At high altitudes, the increased adenosine concentration contributes to brain protection against hypoxia through various mechanisms such as stimulation of glycogenolysis for ATP production, reduction in neuronal energy requirements, enhancement in 2,3-bisphosphoglycerate production, and increase in cerebral blood flow secondary to vasodilation of cerebral arteries. In the context of mountain illness, the increased level of A2AR expression leads to glial dysfunction through neuroinflammation and is involved in the pathogenesis of neurological disorders. Nonetheless, a high level of adenosine concentration can protect against high-altitude pulmonary edema via a decrease in pulmonary arterial pressure. The adenosinergic system is also involved in the acclimatization phenomenon induced by prolonged exposure to altitude hypoxia. During hyperoxic exposure, decreased extracellular adenosine and low A2A receptor expression contribute to vasoconstriction. The resulting decrease in cerebral blood flow is considered a preventive phenomenon against cerebral oxygen toxicity through the decrease in oxygen delivery to the brain. With regard to lung oxygen toxicity, hyperoxia leads to an increase in extracellular adenosine, which acts to preserve pulmonary barrier function. Changes in the adenosinergic system induced by exposure to extreme oxygen partial pressures frequently have a benefit in decreasing the risk of adverse effects.
- Adenosine
- hypoxia
- altitude
- hyperoxia
- diving
1. Introduction
1.1. Altitude Hypoxia
The decrease in ambient pressure secondary to the ascent to altitude exposes the body to hypoxia. For example, the partial pressure of O2 decreases from 19.6 KPa at sea level to 6.5 KPa at the summit of Everest. Apart from mountaineers, a significant part of the population lives at an altitude of more than 3000 m with a partial pressure of O2 around 85 to 110 mmHg, with physiopathological consequences [8] involving the adenosinergic system. Acclimatization to severe hypoxia is achieved by an increase in O2 delivery or a decrease in O2 requirements to maintain the critical O2 tension at which cell function is not impaired. Healthy subjects such as climbers and aviators experience hypoxia at high altitudes. In the areas where compensation is possible, the immediate physiological response to hypoxia in healthy