Magnetic resonance imaging linear accelerators (MRLINAC) technology allows clinicians to leverage imaging information gathered during radiation therapy to adapt therapy for a patient while actively undergoing treatment. There is a significant need to understand how imaging changes may correlate to outcomes during treatment for glioblastoma (GBM) as these tumors have a poor prognosis and treatment tailored to the tumor characteristics may improve outcomes. Some of the advantages of MR guided therapy include facilitating a more detailed study of tumor and normal tissue response during chemo-radiation therapy, providing a mechanism to adapt therapy based on imaging changes, identifying new imaging biomarkers for tumor response as well as normal tissue response. These avenues could provide a more tangible way to evaluate pseudoprogression and radiation necrosis with radiogenomics as a mechanism to correlate imaging findings to genomic biomarkers.
- GBMs
- radiotherapy
- MRI
1. Molecular Basis of Glioblastoma (GBM)
2. Role of Radiotherapy in GBM
3. Types of Radiotherapy Devices for GBM
The role of radiotherapy as a cornerstone of treatment for GBM after surgical resection has been well established. There are multiple techniques available to deliver radiation that have been explored over the years. LINAC—The most common technique utilized is external beam radiotherapy through the use of a linear accelerator (LINAC). LINAC based treatments provide photon radiation. Typical LINACs have on-board imaging capabilities which allow verification with a cone beam CT or kV X-ray image. The on-board imaging is utilized for confirming patient positioning and verifying treatment field shape, is not of diagnostic quality, is low resolution, and is not ideal for visualizing soft tissue such as brain. However, LINAC based treatment remains the standard of care at this time. IORT—Intraoperative radiotherapy (IORT) is a method of radiotherapy that delivers a large single dose of radiation directly to the tumor tissue and resection cavity. In several small and limited studies IORT has been utilized to provide dose escalation, delivering 12–20 Gy intraoperatively with patients subsequently receiving adjuvant radiotherapy as well. The most recent studies in the TMZ era have been relatively small, consisting of approximately 15–50 patients. While these studies have shown manageable rates of toxicity and verified the safety of IORT, they have failed to show meaningful improvements in patient outcomes such as PFS or OS improvements [21][22]. As such, IORT is not a considered a standard of care practice for patients with GBM. GammaTile—GammaTile brachytherapy (GT) is a bioresorbable 3D-collagen tile embedded with Cesium-131 sources which is implanted in the final stages of tumor resection. GT is a relatively new method to treat recurrent brain tumors. A recent study in IDH wildtype GBM treated with maximal safe resection and GT at the time of recurrence demonstrated an overall survival of 20 months for MGMT promoter unmethylated patients and 37 months for MGMT promoter methylated patients. GT safety profile is comparable to patients undergoing repeat surgery without GammaTile [23]. SRS—Stereotactic radiosurgery (SRS) is another method of radiotherapy that entails high dose per fraction irradiation. SRS may be performed with a LINAC or a cobalt source platform that utilizes multiple beams that converge in three dimensions on a small target. Through this technique, a much higher dose may be delivered, which leads to a more ablative treatment, causing higher rates of cell kill and significant damage to tumor vasculature [24][25]. Since