Iodine is one of the 30 essential elements for life, and its chemical speciation defines its biological activities. Both inorganic and organic chemical species have crucial roles in the biology of most living organisms. The most relevant inorganic species are iodate (IO3−) and iodide (I−), as the major sources of iodine for living beings, together with molecular iodine (I2) and hypoiodous acid (HIO) as the most reactive performing catalytic activities. Conversely, Thyroid Hormones (THs) are the master regulators of the metabolism of vertebrates and the representative organic species. Mainly inorganic species are exploited in the health science industry to produce disinfectants, supplements, medicines, and X-ray contrast media.
- iodine species
- iodide
- molecular iodine
- thyroid hormones
1. Introduction
2. History and Chemical Characteristics
In 1811, the French chemist Bernard Courtois discovered iodine when he tried to obtain saltpeter from seaweed and accidentally added too much sulfuric acid to the mixture, producing a purple vapor. Two years later, iodine was recognized as a new element receiving its name from the Ancient Greek term “οειδής” or “ioeides” which means violet [8]. The periodic table represents iodine by the I letter, which has an atomic number of 53, an atomic mass of 126.9045 Da, and belongs to group 17 of halogens [9]. There are 37 known isotopes of the element with masses from 108 to 144 (108I – 144I). Most are artificially produced and lose energy via radiation (radiation decay) in days, hours, or less,; except for Iodine-127 ( 127I), the natural and only 100% stable isotope. Iodine 129 (, and 129I), with a half-life of 15.7 million years, can also be which is naturally produced in traces by spontaneous fission and cosmic-ray reactions (see applications of radioisotopes in section 6.3 and 6.4) [10][11]. Iodine lacks an electron to fulfill the valence shell; hence, it cannot exist in nature as a free element (neutral atom) because of its high reactivity and electronegativity (2.66 on the Pauling scale). Instead, the diatomic form of I2, formed by a nonpolar covalent bond between two iodine atoms, is recognized as the stable state of the element [9][12]. Likewise, iodine can combine with most elements (except noble gases and most synthetic elements), yielding broad inorganic and organic chemiocal forms (iodine species. Those chemical species d) with oxidation states of −1, 0, +1, +3, +5, and +7, distributed along the lithosphere, hydrosphere, and atmosphere with diverse oxidation states (−1, 0, +1, +3, +5, and +7) [9]e.3. Distribution of Iodine
In the Earth’s crust, the richest inorganic source of iodine is oceanic sediments (68.2%) and continental sedimentary rocks (27.7%), followed by igneous and metamorphic rocks (2.7%), seawater (0.81%), and mafic oceanic crust (0.68%) [13]. In the atmosphere, sea spray aerosolization, volcanic gases, and human activities contribute to iodine emissions., However,but the highest discharge is given by biological conversion to volatile methyl forms, such as methyl iodide (CH3I). Cycling of iodine involves biotic and abiotic processes through the lithosphere, hydrosphere, and atmosphere. Into seawater, iodine species are cycled during subduction of the oceanic crust (descending of a tectonic plate below another) and via decomposition of marine organisms. In contrast,; whereas the flux from the atmosphere to the lithosphere occurs during rainfall, wet deposition, leaching, and runoff [13][14][15]. Furthermore, many living organisms an important amount of iodine is accumulated and use a significant amount of iodined by many living organisms, including algae, plants, corals, sponges, anemones, lobworms, shellfishes, arthropods, and bacteria, that cycle organic and inorganic iodine species in the biosphere (Figure 1) [15].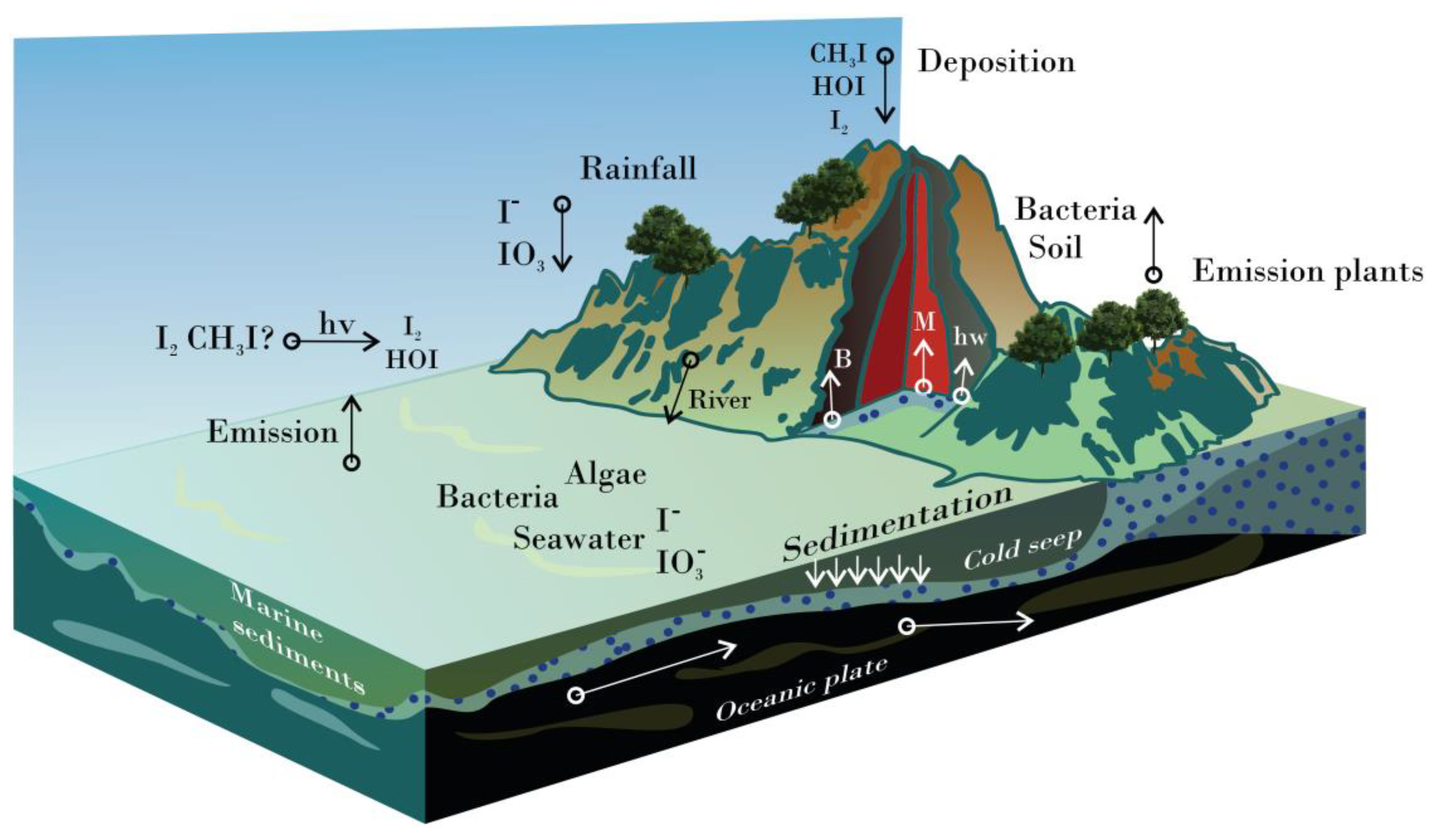
4. Relevant Iodine Species
4.1. Main Inorganic Forms
Dominant iodine species in solid-state are potassium iodate (KIO3) and potassium iodide (KI), whereas IO3- and I- ions lead to aqueous systems [19]. I2 and CH3I are the most abundant species in the atmosphere, produced by biotic and abiotic processes [20]. Atmospheric photochemistry promotes the speciation of gaseous iodine species (e.g., HI, IO-, HOI, IONO2 INO2, and IO2) [21][22]. Some of them (mainly I2 and HOI), together with other halogen compounds, are responsible for ozone (O3) depletion in the lower troposphere when interacting with hydrogen-oxygen species and nitrogen oxides [23].
