Metabolic syndrome (MetS) prevalence continues to climb significantly worldwide in today’s ad libitum society. MetS have tremendous societal and economic ramifications, making it imperative to develop effective strategies for preventing and controlling it to alleviate this growing burden. Periodontal disease and MetS are associated with several risk factors. Studies in the past have demonstrated that obesity, cardiovascular illness, and type 2 diabetes mellitus have a negative effect on the severity of periodontal disease. Patients with metabolic syndrome have elevated serum levels of proinflammatory mediators such as tumour necrosis factor-alpha interleukin-6 and C-reactive protein. Remarkably, Intermittent fasting is underpinned by scientific evidence, claiming to be the most effective non-pharmacological, potential therapeutic alternative for combating a wide range of metabolic, inflammatory, and lifestyle-related diseases.
Metabolic syndrome (MetS) prevalence continues to climb significantly worldwide in today’s ad libitum society. MetS have tremendous societal and economic ramifications, making it imperative to develop effective strategies for preventing and controlling it to alleviate this growing burden. Periodontal disease and MetS are associated with several risk factors. Studies in the past have demonstrated that obesity, cardiovascular illness, and type 2 diabetes mellitus have a negative effect on the severity of periodontal disease. Patients with metabolic syndrome have elevated serum levels of proinflammatory mediators such as tumour necrosis factor-alpha interleukin-6 and C-reactive protein. Remarkably, Intermittent fasting is underpinned by scientific evidence, claiming to be the most effective non-pharmacological, potential therapeutic alternative for combating a wide range of metabolic, inflammatory, and lifestyle-related diseases.
Nonetheless, an insufficient investigation has been performed to determine whether intermittent fasting has therapeutic benefits on periodontal inflammation and diseases. Here we show the interrelationship between metabolic syndrome and periodontal disease and contextualize the beneficial impact of intermittent fasting in modulating the chronic metabolic and periodontal inflammatory response. We also anticipate that this review paves the way for further exploration of intermittent fasting as a unique research paradigm representing a cost-effective alternative strategy to conventional disease management in patients with periodontal diseases and metabolic syndrome, which may serve as the foundation for an integrative vision relevant to primary, diagnostic, and therapeutic purposes.
- intermittent fasting
- metabolic syndrome
- calorie restriction
- periodontal diseases
1. Introduction
2. Impact of IF on PD and Mets
2.1. Periodontal Diseases
PD is a chronic inflammatory condition that causes inflammation of the periodontal soft tissues and progressive loss of periodontal ligament and alveolar bone, destroying the tooth-supporting apparatus and potentially resulting in tooth loss [30][42]. Inflammation is the underlying cause of periodontal diseases, and it plays a critical role in their progression. The presence of a considerable number of bacteria might indirectly result in tissue degeneration by activating host defense cells, which produce and release chemical mediators that promote connective tissue breakdown effectors. Microbial plaque components have the ability to cause an initial infiltrate of inflammatory cells such as lymphocytes, macrophages, and polymorphonuclear leukocytes (PMNs). Microbial components, particularly lipopolysaccharide (LPS), stimulate macrophages to produce and secrete a wide range of proinflammatory molecules, including the cytokines, interleukin-1 IL-1, IL-4, IL-10, IFN, TGF and TNF-alpha; prostaglandins, particularly prostaglandin E2 (PGE2); and hydrolytic enzymes. These cytokines have strong proinflammatory and catabolic properties, and they play an important role in the degradation of periodontal tissue through the action of collagenolytic enzymes such as MMPs [31][43]. ROS in the inflammatory environment activates these latent collagenolytic enzymes [32][44]. While it is possible that inflammatory processes originating in one organ induce disorders in another, communication between distant sections of the body and their inflammatory states are accomplished by cells or soluble chemical mediators [30][42]. Significant evidence has been gathered to support comorbidity between PD and other chronic illnesses such as diabetes mellitus, CVS, preterm birth, rheumatoid arthritis, respiratory diseases, chronic kidney diseases, and Alzheimer’s. Figure 1 demonstrates proposed connections between PD and several systemic diseases using schematic representation [13][30][33][34][35][36][13,42,45,46,47,48].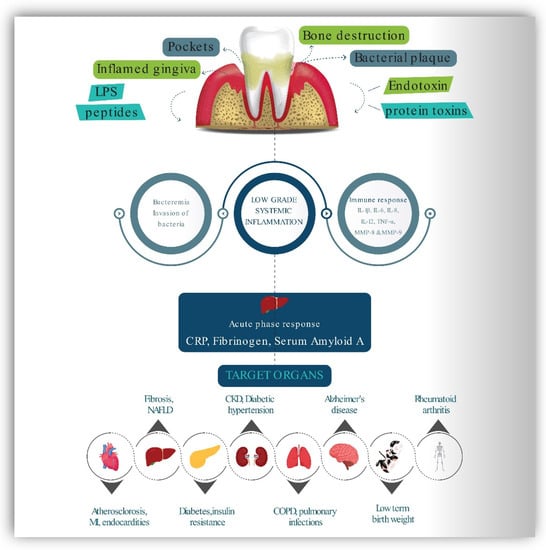