a much higher dose is being utilized, it is critical to ensure accurate target localization and tight margins. Due to this, greater spatial resolution is required; therefore, it is recommended that magnetic resonance imaging is co-registered to aid in target volume delineation [26]. At present, stereotactic radiosurgery is commonly utilized in the treatment of brain metastases. There have been multiple prior attempts to establish a role for SRS in the treatment of GBMs, such as in the Radiation Therapy Oncology Group (RTOG) 9305 trial which compared postoperative resection cavity SRS plus external beam radiotherapy vs. resection plus external beam radiotherapy. Unfortunately, there were no significant survival differences or pattern of failure differences between the two arms [27]. As such, the role of SRS for the treatment of GBMs remains controversial and limited. Currently, SRS is most commonly utilized in the setting of recurrent GBM for patients with a high-performance status, a good response to the initial chemoradiotherapy treatment, a prolonged interval to recurrence, and limited volume disease [28]. Protons—Charged particle therapy, particularly proton therapy, has been gaining popularity in the last decade. Proton based radiation imparts a dosimetric benefit, allowing for a more favorable dose distribution, which in turn may reduce patient morbidity. A retrospective analysis comparing photon and proton treatment plans showed that proton therapy provided a dosimetric advantage by reducing dose to organs at risk [29]. Although proton therapy provides a more favorable dosimetry, it is unclear if this translates into improved clinical outcomes or reduced late toxicity. A recent prospective phase II randomized controlled trial compared proton therapy vs. intensity modulated radiotherapy for patients with newly diagnosed GBMs and utilized first cognitive failure as a primary endpoint. Despite the more favorable dosimetry, there were no significant differences in cognitive failure between the treatment arms. Additionally, there were no significant differences in progression free survival or overall survival [30]. Pending results from the NRG BN001 trial [Clinical Trial NCT02179086] will also allow a comparison between proton- and photon-based radiotherapy in the treatment of GBM. Thus far, proton therapy has not yet demonstrated improved treatment efficacy nor reduction in toxicity in the treatment of GBM. MRI guided machine—Soft tissue imaging is critical for successful volume definition in GBM. As already mentioned, for GBM treatment it is necessary to co-register MRI scans to the radiotherapy planning scan in order to have the necessary spatial resolution to properly define the target volume and organs at risk. Furthermore, as image guided radiotherapy has become a mainstay of treatment, there has been a need for better soft tissue image guidance. This has led to the development of MRI guided radiotherapy machines.4. Imaging Characteristics of GBM on MRI
MRI—On MRI, GBMs typically demonstrate contrast-enhanced T1-weighted heterogeneous enhancement and irregular borders, central necrosis, and significant surrounding T2/FLAIR hyperintensity. The increased FLAIR signal in the peritumoral habitat reflects not only edema but also nonenhancing infiltrative tumor. The increased cellularity of these tumors often appears heterogeneously relatively T2-hypointense and may be associated with restricted diffusion. However, a minority of GBMs will manifest as ill-defined nonenhancing, T2/FLAIR hyperintense masses that are difficult to differentiate from low-grade gliomas or as smaller homogeneously enhancing