In general terms, all iodine species formed in aqueous solutions are relevant for the biological systems. Up to 10 different iodine species can be formed when I2 and I- combine in an aqueous solution (reactions 1-9), where the chemical speciation is highly influenced by iodide amount [c(I-)], pH, and redox potential (Eh) (Fig. 2A) [24][25][26]. An excellent example is Lugol’s solution (typically made of 5% I2 and 10% KI), used as a disinfectant and for other commercial purposes (see sections 5 and 6.1). Under those conditions, I2, I-, triiodide (I3–), pentaiodide (I5–), and hexaiodide (I62–) coexist. I2 is the most reactive of those, showing several biological activities, I3– is responsible for staining, and I5–/I62– barely represents ~8% of the oxidizing potential [26]. However, only I-, I2, and I3- are formed and available in significant amounts under physiological conditions [26][27].I2 + H2O ↔ HIO + I− + H+. (1)
HIO ↔ OI− + H+. (2)
I2 + I− ↔ I3−. (3)
HIO + H+ ↔ H2OI+. (4)
I3− + I2 ↔ I5-. (5)
2I3− ↔ I62−. (6)
OI− + I- +H2O ↔ HIO2- + OH-. (7)
HIO2- ↔ I2O- + H+. (8)
3HIO ↔ IO3- + 2I- + H+. (9)
4.2. Representative Organic Species
Thyroid hormones (THs) are the protagonists of organic iodine species because of their hormonal role in vertebrate animals. THs comprise i) 3-iodotyrosine or monoiodotyrosine (MIT or T1) and 3,5-diiodotyrosine (DIT) as precursors; ii) 3’,5,3-triiodothyronine (T3) and thyroxine (T4), typically considered as the active hormones; and iii) 3’,5’,3 triiodothyronine or reverse T3 (rT3), 3’,5’ diiodotyrosine (3’,5’-DIT), and 3’- monoiodotyrosine (3’-MIT), the T4 derivatives [28][29]. Other THs derivatives include thyronamines (TAMs) and thyroacetic acids like 3,3',5-triiodothyroacetic acid (Triac), and 3,3′,5,5′-tetraiodothyroacetic acid (Tetrac) produced by deiodination and decarboxylation [29].
Thyroid Peroxidase (TPO) is the enzyme responsible for synthesizing THs using thyroglobulin (TG) as a substrate. TG is, the main iodinated compound in the thyroid gland [30][31][32]. The sequence forllowed in TH production is TPO incorporatesing one iodine atom into Tyr residues at position 3 of the ring to produce MIT (reaction 10) and then at position 5 to form DIT (reaction 11). Subsequently, T3 is constructed by an oxidative coupling reaction between one DIT and one MIT (reaction 12), still incorporated into the TG. At the same time, T4 is formed by coupling two adjacent DITs (reaction 13). At the end of the process, only 37 of the ~70 Tyr residues in the TG are known iodination targets [30][31]. Most MITs and DITs produced are kept in the thyroid follicellles and are eventually degraded by iodotyrosine deiodinases (IYD) enzymes into MIT and Tyr (T0), respectively (reactions 14 and 15) [33]. Meainwhile, T3 and T4 are transported into the bloodstream, mostly bound to plasma proteins. Just a fraction of T3 (21.8%) is synthesized and released in the same fashion as T4; most of it is generated by the deiodination of T4 out of the thyroid by two kinds of iodothyronine deiodinases (ID) (Reaction (16)) [34][35]. A different iodothyronine deiodinase transforms T4 into rT3 (Reaction (17)), an inactive TH produced to maintain hormone homeostasis [36].
Tyr residue + I
(10) Tyr residue + I
−
+ H
2
O
2
+ H
+
+ TPO → MIT + 2H
2O + TPO. (10)
O + TPO.
MIT + I− + H
(11) MIT + I− + H
2
O
2
+ H
+ + TPO → DIT + 2H2O + TPO. (11)
+ TPO → DIT + 2H2O + TPO.
MIT + DIT + H
(12) MIT + DIT + H
2
O
2
+ H
+
+ TPO → T3 + 2H
2O + TG (dehydroalanine). (12)
O + TG (dehydroalanine).
2DIT + I
(13) 2DIT + I
−
+ H
2
O
2
+ H
+
+ TPO → T4 + 2H
2O + TG (dehydroalanine). (13)
O + TG (dehydroalanine).
DIT + NADPH + IYD → MIT + NADP
(14) DIT + NADPH + IYD → MIT + NADP
+
+ I
− + IYD. (14)
+ IYD.
MIT + NADPH + IYD → Tyr + NADP
(15) MIT + NADPH + IYD → Tyr + NADP
+
+ I
− + IYD. (15)
+ IYD.
T4 + NADPH + ID→ T3 + NADP
(16) T4 + NADPH + ID→ T3 + NADP
+
+ I
− + ID. (16)
+ ID.
T4 + NADPH + ID→ rT3 + NADP
(17) T4 + NADPH + ID→ rT3 + NADP
+
+ I
− + ID. (17)
+ ID.
TPO is also responsible for the iodination of lipids (iodolipids) as α-IHDA and 6-IL. Noticeably, 6-IL was recently related to the antioxidant, anti-inflammatory, and anticarcinogenic activities [37][38]. Other peroxidase enzymes like Lactoperoxidase (LPO) are responsible for the synthesis of iodolactones (e.g., δ-lactone of 6-iodo-4-hydroxy-eicosa-8,11,14-trienoic acid, and ε-lactone of 5-iodo-4-hydroxy-7-docosapentaenoic acid) using docosahexaenoic acid (DHA) as a substrate [39].