subjects includes increases in breathing rate, diuresis and cardiac output, and erythropoiesis when exposure to hypoxia continues for several weeks. Some cells are particularly sensitive to the decrease in partial pressure of O2, such as neurons. Acute hypoxic exposure can lead to impaired cognitive function and sometimes loss of consciousness and seizures. To protect cerebral function, early increases in cerebral blood flow (CBF) occur [9]. The magnitude of the changes in CBF is related to the changes in cerebral vasomotion secondary to hypoxic and hypercapnic ventilatory responses. Hypoxia leads to vasodilation, while hypocapnia induces vasoconstriction. It was reported that brain adenosine blood concentration increases during hypoxia [10]. Furthermore, an increase in APLs is common during hypoxia, ischemia, inflammation, and beta-adrenergic stimulation [1[1][2][11][12][13],2,11,12,13], and was observed in healthy volunteers exposed to altitude hypoxia [14]. The mechanism supporting the increase in APLs in such circumstances is well-documented. An increase in the activity of soluble ecto-5′-nucleotidae (CD73), an enzyme that hydrolyzes AMP into adenosine, was reported. Thus, elevated CD73 contributes to hypoxia-induced adenosine accumulation [15]. Previous studies have supported the contribution of increased extracellular adenosine concentration to protecting the brain from hypoxia [2,21][2][16]. This protection includes the stimulation of glycogenolysis for ATP production via anaerobic glycolysis and the reduction in neuronal energy requirements [22][17]. Furthermore, the increase in APLs and CD73 activity can increase via A2B receptor activation, 2,3-bisphosphoglycerate (2,3-BPG) production, which decreases the affinity of hemoglobin for dioxygen, promoting O2 delivery to tissues [15]; see Figure 1.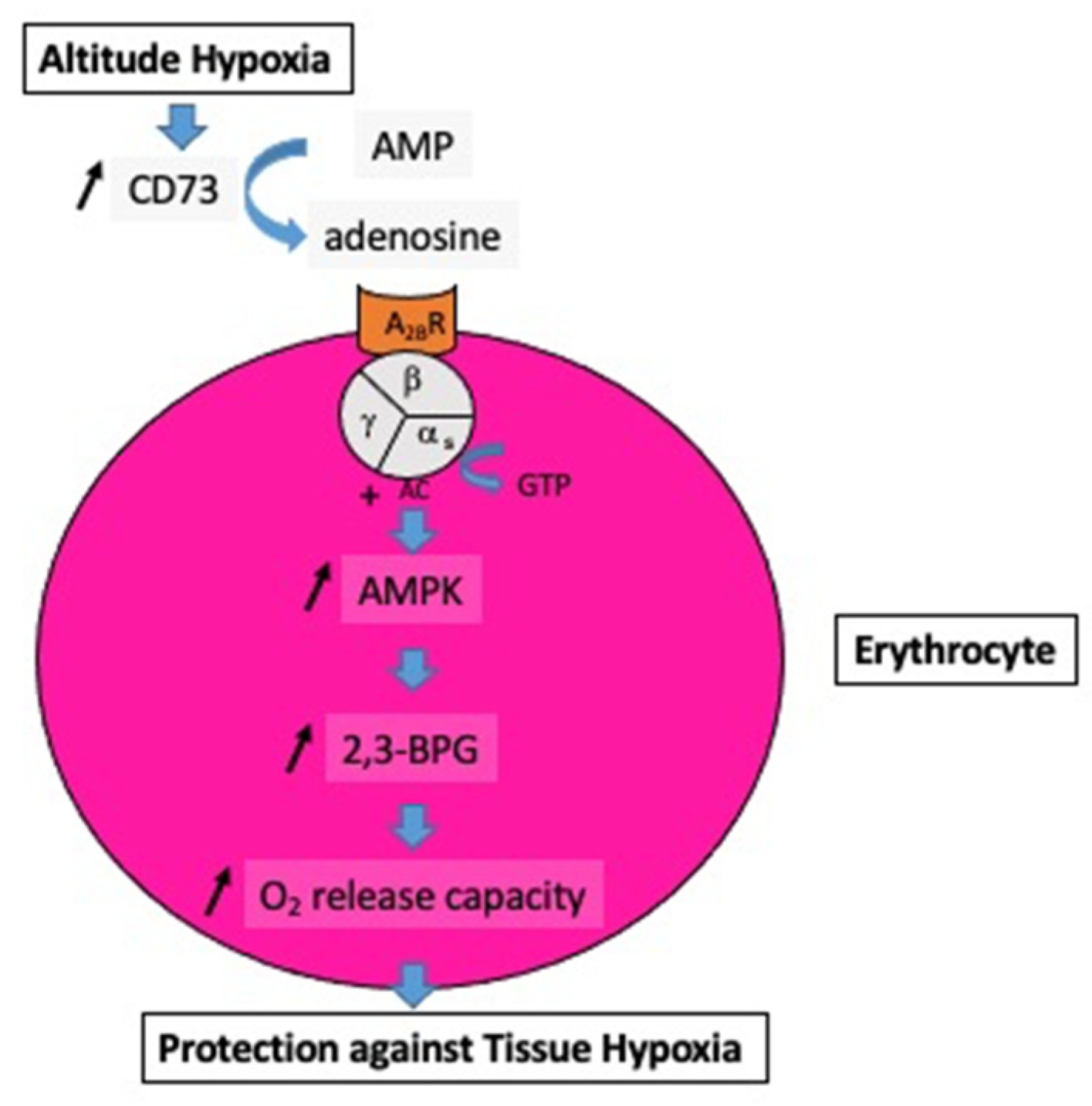
1.2. Acute Altitude Illness
1.3. Chronic Hypoxia: Life at Altitude
Prolonged exposure to altitude hypoxia is known to result in the development of an acclimatization phenomenon. In a human study, Song et al. [14] reported that the adenosinergic-signaling network enhanced the hypoxia adenosine response to counteract hypoxia-induced maladaptation. They measured APLs and soluble CD73 activity in healthy subjects at sea level and during a stay at high altitudes (5260 m). The volunteers