well-defined masses that can be mistaken for metastases. GBMs at the corpus callosum can be difficult to differentiate from lymphoma. Tumefactive multiple sclerosis, infection, and subacute infarcts also can be difficult to differentiate from GBMs or other neoplasms. GBMs typically result in significant mass effect. GBMs can demonstrate increased corrected relative cerebral blood volume (rCBV) on dynamic susceptibility contrast (DSC) MR perfusion, increased permeability on dynamic contrast-enhanced (DCE) MR perfusion, and an abnormal tumor spectrum on MR spectroscopy, with reversal of Hunter’s angle—meaning increased choline (Cho), decreased creatine (Cr) and decreased N-acetyl-aspartase (NAA) (Figure 1).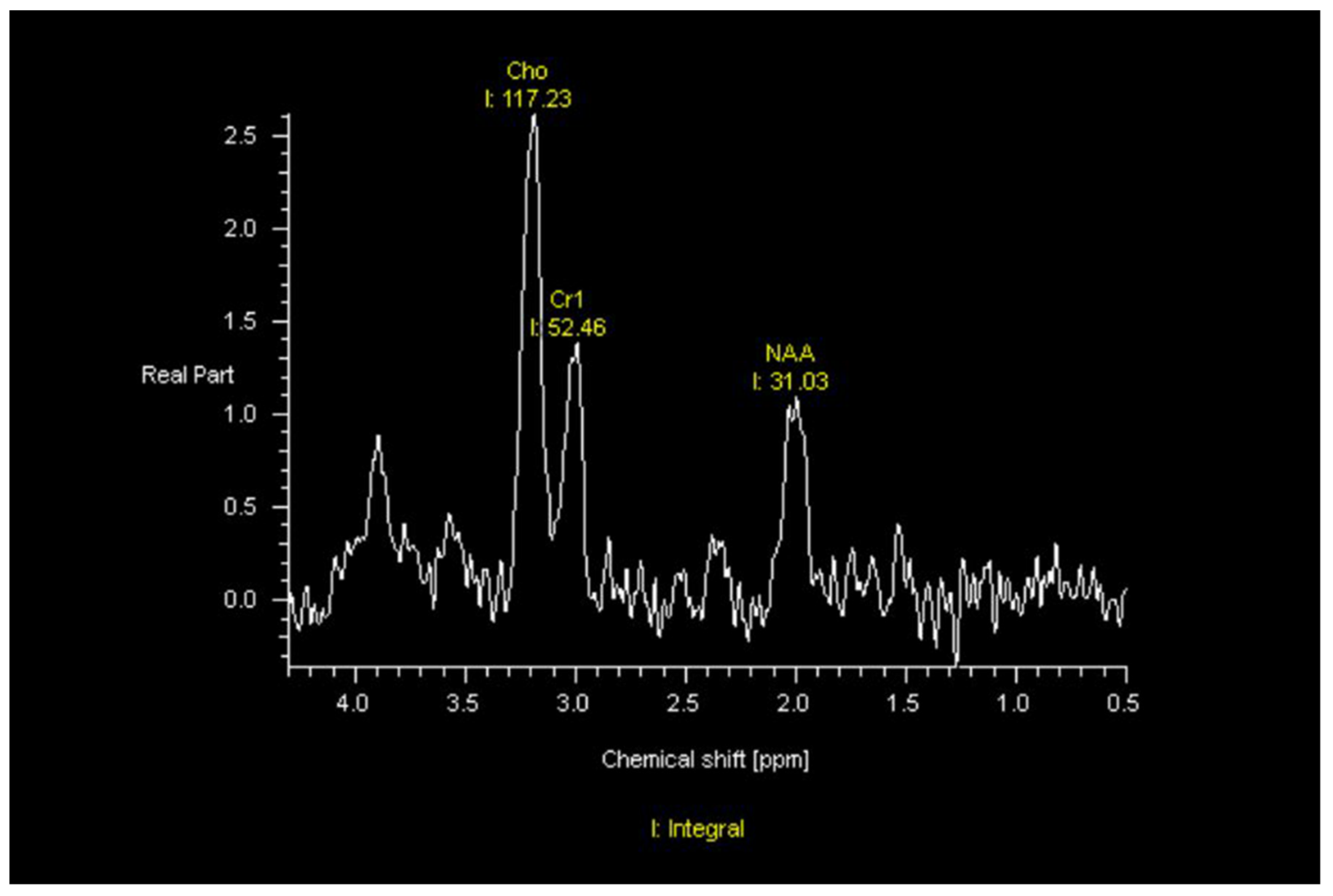
5. Radiomic and Radiogenomic Differentiation of Molecular Markers, Sex Differences, and Morphologic Subtypes of GBMs
6. MRI Guided Machines
Imaging component—Magnetic resonance imaging linear accelerators (MRLINAC) provide improved soft tissue imaging, allowing for superior image guidance and adaptive treatment planning. Combining an MRI system and LINAC is an arduous task with numerous logistical obstacles. Firstly, the MRI imaging system relies on a high-powered magnet, which produces a magnetic field that may hamper the function of the multi-leaf collimator (MLC) of the LINAC [35]. Additionally, a magnetic field may influence the motion of electrons as they travel through the accelerating waveguide [36]. Furthermore, the presence of a LINAC near an MRI system may lead to interaction between the treatment beam and RF receiver coil, causing image quality degradation [37]. There are several different methods of overcoming these obstacles. Currently there are two commercial systems available, with more to come in the future. The Elekta Unity utilizes a 1.5 T magnet, which is the highest-powered magnet commercially available in today’s MRLINACs. To overcome interference from this magnet the photon beam is placed on a rotating gantry which passes a superconducting cryostat configured to avoid angles that will interfere with imaging quality. Additionally, the electron gun is housed in a zero-field zone and utilizes specific shim settings to minimize image degradation [38]. Treatment planning systems are fully integrated into both the Unity and MRIdian, allowing for on-table treatment plan adaptive radiotherapy. This allows treatment to be re-planned in the event of organ motion or with target volume alteration during the course of treatment. In these systems, each daily scan is registered to the primary planning image along with the initial target volumes and organ at risk contours. These volumes can then be adjusted as appropriate. The original treatment plan is subsequently recalculated with an updated Monte Carlo dose calculation that is calibrated to account for the magnetic field as well. The software will provide a dose volume histogram (DVH) comparison of both plans. The user can then determine which plan is preferred, providing the patient with superior target coverage and sparing of organs at risk [39][40].References
- Louis, D.N.; Perry, A.; Wesseling, P.; Brat, D.J.; Cree, I.A.; Figarella-Branger, D.; Hawkins, C.; Ng, H.K.; Pfister, S.M.; Reifenberger, G.; et al. The 2021 WHO Classification of Tumors of the Central Nervous System: A summary. Neuro Oncol. 2021, 23, 1231–1251.
- Labussiere, M.; Boisselier, B.; Mokhtari, K.; Di Stefano, A.L.; Rahimian, A.; Rossetto, M.; Ciccarino, P.; Saulnier, O.; Paterra, R.; Marie, Y.; et al. Combined analysis of TERT, EGFR, and IDH status defines distinct prognostic glioblastoma classes. Neurology 2014, 83, 1200–1206.