5. Iodine in the Industry
Molecular iodine is one the most exploited chemicals in the industry, mainly as a catalyst for organic synthesis (including many heterocyclic compounds used in pharmacy), because of its low cost, efficiency, and high selectivity [40]. I− is considered a mild reducing agent and , and it is a much less reactive species than I2. IO3− is less reactive and has low toxicology; together with I−, it can also be used as a chemical reagent or serve as an ingredient for various products (e.g., supplements and iodophors) [12][41]. Hydrogen iodide (HI), iodine pentoxide (I2O5), iodic acid (HIO3), and sodium periodate (NaIO4) are other frequent chemicals used in the pharmaceutical industry for organic synthesis [42][43]. In this research, the chemical synthesis is not addressed, but it is recommended to consult Küpper et al. (2011) and Wang et al. (2021). Historically, Lugol’s solution has been one of the most used iodine-based products in medicine and the industry. It was first used in the early 20th century by J.G.A. Lugol as a treatment for tuberculosis and is still considered an essential component of basic healthcare systems [44][45]. Lugol’s solution is used as an antiseptic, disinfectant, supplement, and laboratory reagent, among the most important applications [2][46]. Currently, many iodine-based products are being developed, and the global demand for iodine has increased in rthecen last decades. In 2017, the iodine market value was 833 million USD, and it is forecasted to be ~1.14 billion USD by 2024 [47]. Chile and Japan lead the global production of iodine (having also the biggest reserves worldwide), followed by Turkmenistan, Azerbaijan, Indonesia, and Russia (the US has been excluded from statistics in recent years) [48][49]. In the case of radioisotopes (used in nuclear medicine), ithey must be produced in nuclear reactors or cyclotrons from tellurium or xenon gases [50][51]. The major industrial applications of iodine include production of X-ray contrast media (XCM) (22%), pharmaceuticals (13%), polarization films (12%), animal feed (8%), iodophors (7%), fluorochemicals (7%), biocides (4%), nylon (4%), and human nutrition supplements (3%) [52]. The section below describes the relevant iodine applications of iodine in biomedicine and some of the representative iodine-based products.6. Applications in the Health Sciences
6.1. Disinfection, Asepsis, and Wound Care
Iodine has a broad spectrum against several microorganisms, including resistant forms (e.g., conidia, endospores, cysts, biofilms) [53][54][55]. Of all inorganic iodine species with catalytic activity, I2 is the most abundant and the leading antimicrobial agent in iodine-based disinfectants [26]. Other iodine species recognized as antimicrobials are HOI and H2OI+. However, they are restricted to extreme pH ranges, and the amount of I- [56][57]. Within solvents like alcohol, the solvated forms I2⋅H2O or I2⋅ROH are proposed as the anti-microbial species [58]. Lugol’s solution became popular as a disinfectant but had some drawbacks, such as staining of the skin and materials, local pain, and irritation. In addition, a proportion of I2 is lost by volatilization. These problems were solved in the early 1950s by the development of iodophors. The advantages of iodophoric preparations are reduced staining, increased I2 solubility, broad pH range (2.5–7.0), and slow release to prolong the antimicrobial action [59][60]. Iodophors are made with solubilizing agents such as natural or synthetic polymers or surfactants. They can be anionic, cationic, or nonionic [61][62]. Natural polymers are mostly starch and cellulose derivatives (e.g., amylose, amylopectin, Cadexomer, carboxymethyl cellulose, and methyl hydroxypropyl cellulose). Chitosan and lecithin are used in more complex iodophoric formulations (e.g., carboxymethyl chitosan and hydroxylated lecithin). Regarding synthetic polymers, PVP/I is the most used, followed by polyvinyl alcohol with iodine (PVAI). PVP/I is routinely used as a milk and teat disinfectant and is, in fact, an important contributor to the iodine content in dairy products [63]. Other excellent polymeric carriers include poly(4-vinyl pyridine), poly(3-vinyl-10-methylphenothiazine), poly(2-ethyl-2-oxazoline), and poly(tetramethylene ether) glycol [62][64]. Iodophors like PVP/I have shown biocidal effects on different species of bacteria (e.g., Escherichia coli, Staphylococcus aureus, Pseudomonas aeruginosa, and Chlamydia trachomatis), fungi (e.g., Candida spp. and Trichophyton spp.), protozoa (e.g., Trichomonas and Acanthamoeba spp.), and viruses (e.g., herpes simplex virus type I, adenovirus, influenza A viruses, rotavirus, poliovirus, and human immunodeficiency virus) [65][66][67][68][69][70][71][72][73]. Enveloped viruses are susceptible to iodine, and PVP-I’s efficacy (0.2–5%) was more recently proven in reducing viral loads of SARS-CoV-2 down to undetectable levels. Currently, skin, ophthalmic, nasal, and oral PVP-I-based antiseptic products are recommended to prevent transmissions during medical consultation [74][75][76]. Iodophors have also been exploited in novel wound healing and anti-inflammatory products because of their biocompatibility. PVAI and PVP/I-based hydrogels are good examples; they are constituted by flexible matrices that maintain asepsis and moisture. Moreover, they also absorb exudates, allow wound oxygenation, and have low toxicity and skin irritation [77][78]. Together with other components, hydrogels can serve as scaffolds for tissue regeneration, regulate medication released, or display unique properties to respond to stimuli, such as color change by temperature (thermochromism) or pH/thermal sensitivity [79][80]. It is important to mention that using iodine-based disinfectants in drinking water is not recommended because of the risk of undesirable byproducts. There are more than 600 peptides in water [81] reacting with chloramine (NH2Cl), H2OI+, and HIO to form highly toxic compounds of concern for people and the environment [82]. Reactions of HIO, I2, OI− species, and chloramines also affect pyridine nucleotides and glutathione (GSH), a potent and essential cellular antioxidant molecule. HIO (resulting from I2 and OH−) is a more selective downgrader of reduced dihydro-nicotinamide mononucleotide (NMNH) and nicotinamide adenine dinucleotide phosphate (NADH) than HOCl, and it can directly oxidize GSH or decrease its production by reducing the availability of NADPH (needed in GSH cycling) [83].6.2. Supplementation
When iodine ingestion is insufficient, there is a need to consume supplements to maintain normal thyroid function (euthyroidism). Iodine intake by groups of age is recommended as follows: 90 µg/day for infants and children 0–59 months, 120 µg/day for school children (6 to 12 years), 150 µg/day for adults, and 200 µg/day for pregnant and breastfeeding women [84]. Upper limits are much more difficult to establish because they are influenced by previous long-term iodine status [85] and even the kind of supplementation [86]. Some studies reported normal thyroid function at high doses of iodine from the diet (mainly from seaweed, 1.2 mg/day) [87], supplements (1–3 mg/day) [88], Lugol’s solution, and PVP-based water disinfectants (4–8 mg/L water) [89]. However, the recommended safe iodine intake for euthyroid people by the WHO is up to 1 mg/day, except for pregnant and lactating women that have no extra benefit receiving >500 µg/day and children of <2 years that should not exceed >180 µg/day [90]. The most common and suitable indicator to evaluate the iodine status in a population is urinary iodine, given that iodine is mostly excreted in urine (~90%). In this sense, the best method is urinary iodine excretion (UIE), which is determined