Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Allison Jean Stewart and Version 2 by Amina Yu.
Pituitary pars intermedia dysfunction (PPID) is the most common endocrine disorder of geriatric horses, affecting 20–25% of horses over the age of 15 years. Since the disease was first described in 1932, considerable research has been conducted investigating PPID pathophysiology, prevalence of clinical signs, appropriate diagnostic techniques and treatment. In recent years, awareness of PPID among horse owners has grown, and veterinarians are increasingly testing for underlying endocrinopathies. An increase in awareness has led to a substantial increase in research conducted in the field of equine endocrinology.
- endocrine
- geriatric
- hypertrichosis
- insulin dysregulation
- α-melanocyte stimulating hormone (α-MSH)
- proopiomelanocortin (POMC) derived peptides
1. Anatomy and Physiology
The equine pituitary gland is suspended by the infundibular stalk, ventral to the hypothalamus in the sella turcica [1][10]. The pituitary gland is composed of the adenohypophysis (pars distalis, pars intermedia and pars tuberalis), and the neurohypophysis (pars nervosa) [2][11]. In response to physiologic, pathologic or environmentally induced stressors, there is activation of the hypothalamic-pituitary-adrenal axis. This involves the paraventricular dopaminergic neurons of the hypothalamus synthesizing corticotropin-releasing hormone (CRH) which is released in the hypothalamic-hypophyseal portal vessels. There is local action of CRH on the corticotroph cells of the pars distalis, which leads to adrenocorticotropic hormone (ACTH) secretion. Adrenocorticotrophin acts on the zona fasiculata cells of the adrenal glands to synthesise and secrete glucocorticoids. The pars intermedia in horses is composed of melanotrope cells which are directly innervated by hypothalamic periventricular dopaminergic neurons which release dopamine. Dopamine acts on the D2 receptors of the melanotropes to inhibit cell proliferation and transcription of proopiomelanocortin (POMC)POMC [3][4][5][12,13,14]. POMC undergoes processing to produce ACTH, α-MSH, β-END and corticotropin like intermediate lobe peptide (CLIP) [6][7][8][9][10][11][4,15,16,17,18,19]. In the normal equine pituitary gland most ACTH is produced via enzymatic conversion of POMC by prohormone convertase I (PC-1) in the pars distalis [7][15]. ACTH is further cleaved by prohormone convertase 2 (PC-2) to produce α-MSH and CLIP [6][7][8][9][10][11][4,15,16,17,18,19]. β-END is produced via PC-2 conversion of β-lipotropin [12][20] (Figure 1). Melanotrophs are also stimulated by thyrotropin-releasing hormone (TRH) [13][21].
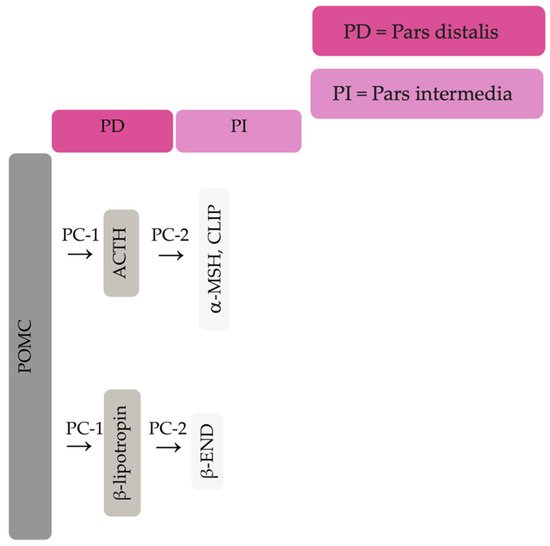
Figure 1. Simplified processing of POMC in the pars distalis by PC-1 to produce ACTH and β-lipotropin. Further PC-2 activity on ACTH and β-lipotropin to produce α-MSH, CLIP and β-END in the pars intermedia.
Closely linked to the hypothalamic-pituitary-adrenal axis is the hypothalamic-pituitary-thyroid axis [14][22]. Endogenous TRH produced by the hypothalamus causes an increase in thyroid stimulating hormone (TSH) produced by the pituitary gland, and an increase in circulating concentrations of thyroxine and triiodothyronine [15][23]. Glucocorticoids exert an inhibitory action on the hypothalamic-pituitary-thyroid axis by reducing TRH secretion by the hypothalamus [16][17][24,25]. Exogenous TRH administration will lead to binding of TRH receptors on the melanotrophs of the pars intermedia and secretion of POMC derived peptides [18][26].