2.2. Activation and Regulation of Periodontal Inflammation by AMPK Pathway and Role of Sirtuins
Oxidative stress is a critical regulator of the systemic pathophysiological effects of PD. SIRT1’s anti-oxidative stress effects in PD have been elucidated. The activation of SIRT1 phosphorylates and activates AMPK, thereby reducing periodontal inflammation-induced oxidative stress. Significantly decreased alveolar tissue damage, enhanced cell viability, and decreased release of proinflammatory cytokines such as IL-1, IL-6, and TNF were found. SIRT 2 was also found to be positively related with nicotinamide phosphorribosyl transferase (NAMPT) activities in human gingival fibroblasts, which were greatly elevated during PD and involved in osteoclast recruitment by promoting the production of cyclooxygenase-2, matrix metalloproteinase (MMP)-1 and MMP-3 [37][49]. In a study involving mice, Chen et al. show that SIRT3 inhibits oxidative stress through controlling PGC-1 and mitochondrial function [38][50]. SIRT6 is also implicated in the regulation of periodontium homeostasis in PD. Huang et al. demonstrated that elevated SIRT6 inhibits cementoblast development and mineralization via inhibiting glucose transporter 1 (GLUT1), a glucose transporter required for cementogenesis, and by activating the AMPK pathway. SIRT6 overexpression improves osteogenic differentiation and reduces LPS-induced inflammatory response through inhibiting the NF-B pathway [39][51]. RWesearchers predicted that fasting may halt the course of PD and lessen systemic oxidative stress through the activation of mitochondrial sirtuins and the AMPK pathway. By reducing oxidative stress, fasting may help prevent alveolar bone loss and inflammatory reactions in the periodontium. The exact roles played by IF at the molecular level to inhibit initiation and progression of PD still require further investigation. However, defining the function and mechanism of fasting in the context of PD may be very helpful for the development of novel therapeutic approaches.2.3. Impact of Intermittent Fasting and Calorie Restriction on Periodontal Inflammation Diseases
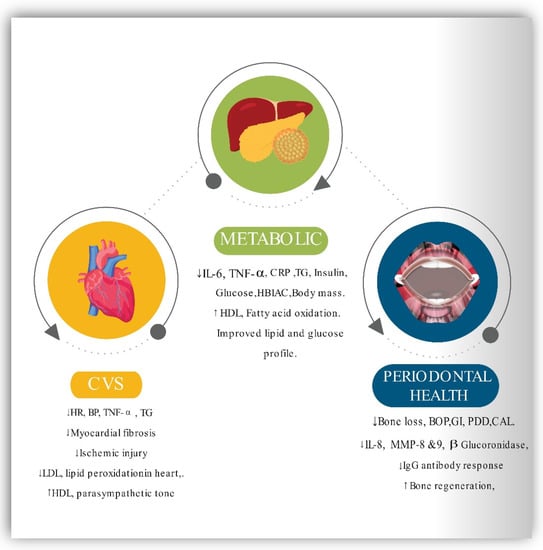
Numerous dietary suggestions that improve periodontal health are vitamin C and vitamin D3 dietary supplements, omega-3 complex supplementation, fiber supplements, antioxidant supplementation, and carbohydrate restriction [40][52]. Regardless of whether persistent plaque is present, anti-inflammatory regimes have been shown to considerably reduce inflammation of gingival tissue [11]. Recent cross-sectional research reveals that healthy body weight, nutritious food, and adequate physical exercise reduce the severity and extent of PD [41][53]. However, in humans, the effect of IF and calorie restriction on periodontal inflammation and infection is scarce. The long-term, irregular, and unpredictable nature of the periodontal disease progression makes disease evaluations extremely difficult. The inflammatory, immunological, kinetic, and disease progression characteristics of active periodontal destruction were studied in different animal studies [42][54]. A recent study [43][55] used an experimental mouse model to assess the positive benefits of IF regimens for periodontal tissues. The authors discovered that fasting regimens resulted in a decreased loss of bone than non-fasting regimens at the ligature-induced PD site and on the contralateral maxillary side. Quantitative computed tomography and calcein-labeled histomorphometric examinations on peripheral bone revealed that the fasted sample subjects had a more excellent capability for regenerating bone than the non-fasted sample group. Additionally, the bone marrow cells of the fasted groups formed more incredible mineralized modules than those of the non-fasted groups [43][55]. Nonhuman primates are ideal animal models for periodontics research owing to their anatomical and biological similarities. The National Institute on Aging on a Rhesus monkey cohort (Macaca mulatta) conducted a longitudinal to ascertain the influence of calorie restriction on the clinical microbiological and immunological aspects of PD. Monkeys were fed twice daily at 6:30 a.m. and 1 p.m. (16 h fasting period and 8 h eating window, 16:8 ratio). For 13–17 years, monkeys were subjected to a 30% drop in dietary consumption of calories compared with a control ad libitum diet group [44][45][46][56,57,58]. The results proved that long-term exposure to CR and time-restricted eating significantly