from the whole urine collected for 24 h. Urinary iodine concentration (UIC) from one urine sample (preferably collected in the morning) is enough and more practical to define the general status according to WHO [2013]. For most people (including lactating women), >100 µg/L UIC is considered adequate, but <100 µg/L UIC reflects insufficient intake (<20 µg/L UIC suggests severe iodine deficiency), except for pregnant women whose optimal UIC is considered 150–249 µg/L, with <100 µg/L considered insufficient [91]. Nonetheless, urinary concentrations might vary in short periods (days–hours). Thus, to determine the iodine status and thyroid function of individuals, it is recommended to screen the levels of TSH and free T4 as a minimum [92][93]. Other parameters are evaluated to monitor thyroid function, such as goiter rate (%), levels of T3, rT3, TG, antibodies for TG (TgAb) or TPO (TPOAb), and thyroid-stimulating immunoglobulin (TSI) [88]. Optimal consumption of iodine can be obtained with an appropriate diet, consuming seafood (e.g., seaweed, fish, crabs, and oyster), dairy products (e.g., milk, yogurt, and cheese), tubers (e.g., turnip and saffron), beef kidney, green beans, eggs, yeast, some condiments (e.g., chili powder and mint), and iodized salt [94][95]. However, some geographical areas might have iodine-deficient water and soils; consequently, the iodine content in food is lower. For example, iodine content in plants can be up to 1 mg/kg or down to 10 μg/kg (dry weight), depending on the soil [92]. Geographic iodine-deficient areas include mountainous and inland regions of South America (e.g., the Andes and inland Brazil), the Midwestern United States, Europe (e.g., Alps, Pyrenees, England, Wales, Greece, and the Netherlands), Asia (China, India, Bangladesh, Himalayan hillsides, and Indonesia), Africa (e.g., Atlas Mountains, Nigeria, Cameroon, the Central African Republic Democratic Republic of Congo, Uganda, and Ethiopia), Southern Australia, and Highlands of New Guinea [96]. The additional intake of iodine from supplements is recommended to prevent IDD in iodine-deficient areas (especially among women of reproductive age). Currently, the best strategy to face IDD in the world has been the universal iodization of table salt (with KI, NaI, or KIO3), implemented in 1994 by the International Council for the Control of Iodine Deficiency Disorders (ICCIDD). The advantages of this product lie in the global consumption of salt, cheap cost production, long shelf-life, accessibility for remote communities, and imperceptible taste modification [4]. IDD persists even in developed countries due to the unequal consumption and distribution of iodized salt among low- and high-income households [97][98]. Moreover, it has been demonstrated that iodine can be partially or entirely lost during cooking depending on cookware materials and ingredients such as ascorbic acid, glucose, and some condiments, as well as because of impurities and storage conditions, mainly the kind of package and humidity [99][5]. In the market, there is a wide variety of supplements that can also be taken with one or more of the following components in their formulations: KI, NaI, KIO3, I2, iodized oil, natural products based on seaweed (from species Laminaria spp., Fucus vesiculosus, Alaria esculenta, Ascophyllum nodosum, Ecklonia maxima, Eisenia bicyclis, Hizikia fusiforme, Palmaria palmata, Porphyra tenera, Postelsia palmaeformis, and Sargassum sp.) or plants (e.g., Commiphora mukul and Iris versicolor) [94][100][101]. Among all supplements, natural formulations have the most variability or declare the highest iodine contents and should be avoided for pregnant women or those planning a pregnancy [101][102]. Natural or synthetic thyroid hormones are used not as supplements but under prescription to treat hypothyroidism. Currently, levothyroxine (or l-thyroxine) is the most recommended by endocrine societies (and produced worldwide) for thyroid hormone replacement therapy [103]. Probiotic consumption might improve iodine status, given that the gut microbiome participates in nutrient absorption and cycling of THs. Autoimmune thyroid dysfunctions and thyroid carcinoma are linked to dysbiosis (imbalance in the microbiota). Hypothyroidism and hyperthyroidism are correlated with the reduction in intestinal bacteria from Lactobacillaceae and Bifidobacteriaceae families [104]. Vitamin D and other nutrients such as iron, copper, selenium, and zinc are often altered in thyroid disorders. They can be considered in supplementation and the avoidance of goitrogens [96][104]. Goitrogens decrease iodine absorption, primarily by inhibiting cellular iodine transporters, interfering with TH synthesis, or reducing the conversion of T3 from T4 [96][105][106]. They comprise cyanide (from smoking), nitrates, fluoride, some contaminants (e.g., perchlorate and disulfides), foods rich in glucosides (e.g., cassava, lima beans, linseed, sorghum, and sweet potato), glucosinolates (e.g., broccoli, kale, cauliflower, cabbage, and turnips), and flavonoids (e.g., onions, lettuce, tomatoes, and grapes). Even nutrient deficiencies of iron, selenium, and vitamin A are considered goitrogens [106][107].6.3. Contrast Agents
X-rays allow us to see structures of high density because the X-ray absorption coefficient (µ) is directly proportional to the atomic mass of the compound. Bones and some organs in the body can be directly distinguished by X-ray, but other less dense structures need contrast agents to visualize them [108]. X-ray contrast media (XCM) are substances that allow visualization of those biological structures, and, depending on the difference in µ, they can be classified as positive or negative. Negative XCM are gases of lower absorption coefficient (e.g., O2 and CO2), and positive XCM contain elements of high atomic number, such as iodine or barium, that stand out in X-ray imaging [108][109]. Positive XCM can be classified as targeted (or specific) and extracellular (or unspecific), depending on whether the contrasting reagent is metabolized in the body [108][110]. Extracellular XCM are water-soluble agents mainly used to visualize the circulatory system. The pharmacokinetics is very similar among extracellular XCM, taking 3–10 min for distribution and typically 1–2 h in elimination (via glomerular filtration). Under renal impairment, the excretion takes up to 10 h with a higher risk of nephrotoxicity [108][110]. On the contrary, targeted XCM (alsor biliary contrast agents) have good lipophilicity and different distribution and elimination times. The disadvantages of XCM with low hydrophilicity are less tolerability, hepatic or renal toxicity, and higher allergic reactions [108][111]. For those reasons, research on targeted XCM is now developing into noniodine compounds, although promising advances have been accomplished with liposomes and polymers as carriers [111]. The simplest contrast agent is NaI, the first iodinated XCM in the market (in 1918), with an excellent µ value but not as good tolerability at high doses. Currently, most XCM are based on molecules of one or more triiodobenzene rings. Triiodobenzene derivatives are the extracellular XCM of choice because of their stability, tolerability, low toxicity, and wide range of compounds that can be produced. The synthesis is achieved by substituting the hydrogens at positions 1, 3, and 5 of the benzene ring with I atoms. Some good examples are iohexol, iopamidol, ioversol, ioxilan, iopromide, ioxaglic acid, iotrolan, iodixanol, and diatrizoate meglumine [112]. Examples of approved targeted agents are iodipamide meglumine to visualize the bile duct and the gallbladder and lipiodol for imaging hepatocellular carcinoma [113][114][115].6.4. Applications in Nuclear Medicine