returned for several days (from 7–21 days) at 1525 m, and a further blood sample was collected upon re-ascent at 5260 m. The autscholars found that APLs and CD73 activity were significantly higher upon re-ascent to 5260 m for 1 day, after spending several days at 1525 m, compared with the first hypoxia exposure. Consequently, the first stay at high altitude can enhance the defense response to hypoxia through an increase in APLs and CD73 activity. Although adenosine production is activated during prolonged stays at high altitudes, its action on the artery decreases. Calbet et al. [40][21] reported that short-term residence at altitude (between 8 and 12 days at 4554 m) induced an increase in resting blood pressure. Vasodilatory responses secondary to exogenous adenosine infusion were impaired by alteration in endothelial function. Thus, chronic or acute exposures to a high endogenous adenosine extracellular concentration may have different effects on the cardiovascular system.2. Hyperoxia
In hyperbaric conditions, subjects breathe a mixture of high-pressure gases through a regulator. Most frequently, diving tanks contain compressed air (filtered and dehumidified), i.e., 78% nitrogen, 20.9% oxygen, and small proportions of trace gases. The increase in ambient pressure generates an increase in the partial pressures of oxygen and nitrogen. Furthermore, the gas density is increased. Some divers inhale oxygen-enriched gas mixtures to decrease the nitrogen content of tissues and blood at the time of decompression and to limit the occurrence of decompression sickness. For an air dive, the partial pressure of O2 is 40 KPa at 10 m depth and 60 KPa at 20 m depth. In the particular case of military diving, the use of pure oxygen through a closed-circuit self-contained underwater breathing apparatus (SCUBA) allows better self-sufficiency (the exhaled gas is reused after the CO2 is extracted by lime) and discretion (no bubbles). Consequently, hyperoxia is a constant stressor for healthy subjects working in hyperbaria, such as SCUBA divers or professional workers in a tunnel boring machine hyperbaric chamber.2.1. Cardio-Vascular Changes