reduced the degree of naturally occurring chronic periodontitis. The CR diet reduced the ligature-induced gingival index (GI), probing pocket depth (PPD), bleeding on probing (BOP), and clinical attachment level (CAL) by a significant amount [44][56]. Another study [46][58] found that the male CR group had significantly decreased depth of the periodontal pocket, substantially lower levels of IgG antibody response, and considerably decreased IL-8 and -glucuronidase levels in GCF in comparison to a control group that received ad libitum meals. However, the male CR group showed a non-significant drop in the IL-1 levels. In the GCF, the female calorie-restricted group had reduced IgG levels of antibodies than the ad libitum group, but both groups had equal levels of markers of inflammation, suggesting that calorie restriction may be beneficial. However, the periodontal microbiota of male and female monkeys was unaffected by a calorie restriction diet [46][58]. In another study conducted to know the antibody responses and also the acute serum host response in rhesus monkeys, it was demonstrated that gender variations in calorie restrictions have an impact on systemic effects. Samples of male monkey serum had higher quantities of haptoglobin and a1-acid glycoprotein than the sample of female monkey serum, according to the findings. Serum IgG antibody responses to Pophyromonas gingivalis, Campylobacter rectus, and Actinomycetemcomitans were significantly increased in the sample of female rhesus monkeys. Antibodies against Fusobacterium nucleatum, however, demonstrated a substantial impact in females on a calorie-restricted regime [45][57]. Recent findings from the first human trial indicated that a specified therapeutically supervised periodic fasting regimen had beneficial effects on inflammation of periodontal tissues in female MetS patients. Bodyweight, waist circumference (WS), body mass index (BMI), BP, fasting plasma glucose (FPG), total cholesterol, CRP, and HDL were all reduced as a result of clinically supervised fasting. At the same time, BOP and GCF levels were also reduced as a result of the fasting [47][59]. As a result, fasting may be recommended as an additional strategy in addition to routine periodontal therapy in obese and overweight individuals who have been diagnosed with periodontitis. Therefore, it will be imperative to conduct many randomized clinical trials in persons who have MetS and periodontal disease in the future. Figure 1 presents a schematic representation of the impact of IF on CVS, metabolic, and the periodontal health2.4. Inflammation and Immune Mediation between PD and MetS
Inflammation contributes a significant part in the initiation of the MetS [48][106]. Numerous studies established correlations between inflammation and obesity. Increased levels of CRP, TNF, IL-6, fibrinogen, and other acute-phase reactants have been documented in obese people [49][50][51][52][53][54][55][107,108,109,110,111,112,113]. Several diseases, such as hyperlipidemia [56][114], PD [57][58][115,116], and type 2 diabetes mellitus [59][117], are correlated with elevated cytokine production. Increased IL-1 levels in GCF [60][118] were observed in patients with insulin depended diabetes and hyperlipidemia, thus, a vicious cycle may develop. Inflammation caused by PD and MetS may further aggravate and exacerbate PD and metabolic sickness [61][62][63][64][119,120,121,122], resulting in impaired metabolic regulation and type 2 diabetes-related problems. [61][119] Furthermore, TNF, a cytokine that causes insulin resistance [65][66][67][68][69][70][123,124,125,126,127,128], is dose-dependent and linked with the severity of PD in adult individuals with insulin-dependent diabetes [71][129]. Thus, the hyper inflammatory state syndrome can amplify the local and systemic inflammatory responses to microbes. The response of the host to the microbial assaults caused by cytokine dysregulation is associated with prolonged TNF expression [72][73][130,131]. According to multiple animal and human studies, diabetes may accelerate alveolar bone disintegration via hyperglycemia-mediated modulation of the receptor activator of nuclear factor-kappa B ligand to osteoprotegerin ratio in periodontal tissues [74][75][76][132,133,134]. The rate of osseous regeneration following bone resorption may be reduced as a result of the death of bone-lining cells and the increased number of fibroblasts [77][78][79][135,136,137]. As a result, all of these factors may have a role in the uncoupling of bone breakdown and healing in periodontal diseases, which are commonly noticed in patients with type 2 diabetes. Increased blood glucose levels result in the formation of