Hypothalamic and pituitary secretions are physiologically influenced by several factors including stress, exercise, illness, photoperiod length, and climate [19][20][21][22][27,28,29,30]. In late summer and autumn, concentrations of α-MSH and ACTH in peripheral blood increase in normal horses, with more pronounced increases in animals with PPID [23][31]. These seasonal changes in ACTH and α-MSH concentrations require seasonally adjusted diagnostic cut-off values to diagnose Pituitary pars intermedia dysfunction (PPID)ID [24][25][2,32].
2. Pathophysiology of PPID
Pituitary pars intermedia dysfunction is one of the most common endocrinopathies in horses; however, the pathophysiology of PPID is incompletely understood [26][27][28][29][30][31][33,34,35,36,37,38]. The disease is caused by loss of dopaminergic inhibition of the pituitary PI due to oxidative-stress and subsequent neurodegeneration of dopaminergic neurons within the hypothalamus [9][32][17,39]. This theory was confirmed recently in a study that aimed to determine whether it was decreased dopamine or dopamine D2 receptor dysfunction that led to PPID. Tyrosine hydroxylase is a biomarker of dopaminergic neurons, and this retrospective study used 28 horses with PPID to measure tyrosine hydroxylase expression within the pars intermedia. A negative correlation between pituitary histomorphological grades and tyrosine hydroxylase was observed, confirming the involvement of reduced dopamine in the pathogenesis of PPID [31][38]. The loss of dopaminergic inhibition on the melanotropes of the pars intermedia results in hyperplasia, microadenoma or macroadenoma formation and overproduction of POMC derived peptides including ACTH and α-MSH (Figure 2) [8][16]. The ACTH secreted by the PI of horses with PPID is largely biologically inactive [9][33][34][17,40,41]. Subsequently, increased plasma ACTH concentrations do not result in adrenal stimulation and hypercortisolaemia [8][9][35][36][37][16,17,42,43,44]. Horses with PPID have resting serum concentrations of free thyroxine and TSH that are lower than age-matched control horses, with normal TSH responses to exogenous TRH administration [16][24]. Because glucocorticoids exert an inhibitory action on the hypothalamic-pituitary-thyroid axis [16][17][24,25], it has been hypothesized that increased glucocorticoid activity does exist, with prolonged tonic suppression of TRH [16][24].
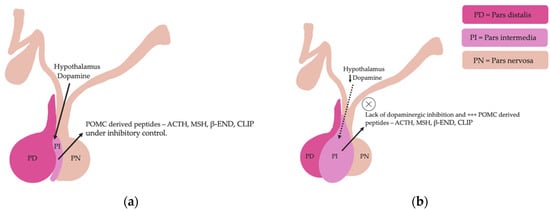
Figure 2. Normal equine pituitary gland (a). Equine pituitary gland affected by PPID demonstrating a loss of dopaminergic inhibition, and subsequent macroadenoma formation of the pituitary pars intermedia and overproduction of POMC derived peptides (b).
Horses with PPID have increased concentrations of α-synuclein in dopaminergic nerve terminals within the pars intermedia compared to healthy geriatric horses [5][38][14,45]. α-synuclein extracted from the pituitary glands of PPID affected horses is misfolded and overexpressed compared to normal and age-matched horses [38][45]. In one study, the ultrastructure of α-synuclein from five each of young, aged and PPID affected horses was assessed using transmission electron microscopy and revealed no α-synuclein fibrils in young and aged horses. However, α-synuclein fibrils were detected in horses with PPID [38][45]. Accumulation of α-synuclein and oxidative stress can lead to cytotoxicity and subsequent degeneration of dopaminergic neurons in humans with Parkinson’s disease [39][46]. Further research is required to determine if misfolded α-synuclein is the cause or result of degeneration of dopaminergic neurons in horses with PPID [38][45].
3. Signalment
Twenty to twenty-five percent of horses over 15 years of age are affected by PPID [6][24][40][2,3,4]. There does not appear to be any sex predilection [6][40][3,4] or any breed predisposition to PPID [40][3]. Previously, despite the high prevalence of PPID in the geriatric equine population, owners were infrequently aware of the disease [6][4]. In 2012, free basal ACTH testing for PPID was well marketed, improving awareness of PPID in both owners and veterinarians [41][8]. However, despite recognising clinical signs, owners may be unlikely to seek veterinary advice [6][4]. Early clinical signs are also easily missed as they can be confused with normal age-related changes [6][42][4,47]. It is not recommended to test horses less than 10 years-of-age unless hypertrichosis is present [8][16] as younger horses are rarely affected by PPID [9][17]. The youngest horses reported with PPID were 7 years of age. This is considered unusual and early onset familial PPID was suspected [9][17].