- Network, C.G.A.R. Comprehensive genomic characterization defines human glioblastoma genes and core pathways. Nature 2008, 455, 1061–1068.
- Verhaak, R.G.; Hoadley, K.A.; Purdom, E.; Wang, V.; Qi, Y.; Wilkerson, M.D.; Miller, C.R.; Ding, L.; Golub, T.; Mesirov, J.P.; et al. Integrated genomic analysis identifies clinically relevant subtypes of glioblastoma characterized by abnormalities in PDGFRA, IDH1, EGFR, and NF1. Cancer Cell 2010, 17, 98–110.
- Zhang, P.; Xia, Q.; Liu, L.; Li, S.; Dong, L. Current Opinion on Molecular Characterization for GBM Classification in Guiding Clinical Diagnosis, Prognosis, and Therapy. Front. Mol. Biosci. 2020, 7, 562798.
- Wang, Q.; Hu, B.; Hu, X.; Kim, H.; Squatrito, M.; Scarpace, L.; deCarvalho, A.C.; Lyu, S.; Li, P.; Li, Y.; et al. Tumor Evolution of Glioma-Intrinsic Gene Expression Subtypes Associates with Immunological Changes in the Microenvironment. Cancer Cell 2017, 32, 42–56.e46.
- Brennan, C.W.; Verhaak, R.G.; McKenna, A.; Campos, B.; Noushmehr, H.; Salama, S.R.; Zheng, S.; Chakravarty, D.; Sanborn, J.Z.; Berman, S.H.; et al. The somatic genomic landscape of glioblastoma. Cell 2013, 155, 462–477.
- Nie, S.; Zhu, Y.; Yang, J.; Xin, T.; Xue, S.; Sun, J.; Mu, D.; Chen, Z.; Sun, P.; Yu, J.; et al. Clinicopathologic analysis of microscopic tumor extension in glioma for external beam radiotherapy planning. BMC Med. 2021, 19, 269.
- Walker, M.D.; Strike, T.A.; Sheline, G.E. An analysis of dose-effect relationship in the radiotherapy of malignant gliomas. Int. J. Radiat. Onco.l Biol. Phys. 1979, 5, 1725–1731.
- Walker, M.D.; Alexander, E.; Hunt, W.E.; MacCarty, C.S.; Mahaley, M.S.; Mealey, J.; Norrell, H.A.; Owens, G.; Ransohoff, J.; Wilson, C.B.; et al. Evaluation of BCNU and/or radiotherapy in the treatment of anaplastic gliomas. A cooperative clinical trial. J. Neurosurg. 1978, 49, 333–343.
- Walker, M.D.; Alexander, E.; Hunt, W.E.; Leventhal, C.M.; Mahaley, M.S.; Mealey, J.; Norrell, H.A.; Owens, G.; Ransohoff, J.; Wilson, C.B.; et al. Evaluation of mithramycin in the treatment of anaplastic gliomas. J. Neurosurg. 1976, 44, 655–667.
- Walker, M.D.; Strike, T.A. Evaluation of methyl-CCNU, BCNU, and radiotherapy in the treatment of malignant glioma (abstr.). Proc. Am. Assoc. Cancer Res. 1976, 17, 652.
- Nelson, D.F.; Diener-West, M.; Horton, J.; Chang, C.H.; Schoenfeld, D.; Nelson, J.S. Combined modality approach to treatment of malignant gliomas—Re-evaluation of RTOG 7401/ECOG 1374 with long-term follow-up: A joint study of the Radiation Therapy Oncology Group and the Eastern Cooperative Oncology Group. NCI Monogr. 1988, 6, 279–284.
- Murray, K.J.; Nelson, D.F.; Scott, C.; Fischbach, A.J.; Porter, A.; Farnan, N.; Curran, W.J., Jr. Quality-adjusted survival analysis of malignant glioma. Patients treated with twice-daily radiation (RT) and carmustine: A report of Radiation Therapy Oncology Group (RTOG) 83-02. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 453–459.
- Ali, A.N.; Zhang, P.; Yung, W.K.A.; Chen, Y.; Movsas, B.; Urtasun, R.C.; Jones, C.U.; Choi, K.N.; Michalski, J.M.; Fischbach, A.J.; et al. NRG oncology RTOG 9006: A phase III randomized trial of hyperfractionated radiotherapy (RT) and BCNU versus standard RT and BCNU for malignant glioma patients. J. Neurooncol. 2018, 137, 39–47.