advanced glycation end products, which bind to the periodontal receptor for advanced glycation end products (RAGE) and initiate an inflammatory response [80][138]. Blocking the RAGE receptor in diabetic mice reduced the inflammatory response and the subsequent loss of alveolar bone [81][139]. Insulin resistance in PD patients may be associated with the host’s inflammatory response to lipid alterations, obesity, and periodontal diseases [82][140]. Reduced amounts of leptin, an anti-obesity adipocytokine in the gingiva, and GCF can aggravate PD [83][84][85][141,142,143]. However, serum leptin levels, on the other hand, tend to rise as periodontal disease progresses [85][143]. Despite the fact that an in vitro study revealed that adiponectin might have an anti-osteoclastic effect on PD [86][144], evidence for its anti-inflammatory effect between PD and MetS is limited and conflicting [87][88][89][145,146,147]. Resistin is an adipocytokine that is associated with proinflammatory properties [90][148] and is linked to insulin resistance [91][149]. Additionally, when individuals with PD were compared with people who were healthy, there was a link between bleeding on probing and higher levels of serum resistin [88][89][146,147].2.5. Impact of Intermittent Fasting on MetS
As previously stated, short- and long-term IF greatly reduces inflammatory mediator CRP and cytokines such as IL-6 [92][150]. As a result, it is hypothesized that fasting improves the characteristics of MetS via modulating inflammatory responses. Ramadan fasting can decrease TNF- and IL-6 expression in healthy volunteers as it leads to weight loss and decreases body fat percentage [93][151]. In addition, it is hypothesized that TNF- and IL-6 limit lipoprotein lipase (LPL) action, resulting in TNF- and IL-6 down-regulation in fasting individuals, increasing LPL activity and decreasing the fat mass of the body [94][152]. A substantial body of scientific evidence using animal models suggests that IF enhances insulin sensitivity. When fasting or exercising for an extended period of time, the hepatic, cardiac, and skeletal system shift their metabolism to fatty acid oxidation and catabolism of amino acids. However, an energy-dense condition, on the other hand, favors glucose absorption and oxidation [95][153]. IF induces the gene expression that involves lipid storage (PPAR 2 and Fsp27) and fat oxidation (MCPT1), thereby increasing lipogenesis during the IF unrestricted phase and boosting metabolic flexibility and fat oxidation during the fasting period [96][154]. Insulin is critical for glucose homeostasis because it promotes glucose storage. Several explanations have been proposed to elucidate how insulin resistance develops. Prevalent hypotheses suggest that obesity is associated with chronic inflammation, leading to insulin resistance in tissues [97][155]. Growing evidence suggests that obesity is associated with chronic inflammation, which leads to insulin resistance in tissues [96][154]. So, through CR and metabolic reprogramming, IF helps to lower obesity and insulin resistance. Furthermore, various studies have proven that IF results in decreasing levels of leptin and increasing adiponectin, thereby improving insulin resistance [98][156]. Therefore, CR helps individuals to lose weight and improve metabolic health [99][157]. Numerous studies have revealed that humans face difficulties in maintaining daily CR for prolonged periods [100][158]. However, IF has a higher compliance rate and is effective in weight loss and the reduction of obesity-related risk factors for metabolic disease [21][101][102][21,159,160]. Because of the positive effects of fasting, the body uses fatty acids and ketones as fuel. As shown by research, altering one’s metabolic process to one that utilizes fatty acids for energy rather than glucose preserves muscle mass and function while increasing one’s ability to perform daily activities [101][159]. Finally, IF has been shown to reduce adipose tissue mass, notably visceral and abdominal fat, due to its mild energy deficits [103][104][161,162]. This effect has the additional effect of improving the cardiovascular risk profile by lowering BMI and blood pressure, decreasing resting heart rate, decreasing ischemic injury, decreasing lipid peroxidation, and enhancing cardiovascular stress adaptation and resistance to a cardiac muscle injury in myocardial infarction animal models. CVS risk factors are intimately related to MetS components, and intermittent fasting may play a crucial role in the prevention and management of CVD and MetS [25][101][104][25,159,162]. Figure 2 represents the beneficial effects of IF on CVS, metabolic and periodontal health.