All kinds of radiation can be dangerous for life, but the extent of damage depends on the decay mode and half-life of the radioactive atom. Alpha (α) and beta (β) radiation are weaker but significantly dangerous when particles are inhaled, swallowed, or absorbed in the body. Gamma (γ) and X-rays are much more powerful and penetrating, causing immediate severe cellular damage from external sources [116]. In a controlled fashion, nuclear medicine takes advantage of radioisotopes that can be detected in small amounts and represent a lesser danger to lifefor life, to diagnose and treat several diseases. Diagnostics in nuclear medicine differ from radiology in the studying of the functionality of tissues and organs, not only examining anatomic structures. For this purpose, contrast reagentradiopharmaceuticals are injected (most of the time), inhaled, or orally administered to follow their circulation, accumulation, or metabolization in the body [108][117]. For imaging, developed technologies are scintigraphy, single-photon emission computed tomography (SPECT), positron emission tomography (PET), or combinations with computed tomography (CT) such as SPECT/CT and PET/CT [117][118][119]. Radiotherapy also uses radioisotopes to target specific abnormal cells or tissues and destroy them via internal radiation (e.g., hyperthyroidism caused by Graves’ disease toxic nodular goiter) [120]. The most used radioisotope for both diagnostics and therapy is technetium (99Tc), followed by iodine, because of their high intensity and short half-life [117][120]. The main iodine radioisotopes of iodine exploited in medicine and for research are 123I, 124I, 125I, and 131I [121]; their physicochemical properties are described in Table 1.| Isotope | Abundance | Atomic Mass | Half-Life | Decay Mode (%) | keV | Production | Application | |||
|---|---|---|---|---|---|---|---|---|---|---|
| 123 | I | Synthetic | 122.9056 | 13.2232 h | β | + | (100%) | 159 | Cyclotron | Diagnosis (SPECT) and therapy |
| 124 | I | Synthetic | 123.9062 | 4.176 d | β | + | (100%) | 603 | Cyclotron | Research and diagnosis (PET) |
| 125 | I | Synthetic | 124.9046 | 59.392 d | ε (100%) | 27.5 | Nuclear reactor and cyclotron | Therapy and radioimmunoassay | ||
| 127 | I | Natural (1) | 126.9045 | Stable | Natural | Diagnosis (X-rays and CT) and therapy | ||||
| 131 | I | Synthetic | 130.9061 | 8.0249 d | β | − | (100) | 364.5 | Nuclear reactor | Diagnosis, therapy, and RIA |
6.5. Prophylaxis
Radioactive contamination after a nuclear explosion or an accident can bring severe consequences for people and the environment in the short and long term, as occurred with the atomic bombings of Hiroshima and Nagasaki in 1945 or the Chernobyl (former Soviet Union) and Fukushima (Japan) nuclear accidents in 1986 and 2011, respectively. Beyond the immediate damage of radiation, iodine radioisotopes are of particular concern because of their accumulation in the body and potential incorporation into the food chain following regular iodine cycling [131][132][133]. High radiation levels can induce hypothyroidism or acute thyroiditis. Lower exposure to radiation increases the risk of thyroid cancer and benign thyroid nodules in the long term, especially in infants, children, and adolescents [134]. HTo prevent the absorption of radioactive isotopes (prophylaxis), high doses of stable iodine (127I) can be promptly distributed in the population to prevent the absorption of radioactive isotopes (prophylaxis) [88]. Prophylaxis is not used to restore iodine status; instead, it takes advantage of the Wolff–Chaikoff effect, a transient inhibition of TH production induced by excess iodine. In most cases, the thyroid function is restored in 1–2 weeks. However,but vulnerable groups (e.g., fetuses, neonates, and patients with autoimmune thyroiditis and Graves'’ disease or treated with antithyroid drugs) may not "“escape"” from this effect [135]. Prophylaxis is recommended when exposure to vulnerable groups (neonates, infants, and children) is ≥10 mGy (1 Gy is equal to 1 J of radiation absorbed per kg) [136]. Older adults (>40 years) have a minimal thyroid cancer risk and more side-effects with excessive iodine supplementation; therefore, prophylaxis is recommended at ≥100 mGy. According to WHO, a single dose of I2, KI, or KIO3 is sufficient for all age groupsgroups of age, as indicated in Table 2. Repetition doses are only prescribed for pregnant women from iodine-deficient areas and vulnerable people with prolonged exposure (for example, infants inhaling radioactive material) [136].| Age Group | I | 2 | (mg) |
KI (mg) |
KIO | 3 | (mg) | Fraction of a Tablet (100 mg) |
|---|---|---|---|---|---|---|---|---|
| Adults and adolescents, including lactating women (>12 years) | 100 | 130 | 170 | 1 | ||||
| Children (3–12 years) | 50 | 65 | 85 | 1/2 | ||||
| Infants (1 month–3 years) | 25 | 32 | 42 | 1/4 | ||||
| Neonates (birth–1 month) | 12.5 | 16 | 21 | 1/8 |
References
- Venturi, S.; Donati, F.M.; Venturi, A.; Venturi, M. Environmental Iodine Deficiency: A Challenge to the Evolution of Terrestrial Life? Thyroid 2000, 10, 727–729.
- Gottardi, W. Iodine as Disinfectant. In Iodine Chemistry and Applications; Kaiho, T., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; Volume 9781118466, pp. 375–410.
- Crockford, S.J. Evolutionary Roots of Iodine and Thyroid Hormones in Cellcell Signaling. Integr. Comp. Biol. 2009, 49, 155–166.
- Venkatesh Mannar, M.G.; Dunn, J.T.; World Health Organization. Salt Iodization for the Elimination of Iodine Deficiency; International Council for Control of Iodine Deficiency Disorders: Brussels; Belgium, 1995.
- Diosady, L.L.; Alberti, J.O.; Mannar, M.G.V.; FitzGerald, S. Stability of Iodine in Iodized Salt Used for Correction of Iodine-Deficiency Disorders. II. Food Nutr. Bull. 1998, 19, 240–250.
- Aceves, C.; Mendieta, I.; Anguiano, B.; Delgado-González, E. Molecular Iodine Has Extrathyroidal Effects as an Antioxidant, Differentiator, and Immunomodulator. Int. J. Mol. Sci. 2021, 22, 1228.
- World Health Organization. Protection of the Human Environment. Guidelines for Iodine Prophylaxis Following Nuclear Accidents; Update 1999; World Health Organization: Geneva, Switzerland, 1999; pp. 1–45.
- Küpper, F.C.; Feiters, M.C.; Olofsson, B.; Kaiho, T.; Yanagida, S.; Zimmermann, M.B.; Carpenter, L.J.; Luther, G.W.; Lu, Z.; Jonsson, M.; et al. Commemorating Two Centuries of Iodine Research: An Interdisciplinary Overview of Current Research. Angew. Chemie Int. Ed. 2011, 50, 11598–11620.
- National Center for Biotechnology Information PubChem Element Summary for AtomicNumber 53, Iodine. Available online: https://pubchem.ncbi.nlm.nih.gov/element/Iodine (accessed on 24 April 2022).
- Meija, J.; Coplen, T.B.; Berglund, M.; Brand, W.A.; De Bièvre, P.; Gröning, M.; Holden, N.E.; Irrgeher, J.; Loss, R.D.; Walczyk, T.; et al. Isotopic Compositions of the Elements 2013 (IUPAC Technical Report). Pure Appl. Chem. 2016, 88, 293–306.
- Edwards, R.R. Iodine-129: Its Occurrence in Nature and Its Utility as a Tracer. Science 1962, 137, 851–853.
- Kaiho, T. Inorganic Iodides. In Iodine Chemistry and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; Volume 9781118466, pp. 55–73.
- Muramatsu, Y.; Yoshida, S.; Fehn, U.; Amachi, S.; Ohmomo, Y. Studies with Natural and Anthropogenic Iodine Isotopes: Iodine Distribution and Cycling in the Global Environment. J. Environ. Radioact. 2004, 74, 221–232.
- Moreda-Piñeiro, A.; Romarís-Hortas, V.; Bermejo-Barrera, P. A Review on Iodine Speciation for Environmental, Biological and Nutrition Fields. J. Anal. At. Spectrom. 2011, 26, 2107.
- Amachi, S. Microbial Contribution to Global Iodine Cycling: Volatilization, Accumulation, Reduction, Oxidation, and Sorption of Iodine. Microbes Environ. 2008, 23, 269–276.