- Tsien, C.I.; Brown, D.; Normolle, D.; Schipper, M.; Piert, M.; Junck, L.; Heth, J.; Gomez-Hassan, D.; Ten Haken, R.K.; Chenevert, T.; et al. Concurrent temozolomide and dose-escalated intensity-modulated radiation therapy in newly diagnosed glioblastoma. Clin. Cancer Res. 2012, 18, 273–279.
- Gondi, V.; Pugh, S.; Tsien, C.; Chenevert, T.; Gilbert, M.; Omuro, A.; McDonough, J.; Aldape, K.; Srinivasan, A.; Rogers, C.L.; et al. Radiotherapy (RT) Dose-intensification (DI) Using Intensity-modulated RT (IMRT) versus Standard-dose (SD) RT with Temozolomide (TMZ) in Newly Diagnosed Glioblastoma (GBM): Preliminary Results of NRG Oncology BN001. Int. J. Radiat. Oncol. Biol. Phys. 2020, 108, S22–S23.
- Aydin, H.; Sillenberg, I.; von Lieven, H. Patterns of failure following CT-based 3-D irradiation for malignant glioma. Strahlenther Onkol. 2001, 177, 424–431.
- Wallner, K.E.; Galicich, J.H.; Krol, G.; Arbit, E.; Malkin, M.G. Patterns of failure following treatment for glioblastoma multiforme and anaplastic astrocytoma. Int. J. Radiat. Oncol. Biol. Phys. 1989, 16, 1405–1409.
- Kruser, T.J.; Bosch, W.R.; Badiyan, S.N.; Bovi, J.A.; Ghia, A.J.; Kim, M.M.; Solanki, A.A.; Sachdev, S.; Tsien, C.; Wang, T.J.C.; et al. NRG brain tumor specialists consensus guidelines for glioblastoma contouring. J. Neurooncol. 2019, 143, 157–166.
- Giordano, F.A.; Brehmer, S.; Murle, B.; Welzel, G.; Sperk, E.; Keller, A.; Abo-Madyan, Y.; Scherzinger, E.; Clausen, S.; Schneider, F.; et al. Intraoperative Radiotherapy in Newly Diagnosed Glioblastoma (INTRAGO): An Open-Label, Dose-Escalation Phase I/II Trial. Neurosurgery 2019, 84, 41–49.
- Sarria, G.R.; Sperk, E.; Han, X.; Sarria, G.J.; Wenz, F.; Brehmer, S.; Fu, B.; Min, S.; Zhang, H.; Qin, S.; et al. Intraoperative radiotherapy for glioblastoma: An international pooled analysis. Radiother. Oncol. 2020, 142, 162–167.
- Gessler, D.J.; Neil, E.C.; Shah, R.; Levine, J.; Shanks, J.; Wilke, C.; Reynolds, M.; Zhang, S.; Özütemiz, C.; Gencturk, M.; et al. GammaTile® brachytherapy in the treatment of recurrent glioblastomas. Neurooncol. Adv. 2022, 4, vdab185.
- Guckenberger, M.; Klement, R.J.; Allgauer, M.; Appold, S.; Dieckmann, K.; Ernst, I.; Ganswindt, U.; Holy, R.; Nestle, U.; Nevinny-Stickel, M.; et al. Applicability of the linear-quadratic formalism for modeling local tumor control probability in high dose per fraction stereotactic body radiotherapy for early stage non-small cell lung cancer. Radiother. Oncol. 2013, 109, 13–20.
- Song, C.W.; Kim, M.S.; Cho, L.C.; Dusenbery, K.; Sperduto, P.W. Radiobiological basis of SBRT and SRS. Int. J. Clin. Oncol. 2014, 19, 570–578.
- Soliman, H.; Ruschin, M.; Angelov, L.; Brown, P.D.; Chiang, V.L.S.; Kirkpatrick, J.P.; Lo, S.S.; Mahajan, A.; Oh, K.S.; Sheehan, J.P.; et al. Consensus Contouring Guidelines for Postoperative Completely Resected Cavity Stereotactic Radiosurgery for Brain Metastases. Int. J. Radiat. Oncol. Biol. Phys. 2018, 100, 436–442.