Hyperoxic exposure has a major impact on cardiovascular function in healthy subjects. Numerous studies have shown that cardiovascular responses to acute hyperoxia include a decrease in cardiac output related to the simultaneous decreases in heart rate and stroke volume [41,42,43][22][23][24]. Increases in mean blood pressure and systemic vascular resistance, and a decrease in arterial compliance, have been documented in resting healthy volunteers breathing pure oxygen [41,44,45][22][25][26]. Such an effect of oxygen appears to be related to its vasoconstrictive action on the peripheral vascular system. The exact mechanism by which hyperoxia induces vasoconstriction is not fully understood. The increase in partial pressure of O2 and the production of reactive oxygen species can contribute to arterial vasoconstriction through an alteration in endothelial function or a direct effect on the vascular smooth muscle [46,47][27][28].2.2. Oxygen Toxicity
Retinal toxicity is one of the first indicators of hyperoxia [51][29]. From this perspective, the lack of A1R reduced hyperoxia-induced retinal toxicity in mice [52][30], suggesting that A1R activation did not protect against hyperoxia-induced retinal toxicity. Brain oxygen toxicity is linked to oxidative stress induced by hyperoxia. Damage is secondary to increased production of reactive oxygen species (ROS) and/or reactive nitrogen species and lipid peroxidation, which impair cell membranes [53][31]. Clinical disorders include disturbances of vision (tunnel vision), headache, nausea, muscle twitching, and convulsions similar to epileptic seizures with loss of consciousness [54][32]. It has long been known that prolonged exposure to hyperoxia can lead to lung damage (Lorrain-Smith effect) [59][33]. Pulmonary disorders consist of three successive phases, i.e., inflammatory, proliferative-reparative, and fibrotic. The severity is positively correlated with the duration of exposure and the level of partial pressure of O2. Hyperoxia can disrupt the structure and function of the pulmonary epithelial barrier through the destruction of the pulmonary epithelial tight junction structures (see Figure 2).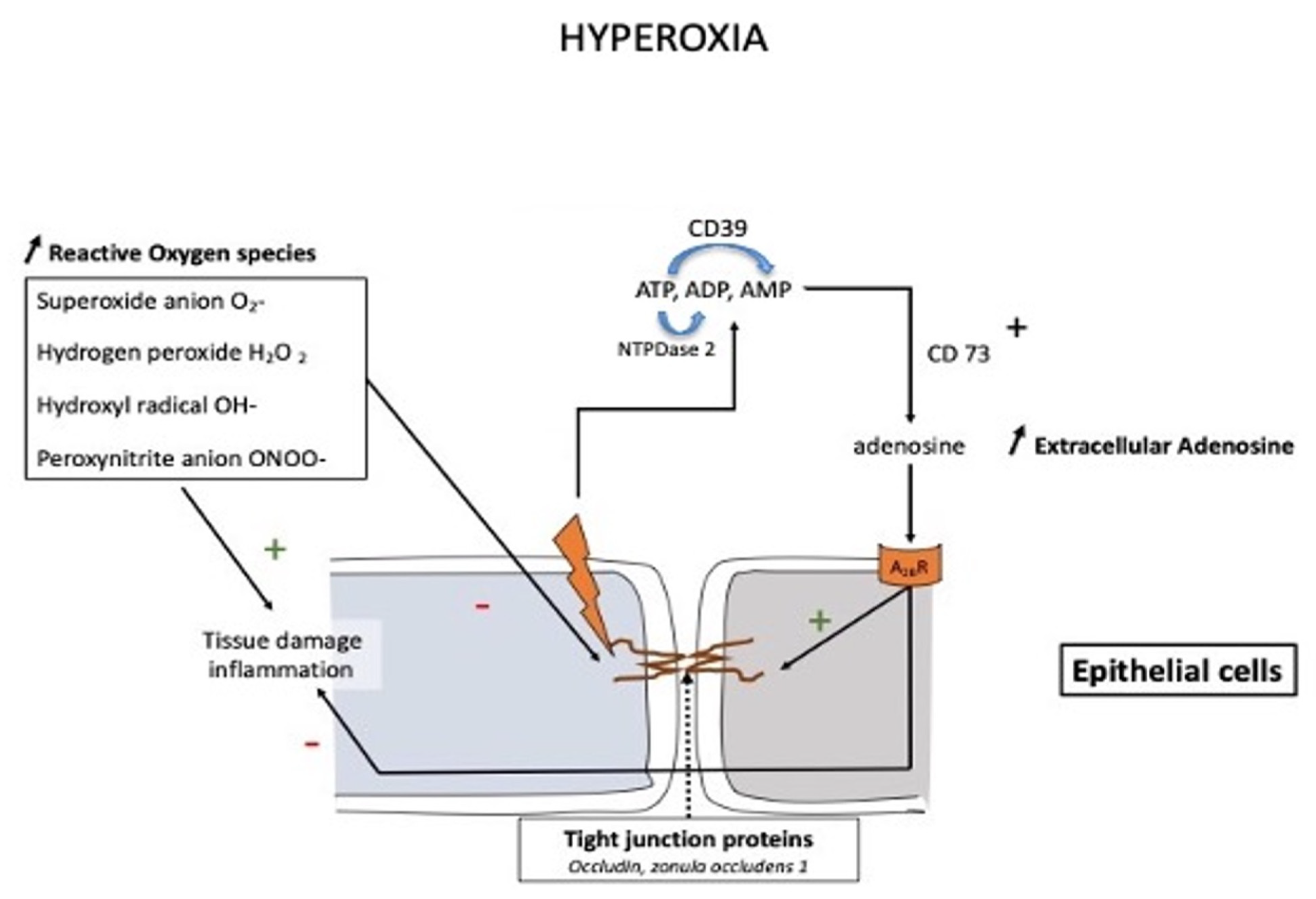
3. Conclusions
References
- Grenz, A.; Homann, D.; Eltzschig, H.K. Extracellular adenosine: A safety signal that dampens hypoxia-induced inflammation during ischemia. Antioxid. Redox. Signal. 2011, 15, 2221–2234.
- Eltzschig, H.K.; Karhausen, J.; Kempf, V.A. Acute oxygen-sensing mechanisms. N. Engl. J. Med. 2006, 354, 975–977.