- Kocher, D.C. A Dynamic Model of the Global Iodine Cycle and Estimation of Dose to the World Population from Releases of Iodine-129 to the Environment. Environ. Int. 1981, 5, 15–31.
- Elmore, D.; Gove, H.E.; Ferraro, R.; Kilius, L.R.; Lee, H.W.; Chang, K.H.; Beukens, R.P.; Litherland, A.E.; Russo, C.J.; Purser, K.H.; et al. Determination of 129I Using Tandem Accelerator Mass Spectrometry. Nature 1980, 286, 138–140.
- Brown, C.F.; Geiszler, K.N.; Lindberg, M.J. Analysis of 129I in Groundwater Samples: Direct and Quantitative Results below the Drinking Water Standard. Appl. Geochemistry 2007, 22, 648–655.
- Crivello, J.V. Diaryliodonium Salt Photoacid Generators. In Iodine Chemistry and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 457–478.
- Carpenter, L.J. Atmospheric Chemistry of Iodine. In Iodine Chemistry and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 591–601.
- Cox, R.A.; Bloss, W.J.; Jones, R.L.; Rowley, D.M. OIO and the Atmospheric Cycle of Iodine. Geophys. Res. Lett. 1999, 26, 1857–1860.
- Chameides, W.L.; Davis, D.D. Iodine: Its Possible Role in Tropospheric Photochemistry. J. Geophys. Res. Ocean. 1980, 85, 7383–7398.
- Raso, A.R.W.; Custard, K.D.; May, N.W.; Tanner, D.; Newburn, M.K.; Walker, L.; Moore, R.J.; Huey, L.G.; Alexander, L.; Shepson, P.B.; et al. Active Molecular Iodine Photochemistry in the Arctic. Proc. Natl. Acad. Sci. USA 2017, 114, 10053–10058.
- Yuita, K. Dynamics of Iodine, Bromine, and Chlorine in Soil: II. Chemical Forms of Iodine in Soil Solutions. Soil Sci. Plant Nutr. 1992, 38, 281–287.
- Li, J.; Wang, Y.; Guo, W.; Xie, X.; Zhang, L. Factors Controlling Spatial Variation of Iodine Species in Groundwater of the Datong Basin, Northern China. Procedia Earth Planet. Sci. 2013, 7, 483–486.
- Gottardi, W. Iodine and Disinfection: Theoretical Study on Mode of Action, Efficiency, Stability, and Analytical Aspects in the Aqueous System. Arch. Pharm. 1999, 332, 151–157.
- Gottardi, W. Potentiometrische Bestimmung Der Gleichgewichtskonzentrationen an Freiem Und Komplex Gebundenem Iod in W~iflrigen Liisungen von Polyvinylpyrrolidon-Iod (PVP-Iod) Polyvinylpyrrolidon-Iod (PVP-Iod). Fresenius’ Zeitschrift für Anal. Chemie 1983, 314, 582–585.
- Hulbert, A.J. Thyroid Hormones and Their Effects: A New Perspective. Biol. Rev. 2000, 75, 519–631.
- Köhrle, J. Thyroid Hormones and Derivatives: Endogenous Thyroid Hormones and Their Targets. In Thyroid Hormone Nuclear Receptor; Springer: Berlin, Germany, 2018; Volume 1897, pp. 85–104.
- Citterio, C.E.; Targovnik, H.M.; Arvan, P. The Role of Thyroglobulin in Thyroid Hormonogenesis. Nat. Rev. Endocrinol. 2019, 15, 323–338.
- Dedieu, A.; Gaillard, J.-C.; Pourcher, T.; Darrouzet, E.; Armengaud, J. Revisiting Iodination Sites in Thyroglobulin with an Organ-Oriented Shotgun Strategy. J. Biol. Chem. 2011, 286, 259–269.
- Fong, P. Thyroid Iodide Efflux: A Team Effort? J. Physiol. 2011, 589, 5929–5939.
- Vermot, A.; Petit-Härtlein, I.; Smith, S.M.E.; Fieschi, F. NADPH Oxidases (NOX): An Overview from Discovery, Molecular Mechanisms to Physiology and Pathology. Antioxidants 2021, 10, 890.
- Milanesi, A.; Brent, G.A. Iodine and Thyroid Hormone Synthesis, Metabolism, and Action. In Molecular, Genetic, and Nutritional Aspects of Major and Trace Minerals; Elsevier: Amsterdam, The Netherlands, 2017; Volume 1896, pp. 143–150.
- Nicoloff, J.T.; Low, J.C.; Dussault, J.H.; Fisher, D.A. Simultaneous Measurement of Thyroxine and Triiodothyronine Peripheral Turnover Kinetics in Man. J. Clin. Invest. 1972, 51, 473–483.
- Gomes-Lima, C.; Burman, K.D. Reverse T 3 or Perverse T 3? Still Puzzling after 40 Years. Cleve. Clin. J. Med. 2018, 85, 450–455.
- Pereira, A.; Braekman, J.C.; Dumont, J.E.; Boeynaems, J.M. Identification of a Major Iodolipid from the Horse Thyroid Gland as 2-Iodohexadecanal. J. Biol. Chem. 1990, 265, 17018–17025.
- Aceves, C.; Anguiano, B.; Delgado, G. Is Iodine a Gatekeeper of the Integrity of the Mammary Gland? J. Mammary Gland Biol. Neoplasia 2005, 10, 189–196.
- Dembitsky, V.M. Biogenic Iodine and Iodine-Containing Metabolites. Nat. Prod. Commun. 2006, 1, 1934578X0600100.
- Wang, X.; Yan, F.; Wang, Q. Molecular Iodine: Catalysis in Heterocyclic Synthesis. Synth. Commun. 2021, 51, 1763–1781.
- Bürgi, H.; Schaffner, T.; Seiler, J.P. The Toxicology of Iodate: A Review of the Literature. Thyroid 2001, 11, 449–456.
- Tekale, S.U.; Kauthale, S.S.; Dake, S.A.; Sarda, S.R.; Pawar, R.P. Molecular Iodine: An Efficient and Versatile Reagent for Organic Synthesis. Curr. Org. Chem. 2012, 16, 1485–1501.
- Dohi, T.; Kita, Y. Oxidizing Agents. In Iodine Chemistry and Applications; Kaiho, T., Ed.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 277–301.
- World Health Organization. WHO Model List of Essential Medicines—22nd List; World Health Organization: Geneva, Switzerland, 2021; p. 66.
- Lugol, J.G.A. Mémoire Sur l’Emploi de l’Iode Dans Les Maladies Scrofuleuses. Glasgow Med. J. 1832, 5, 83–92.
- Cooper, R.A. Iodine Revisited. Int. Wound J. 2007, 4, 124–137.
- Fernández, L. Global Market Value of Iodine 2017 & 2024. Available online: https://www.statista.com/statistics/1001959/market-value-iodine-worldwide/ (accessed on 2 March 2022).
- Garside, M. Iodine Global Reserves by Countries 2020. Available online: https://www.statista.com/statistics/264946/global-iodine-reserves-by-countries/ (accessed on 2 March 2022).
- Garside, M. Major Countries in Iodine Production 2010–2020. Available online: https://www.statista.com/statistics/264945/major-countries-in-iodine-production/ (accessed on 2 March 2022).
