era: An expected new entity. Mycoses 2020, 64, 132–143. Borger, P.; Koeter, G.H.; Timmerman, A.J.; Vellenga, A.; Tomee, J.F.; Kauffman, H.F. Protease from Aspergillus fumigatus induce interleukin (IL)-6 and IL-8 producin in airway epithelial cell lines by transcriptional mechanisms. J. Infect. Dis. 1999, 180, 1267–1274. [CrossRef]
- Kuri-Cervantes, L.; Pampena, M.B.; Meng, W.; Rosenfeld, A.M.; Ittner, C.A.G.; Weisman, A.R.; Agyekum, R.S.; Mathew, D.; Baxter, A.E.; Vella, L.A.; et al. Comprehensive mapping of immune perturbations associated with severe COVID-19. Sci. Immunol. 2020, 5, eabd7114. Kuri-Cervantes, L.; Pampena, M.B.; Meng, W.; Rosenfeld, A.M.; Ittner, C.A.G.; Weisman, A.R.; Agyekum, R.S.; Mathew, D.; Baxter, A.E.; Vella, L.A.; et al. Comprehensive mapping of immune perturbations associated with severe COVID-19. Sci. Immunol. 2020, 5, eabd7114. [CrossRef] [PubMed]
- Lozada-Requena, I.; Núñez Ponce, C. COVID-19: Respuesta inmune y perspectivas terapéuticas. Rev. Peru Med. Exp. Salud Pública 2020, 37, 312–319. Lozada-Requena, I.; Núñez Ponce, C. COVID-19: Respuesta inmune y perspectivas terapéuticas. Rev. Peru Med. Exp. Salud Pública 2020, 37, 312–319. [CrossRef]
- Giudicessi, J.R.; Noseworthy, P.A.; Friedman, P.A.; Ackerman, M.J. Urgent guidance for navigating and circumventing the QTc-prolonging and torsadogenic potential of possible pharmaco-therapies for Coronavirus Disease 19 (COVID-19). Mayo Clin. Proc. 2020, 95, 1213–1221. Giudicessi, J.R.; Noseworthy, P.A.; Friedman, P.A.; Ackerman, M.J. Urgent guidance for navigating and circumventing the QTc-prolonging and torsadogenic potential of possible pharmaco-therapies for Coronavirus Disease 19 (COVID-19). Mayo Clin. Proc. 2020, 95, 1213–1221. [CrossRef]
- Varshneya, M.; Irurzun-Arana, I.; Campana, C.; Dariolli, R.; Gutierrez, A.; Pullinger, T.K.; Sobie, E.A. Investigational treatments for COVID-19 may increase ventricular arrhythmia risk through drug interactions. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 100–107. Varshneya, M.; Irurzun-Arana, I.; Campana, C.; Dariolli, R.; Gutierrez, A.; Pullinger, T.K.; Sobie, E.A. Investigational treatments for COVID-19 may increase ventricular arrhythmia risk through drug interactions. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 100–107. [CrossRef]
- Jenks, J.D.; Mehta, S.R.; Hoenigl, M. Broad spectrum triazoles for invasive mould infections in adults: Which drug and when? Med. Mycol. 2019, 57, S168–S178. Jenks, J.D.; Mehta, S.R.; Hoenigl, M. Broad spectrum triazoles for invasive mould infections in adults: Which drug and when? Med. Mycol. 2019, 57, S168–S178. [CrossRef] [PubMed]
- Gonçalves, S.S.; Stchigel, A.; Cano, J.; Guarro, J.; Colombo, A.L. In vitro antifungal susceptibility of clinically relevant species belonging to Aspergillus section Flavi. Antimicrob. Agents Chemother. 2013, 57, 1944–1947. Gonçalves, S.S.; Stchigel, A.; Cano, J.; Guarro, J.; Colombo, A.L. In vitro antifungal susceptibility of clinically relevant species belonging to Aspergillus section Flavi. Antimicrob. Agents Chemother. 2013, 57, 1944–1947. [CrossRef]
- Aruanno, M.; Glampedakis, E.; Lamoth, F. Echinocandins for the treatment of invasive aspergillosis: From laboratory to bedside. Antimicrob. Agents Chemother. 2019, 63, e00399-19. Aruanno, M.; Glampedakis, E.; Lamoth, F. Echinocandins for the treatment of invasive aspergillosis: From laboratory to bedside. Antimicrob. Agents Chemother. 2019, 63, e00399-19. [CrossRef] [PubMed]
- Ergün, M.; Brüggemann, R.J.M.; Alanio, A.; Delliére, S.; van Arkel, A.; Bentvelsen, R.G.; Rijpstra, T.; van der Sar-van der Brugge, S.; Lagrou, K.; Janssen, N.A.F.; et al. Aspergillus test profiles and mortality in critically Ill COVID-19 patients. J. Clin. Microbiol. 2021, 59, e01229-21. Ergün, M.; Brüggemann, R.J.M.; Alanio, A.; Delliére, S.; van Arkel, A.; Bentvelsen, R.G.; Rijpstra, T.; van der Sar-van der Brugge, S.; Lagrou, K.; Janssen, N.A.F.; et al. Aspergillus test profiles and mortality in critically Ill COVID-19 patients. J. Clin. Microbiol. 2021, 59, e01229-21. [CrossRef] [PubMed]
- Itoh, K.; Tsutani, H.; Iwasaki, H. Multifaceted efficacy of caspofungin against fungal infections in COVID-19 patients. Med. Hypotheses 2022, 164, 110876. Itoh, K.; Tsutani, H.; Iwasaki, H. Multifaceted efficacy of caspofungin against fungal infections in COVID-19 patients. Med. Hypotheses 2022, 164, 110876. [CrossRef] [PubMed]
- Mohamed, A.; Rogers, T.R.; Talento, A.F. COVID-19 Associated invasive pulmonary aspergillosis: Diagnostic and therapeutic challenges. J. Fungi. 2020, 6, 115. Mohamed, A.; Rogers, T.R.; Talento, A.F. COVID-19 Associated invasive pulmonary aspergillosis: Diagnostic and therapeutic challenges. J. Fungi. 2020, 6, 115. [CrossRef] [PubMed]
- Hatzl, S.; Reisinger, A.C.; Posch, F.; Prattes, J.; Stradner, M.; Pilz, S.; Eller, P.; Schoerghuber, M.; Toller, W.; Gorkiewicz, G.; et al. Antifungal prophylaxis 815 for prevention of COVID-19-associated pulmonary aspergillosis in critically ill patients: An observational study. Crit. Care 2021, 25, 335. Hatzl, S.; Reisinger, A.C.; Posch, F.; Prattes, J.; Stradner, M.; Pilz, S.; Eller, P.; Schoerghuber, M.; Toller, W.; Gorkiewicz, G.; et al. Antifungal prophylaxis 815 for prevention of COVID-19-associated pulmonary aspergillosis in critically ill patients: An observational study. Crit. Care 2021, 25, 335. [CrossRef]
More