- Joulia, F.; Coulange, M.; Lemaitre, F.; Costalat, G.; Franceschi, F.; Gariboldi, V.; Nee, L.; Fromonot, J.; Bruzzese, L.; Gravier, G.; et al. Plasma adenosine release is associated with bradycardia and transient loss of consciousness during experimental breath-hold diving. Int. J. Cardiol. 2013, 168, e138–e141.
- Bruzzese, L.; Rostain, J.C.; Née, L.; Condo, J.; Mottola, G.; Adjriou, N.; Mercier, L.; Berge-Lefranc, J.L.; Fromonot, J.; Kipson, N.; et al. Effect of hyperoxic and hyperbaric conditions on the adenosinergic pathway and CD26 expression in rat. J. Appl. Physiol. 2015, 119, 140–147.
- Fromonot, J.; Chaumet, G.; Gavarry, O.; Rostain, J.C.; Lucciano, M.; Joulia, F.; Brignole, M.; Deharo, J.C.; Guieu, R.; Boussuges, A. Hyperoxia Improves Hemodynamic Status During Head-up Tilt Testing in Healthy Volunteers: A Randomized Study. Medicine 2016, 95, e2876.
- Morote-Garcia, J.C.; Rosenberger, P.; Kuhlicke, J.; Eltzschig, H.K. HIF-1-dependent repression of adenosine kinase attenuates hypoxia-induced vascular leak. Blood 2008, 111, 5571–5580.
- Hellsten, Y.; Nyberg, M.; Mortensen, S.P. Contribution of intravascular versus interstitial purines and nitric oxide in the regulation of exercise hyperaemia in humans. J. Physiol. 2012, 590, 5015–5023.
- Peacock, A.J. ABC of oxygen: Oxygen at high altitude. BMJ 1998, 317, 1063–1066.
- Brugniaux, J.V.; Hodges, A.N.; Hanly, P.J.; Poulin, M.J. Cerebrovascular responses to altitude. Respir. Physiol. Neurobiol. 2007, 158, 212–223.
- Winn, H.R.; Rubio, R.; Berne, R.M. Brain adenosine concentration during hypoxia in rats. Am. J. Physiol. 1981, 241, H235–H242.
- Le, G.; Essackjee, H.; Ballard, H. Intracellular adenosine formation and release by freshly-isolated vascular endothelial cells from rat skeletal muscle: Effects of hypoxia and/or acidosis. Biochem. Biophys. Res. Commun. 2014, 450, 93–98.
- Idzko, M.; Ferrari, D.; Eltzschig, H.K. Nucleotide signalling during inflammation. Nature 2014, 509, 310–317.
- Sumi, Y.; Woehrle, T.; Chen, Y.; Yao, Y.; Li, A.; Junger, W.G. Adrenergic receptor activation involves ATP release and feedback through purinergic receptors. Am. J. Physiol. Physiol. 2010, 299, C1118–C1126.
- Song, A.; Zhang, Y.; Han, L.; Yegutkin, G.G.; Liu, H.; Sun, K.; D’Alessandro, A.; Li, J.; Karmouty-Quintana, H.; Iriyama, T.; et al. Erythrocytes retain hypoxic adenosine response for faster acclimatization upon re-ascent. Nat. Commun. 2017, 8, 14108.
- Liu, H.; Zhang, Y.; Wu, H.; D’Alessandro, A.; Yegutkin, G.G.; Song, A.; Sun, K.; Li, J.; Cheng, N.Y.; Huang, A.; et al. Beneficial Role of Erythrocyte Adenosine A2B Receptor-Mediated AMP-Activated Protein Kinase Activation in High-Altitude Hypoxia. Circulation 2016, 134, 405–421.
- Görlach, A. Control of adenosine transport by hypoxia. Circ. Res. 2005, 97, 1–3.
- Laborit, H.; Bonifacj, J.F. Action of adenosine on energy metabolism and on glucose-6-phosphate dehydrogenase in rat brains. Res. Commun. Chem. Pathol. Pharmacol. 1984, 44, 123–130.