- Rayyes, A.; Hamid, A. Technical Meeting of Project Counterparts on Cyclotron Production of I-123. In Proceedings of the Cyclotron production of Iodine-123, Sao Paulo, Brazil, 8–10 August 2001; International Atomic Energy Agency: Vienna, Brazil, 2002; pp. 81–89.
- Chattopadhyay, S.; Saha Das, S. Recovery of 131I from Alkaline Solution of N-Irradiated Tellurium Target Using a Tiny Dowex-1 Column. Appl. Radiat. Isot. 2010, 68, 1967–1969.
- Statista Research Department Global Demand for Iodine by Application 2016. Available online: https://www.statista.com/statistics/862097/global-iodine-demand-share-by-application/ (accessed on 2 March 2022).
- Sharma, A.; Stan, M.N. Thyrotoxicosis: Diagnosis and Management. Mayo Clin. Proc. 2019, 94, 1048–1064.
- Horn-Ross, P.L.; Morris, J.S.; Lee, M.; West, D.W.; Whittemore, A.S.; McDougall, I.R.; Nowels, K.; Stewart, S.L.; Spate, V.L.; Shiau, A.C.; et al. Iodine and Thyroid Cancer Risk among Women in a Multiethnic Population: The Bay Area Thyroid Cancer Study. Cancer Epidemiol Biomarkers Prev. 2001, 10, 979–985.
- Zimmermann, M.B.; Galetti, V. Iodine Intake as a Risk Factor for Thyroid Cancer: A Comprehensive Review of Animal and Human Studies. Thyroid Res. 2015, 8, 8.
- Rackur, H. New Aspects of Mechanism of Action of Povidone-Iodine. J. Hosp. Infect. 1985, 6, 13–23.
- Bafort, F.; Parisi, O.; Perraudin, J.-P.; Jijakli, M.H. Mode of Action of Lactoperoxidase as Related to Its Antimicrobial Activity: A Review. Enzyme Res. 2014, 2014, 517164.
- Ren, B.; Zhu, Y. A New Perspective on Thyroid Hormones: Crosstalk with Reproductive Hormones in Females. Int. J. Mol. Sci. 2022, 23, 2708.
- Gottardi, W. Potentiometrische Bestimmung Der Gleichgewichtskonzentrationen an Freiem Und Komplex Gebundenem Iod in W~iflrigen Liisungen von Polyvinylpyrrolidon-Iod (PVP-Iod) Polyvinylpyrrolidon-Iod (PVP-Iod). Fresenius’ Zeitschrift für Anal. Chemie 1983, 314, 582–585.
- Reddy, J.M.; Knox, K.; Robin, M.B. Crystal Structure of HI 3 ·2C 6 H 5 CONH 2: A Model of the Starch—Iodine Complex. J. Chem. Phys. 1964, 40, 1082–1089.
- Gottardi, W. Iodine and Disinfection: Theoretical Study on Mode of Action, Efficiency, Stability, and Analytical Aspects in the Aqueous System. Arch. Pharm. 1999, 332, 151–157.
- Makhayeva, D.N.; Irmukhametova, G.S.; Khutoryanskiy, V.V. Polymeric Iodophors: Preparation, Properties, and Biomedical Applications. Rev. J. Chem. 2020, 10, 40–57.
- French, E.A.; Mukai, M.; Zurakowski, M.; Rauch, B.; Gioia, G.; Hillebrandt, J.R.; Henderson, M.; Schukken, Y.H.; Hemling, T.C. Iodide Residues in Milk Vary between Iodine-Based Teat Disinfectants. J. Food Sci. 2016, 81, T1864–T1870.
- Sukawa, H.; Yoda, Y.; Sugimoto, H.; Yoshida, S.; Yamamoto, T.; Kuroda, S.; Sanechika, K.; Nishinuma, M. Absorption of Iodine by Polymers and Electrochemical Response of Polymer Film in Aqueous Solution of Iodine. Polym. J. 1989, 21, 403–408.
- Schreier, H.; Erdos, G.; Reimer, K.; König, B.; König, W.; Fleischer, W. Molecular Effects of Povidone-Iodine on Relevant Microorganisms: An Electron-Microscopic and Biochemical Study. Dermatology 1997, 195, 111–116.
- Berkelman, R.L.; Holland, B.W.; Anderson, R.L. Increased Bactericidal Activity of Dilute Preparations of Povidone-Iodine Solutions. J. Clin. Microbiol. 1982, 15, 635–639.
- Rösner, H.; Möller, W.; Groebner, S.; Torremante, P. Antiproliferative/Cytotoxic Effects of Molecular Iodine, Povidone-Iodine and Lugol’s Solution in Different Human Carcinoma Cell Lines. Oncol. Lett. 2016, 12, 2159–2162.
- Piérard, G.E.; Piérard-Franchimont, C.; Arrese, J.E. Povidone-Iodine Wash Solutions in the Prevention of Superficial Fungal Infections; Predictive Evaluation Using the Corneofungimetry Bioassay. Eur. J. Clin. Pharmacol. 1997, 53, 101–104.
- Yu, H.; Tak-Yin, M. The Efficacy of Povidone-Iodine Pessaries in a Short, Low-Dose Treatment Regime on Candidal, Trichomonal and Non-Specific Vaginitis. Postgrad. Med. J. 1993, 69 (Suppl. S3), S58–S61.
- Gatti, S.; Cevini, C.; Bruno, A.; Penso, G.; Rama, P.; Scaglia, M. In Vitro Effectiveness of Povidone-Iodine on Acanthamoeba Isolates from Human Cornea. Antimicrob. Agents Chemother. 1998, 42, 2232–2234.
- Kawana, R.; Kitamura, T.; Nakagomi, O.; Matsumoto, I.; Arita, M.; Yoshihara, N.; Yanagi, K.; Yamada, A.; Morita, O.; Yoshida, Y.; et al. Inactivation of Human Viruses by Povidone-Iodine in Comparison with Other Antiseptics. Dermatology 1997, 195, 29–35.
- Asanaka, M. In Vitro Study on Inactivation of Various Viruses Including Human Immunodeficiency Virus (HIV) by PVP-I. Proc. First Asian/Pacific Congr. Antisepsis. 1988. Available online: https://cir.nii.ac.jp/crid/1570009750369814784?lang=en (accessed on 15 March 2022).
- Sriwilaijaroen, N.; Wilairat, P.; Hiramatsu, H.; Takahashi, T.; Suzuki, T.; Ito, M.; Ito, Y.; Tashiro, M.; Suzuki, Y. Mechanisms of the Action of Povidone-Iodine against Human and Avian Influenza A Viruses: Its Effects on Hemagglutination and Sialidase Activities. Virol. J. 2009, 6, 124.
- Anderson, D.E.; Sivalingam, V.; Kang, A.E.Z.; Ananthanarayanan, A.; Arumugam, H.; Jenkins, T.M.; Hadjiat, Y.; Eggers, M. Povidone-Iodine Demonstrates Rapid In Vitro Virucidal Activity Against SARS-CoV-2, The Virus Causing COVID-19 Disease. Infect. Dis. Ther. 2020, 9, 669–675.