- Souhami, L.; Seiferheld, W.; Brachman, D.; Podgorsak, E.B.; Werner-Wasik, M.; Lustig, R.; Schultz, C.J.; Sause, W.; Okunieff, P.; Buckner, J.; et al. Randomized comparison of stereotactic radiosurgery followed by conventional radiotherapy with carmustine to conventional radiotherapy with carmustine for patients with glioblastoma multiforme: Report of Radiation Therapy Oncology Group 93-05 protocol. Int. J. Radiat. Oncol. Biol. Phys. 2004, 60, 853–860.
- Redmond, K.J.; Mehta, M. Stereotactic Radiosurgery for Glioblastoma. Cureus 2015, 7, e413.
- Harrabi, S.B.; Bougatf, N.; Mohr, A.; Haberer, T.; Herfarth, K.; Combs, S.E.; Debus, J.; Adeberg, S. Dosimetric advantages of proton therapy over conventional radiotherapy with photons in young patients and adults with low-grade glioma. Strahlenther. Onkol. 2016, 192, 759–769.
- Brown, P.D.; Chung, C.; Liu, D.D.; McAvoy, S.; Grosshans, D.; Al Feghali, K.; Mahajan, A.; Li, J.; McGovern, S.L.; McAleer, M.F.; et al. A prospective phase II randomized trial of proton radiotherapy vs intensity-modulated radiotherapy for patients with newly diagnosed glioblastoma. Neuro Oncol. 2021, 23, 1337–1347.
- Snyder, J.M.; Huang, R.Y.; Bai, H.; Rao, V.R.; Cornes, S.; Barnholtz-Sloan, J.S.; Gutman, D.; Fasano, R.; Van Meir, E.G.; Brat, D.; et al. Analysis of morphological characteristics of IDH-mutant/wildtype brain tumors using whole-lesion phenotype analysis. Neurooncol. Adv. 2021, 3, vdab088.
- Bangalore Yogananda, C.G.; Shah, B.R.; Vejdani-Jahromi, M.; Nalawade, S.S.; Murugesan, G.K.; Yu, F.F.; Pinho, M.C.; Wagner, B.C.; Mickey, B.; Patel, T.R.; et al. A novel fully automated MRI-based deep-learning method for classification of IDH mutation status in brain gliomas. Neuro Oncol. 2020, 22, 402–411.
- Yogananda, C.G.B.; Shah, B.R.; Nalawade, S.S.; Murugesan, G.K.; Yu, F.F.; Pinho, M.C.; Wagner, B.C.; Mickey, B.; Patel, T.R.; Fei, B.; et al. MRI-Based Deep-Learning Method for Determining Glioma. AJNR Am. J. Neuroradiol. 2021, 42, 845–852.
- Akbari, H.; Bakas, S.; Pisapia, J.M.; Nasrallah, M.P.; Rozycki, M.; Martinez-Lage, M.; Morrissette, J.J.D.; Dahmane, N.; O’Rourke, D.M.; Davatzikos, C. In vivo evaluation of EGFRvIII mutation in primary glioblastoma patients via complex multiparametric MRI signature. Neuro Oncol. 2018, 20, 1068–1079.
- Yun, J.; St Aubin, J.; Rathee, S.; Fallone, B.G. Brushed permanent magnet DC MLC motor operation in an external magnetic field. Med. Phys. 2010, 37, 2131–2134.
- St Aubin, J.; Santos, D.M.; Steciw, S.; Fallone, B.G. Effect of longitudinal magnetic fields on a simulated in-line 6 MV linac. Med. Phys. 2010, 37, 4916–4923.
- Burke, B.; Wachowicz, K.; Fallone, B.G.; Rathee, S. Effect of radiation induced current on the quality of MR images in an integrated linac-MR system. Med. Phys. 2012, 39, 6139–6147.
- Liney, G.P.; Whelan, B.; Oborn, B.; Barton, M.; Keall, P. MRI-Linear Accelerator Radiotherapy Systems. Clin. Oncol. (R Coll Radiol.) 2018, 30, 686–691.
- Kluter, S. Technical design and concept of a 0.35 T MR-Linac. Clin. Transl. Radiat. Oncol. 2019, 18, 98–101.
- Winkel, D.; Bol, G.H.; Kroon, P.S.; van Asselen, B.; Hackett, S.S.; Werensteijn-Honingh, A.M.; Intven, M.P.W.; Eppinga, W.S.C.; Tijssen, R.H.N.; Kerkmeijer, L.G.W.; et al. Adaptive radiotherapy: The Elekta Unity MR-linac concept. Clin. Transl. Radiat. Oncol. 2019, 18, 54–59.