- West, J.B. High-altitude medicine. Lancet Respir. Med. 2015, 3, 12–13.
- Salys, J.; Kratzer, A.; Zamora, M.; Taraseviciene-Stewart, L. Hypoxia-mediated alterations in adenosine receptor expression in rat lung. Eur. Respir. J. 2011, 38, 333.
- Sharma Kandel, R.; Mishra, R.; Gautam, J.; Alaref, A.; Hassan, A.; Jahan, N. Patchy vasoconstriction versus inflammation: A debate in the pathogenesis of high altitude pulmonary edema. Cureus 2020, 12, e10371.
- Calbet, J.A.; Boushel, R.; Robach, P.; Hellsten, Y.; Saltin, B.; Lundby, C. Chronic hypoxia increases arterial blood pressure and reduces adenosine and ATP induced vasodilatation in skeletal muscle in healthy humans. Acta Physiol. 2014, 211, 574–584.
- Waring, W.; Thomson, A.; Adwani, S.; Rosseel, A.; Potter, J.; Webb, D.; Maxwell, S. Cardiovascular effects of acute oxygen administration in healthy adults. J. Cardiovasc. Pharmacol. 2003, 42, 245–250.
- Molenat, F.; Boussuges, A.; Grandfond, A.; Rostain, J.C.; Sainty, J.M.; Robinet, C.; Galland, F.; Meliet, J.L. Modifications of cardiovascular function secondary to hyperbaric hyperoxia in healthy volunteers: An Echocardiographic and Doppler study. Clin. Sci. 2004, 106, 389–395.
- Gole, Y.; Gargne, O.; Coulange, M.; Steinberg, J.G.; Bouhaddi, M.; Jammes, Y.; Regnard, J.; Boussuges, A. Hyperoxia-induced alterations in cardiovascular function and autonomic control during return to normoxic breathing. Eur. J. Appl. Physiol. 2011, 111, 937–946.
- Harten, J.M.; Anderson, K.J.; Angerson, W.J.; Booth, M.G.; Kinsella, J. The effect of normobaric hyperoxia on cardiac index in healthy awake volunteers. Anaesthesia 2003, 58, 885–888.
- Rossi, P.; Boussuges, A. Hyperoxia-induced arterial compliance decrease in healthy man. Clin. Physiol. Funct. Imag. 2005, 25, 10–15.
- Rubanyi, G.M.; Vanhoutte, P.M. Superoxide anions and hyperoxia inactivate endothelium derived relaxing factor. Am. J. Physiol. 1986, 250, H822–H827.
- Welsh, D.G.; Jackson, W.F.; Segal, S.S. Oxygen induces electromechanical coupling in arteriolar smooth muscle cells: A role for L-type Ca2+ channels. Am. J. Physiol. 1998, 274, H2018–H2024.
- Scott, A.; Fruttiger, M. Oxygen-induced retinopathy: A model for vascular pathology in the retina. Eye 2010, 24, 416–421.
- Zhang, S.; Li, H.; Li, B.; Zhong, D.; Gu, X.; Tang, L.; Wang, Y.; Wang, C.; Zhou, R.; Li, Y.; et al. Adenosine A1 Receptors Selectively Modulate Oxygen-Induced Retinopathy at the Hyperoxic and Hypoxic Phases by Distinct Cellular Mechanisms. Investig. Ophthalmol Vis. Sci. 2015, 56, 8108–8119.
- Ottolenghi, S.; Sabbatini, G.; Brizzolari, A.; Samaja, M.; Chiumello, D. Hyperoxia and oxidative stress in anesthesia and critical care medicine. Minerva Anestesiol. 2020, 86, 64–75.
- Arieli, R.; Arieli, Y.; Daskalovic, Y.; Eynan, M.; Abramovich, A. CNS oxygen toxicity in closed-circuit diving: Signs and symptoms before loss of consciousness. Aviat. Space Environ. Med. 2006, 77, 1153–1157.
- Jones, M.W.; Brett, K.; Han, N.; Wyatt, H.A. Hyperbaric Physics; StatPearls Publishing: Treasure Island, FL, USA, 2017.