- Liang, B.; Yuan, X.; Wei, G.; Wang, W.; Zhang, M.; Peng, H.; Javer, A.; Mendenhall, M.; Julander, J.; Huang, S.; et al. In-Vivo Toxicity Studies and In-Vitro Inactivation of SARS-CoV-2 by Povidone-Iodine In-Situ Gel Forming Formulations. bioRxiv 2020. bioRxiv:2020.05.18.103184.
- Garcia-Sanchez, A.; Peña-Cardelles, J.F.; Ruiz, S.; Robles, F.; Ordonez-Fernandez, E.; Salgado-Peralvo, A.O.; Balloch, J.; Simon, J.C. Efficacy of Pre-Procedural Mouthwashes against SARS-CoV-2: A Systematic Review of Randomized Controlled Trials. J. Clin. Med. 2022, 11, 1692.
- Hoekstra, M.J.; Westgate, S.J.; Mueller, S. Povidone-Iodine Ointment Demonstrates in Vitro Efficacy against Biofilm Formation. Int. Wound J. 2017, 14, 172–179.
- Muppalaneni, S.; Omidian, H. Polyvinyl Alcohol in Medicine and Pharmacy: A Perspective. J. Dev. Drugs 2013, 2, 1–5.
- Miao, Z.; Sun, Y.; Tao, Z.; Chen, Y.; Ma, Y.; Zhu, D.; Huang, X.; Zha, Z. Thermochromic Polyvinyl Alcohol-Iodine Hydrogels with Safe Threshold Temperature for Infectious Wound Healing. Adv. Healthc. Mater. 2021, 10, 2100722.
- Montaser, A.S.; Rehan, M.; El-Naggar, M.E. PH-Thermosensitive Hydrogel Based on Polyvinyl Alcohol/Sodium Alginate/N-Isopropyl Acrylamide Composite for Treating Re-Infected Wounds. Int. J. Biol. Macromol. 2019, 124, 1016–1024.
- Tang, Y.; Xu, Y.; Li, F.; Jmaiff, L.; Hrudey, S.E.; Li, X.-F. Nontargeted Identification of Peptides and Disinfection Byproducts in Water. J. Environ. Sci. 2016, 42, 259–266.
- Gao, Y.; Qiu, J.; Ji, Y.; Wawryk, N.J.P.; An, T.; Li, X.-F. Formation Mechanism of Iodinated Aromatic Disinfection Byproducts: Acid Catalysis with H2OI+. Environ. Sci. Technol. 2022, 56, 1791–1800.
- Prütz, W.A.; Kissner, R.; Koppenol, W.H.; Rüegger, H. On the Irreversible Destruction of Reduced Nicotinamide Nucleotides by Hypohalous Acids. Arch. Biochem. Biophys. 2000, 380, 181–191.
- World Health Organization/United Nations Children’s Fund (UNICEF)/International Council for Control of Iodine Deficiency Disorders. Review of Findings from 7-Country Study in Africa on Levels of Salt Idodization in Relation to Iodine Deficiency Disorders, Including Iodine-Induced Hyperthyroidism; WHO, UNICEF, ICCIDD: Geneva, Switzerland, 1996.
- Sharma, A.; Stan, M.N. Thyrotoxicosis: Diagnosis and Management. Mayo Clin. Proc. 2019, 94, 1048–1064.
- Aceves, C.; Mendieta, I.; Anguiano, B.; Delgado-González, E. Molecular Iodine Has Extrathyroidal Effects as an Antioxidant, Differentiator, and Immunomodulator. Int. J. Mol. Sci. 2021, 22, 1228.
- Nagataki, S. The Average of Dietary Iodine Intake Due to the Ingestion of Seaweeds Is 1.2 Mg/Day in Japan. Thyroid 2008, 18, 667–668.
- Farebrother, J.; Zimmermann, M.B.; Andersson, M. Excess Iodine Intake: Sources, Assessment, and Effects on Thyroid Function. Ann. N. Y. Acad. Sci. 2019, 1446, 44–65.
- Backer, H.; Hollowell, J. Use of Iodine for Water Disinfection: Iodine Toxicity and Maximum Recommended Dose. Environ. Health Perspect. 2000, 108, 679–684.
- World Health Organization. Vitamin and Mineral Requirements in Human Nutrition, 2nd ed; World Health Organization: Geneva, Switzerland, 2005.
- World Health Organization. Urinary Iodine Concentrations for Determining Iodine Status in Populations; World Health Organization: Geneva, Switzerland, 2013.
- Zimmermann, M.B.; Jooste, P.L.; Pandav, C.S. Iodine-Deficiency Disorders. Lancet 2008, 372, 1251–1262.
- Ristic-Medic, D.; Piskackova, Z.; Hooper, L.; Ruprich, J.; Casgrain, A.; Ashton, K.; Pavlovic, M.; Glibetic, M. Methods of Assessment of Iodine Status in Humans: A Systematic Review. Am. J. Clin. Nutr. 2009, 89, 2052S–2069S.
- Zicker, S.; Schoenherr, B. Focus on Nutrition: The Role of Iodine in Nutrition and Metabolism. Compend. Contin. Educ. Vet. 2012, 34, E1-4.
- Milagres, R.C.; de Souza, E.C.G.; Peluzio, M.; Franceschini, S.; Duarte, M.S.L. Food Iodine Content Table Compiled from International Databases. Rev. Nutr. 2020, 33, 1–12.
- Rohner, F.; Zimmermann, M.; Jooste, P.; Pandav, C.; Caldwell, K.; Raghavan, R.; Raiten, D.J. Biomarkers of Nutrition for Development—Iodine Review. J. Nutr. 2014, 144, 1322S–1342S.
- World Health Organization Guideline. In Fortification of Food-Grade Salt with Iodine for the Prevention and Control of Iodine Deficiency Disorders; World Health Organization: Geneva, Switzerland, 2014.
- UNICEF Worldwide, 89 per Cent of People Consume Iodized Salt. Available online: https://data.unicef.org/topic/nutrition/iodine/ (accessed on 15 March 2022).
- Chavasit, V.; Malaivongse, P.; Judprasong, K. Study on Stability of Iodine in Iodated Salt by Use of Different Cooking Model Conditions. J. Food Compos. Anal. 2002, 15, 265–276.
- Stansbury, J.; Saunders, P.; Winston, D. Promoting Healthy Thyroid Function with Iodine, Bladderwrack, Guggul and Iris. J. Restor. Med. 2012, 1, 83–90.
- Zimmermann, M.; Delange, F. Iodine Supplementation of Pregnant Women in Europe: A Review and Recommendations. Eur. J. Clin. Nutr. 2004, 58, 979–984.
- Leung, A.M.; Pearce, E.N.; Braverman, L.E. Iodine Content of Prenatal Multivitamins in the United States. N. Engl. J. Med. 2009, 360, 939–940.
- Hennessey, J.V. The Emergence of Levothyroxine as a Treatment for Hypothyroidism. Endocr. 2016 551 2016, 55, 6–18.
- Knezevic, J.; Starchl, C.; Tmava Berisha, A.; Amrein, K. Thyroid-Gut-Axis: How Does the Microbiota Influence Thyroid Function? Nutrients 2020, 12, 1769.
- Agrawal, V.; Ghaznavi, S.A.; Paschke, R. Environmental Goitrogens. In Encyclopedia of Endocrine Diseases; Elsevier: Amsterdam, The Netherlands, 2018; pp. 506–511.
- López-Moreno, M.; Garcés-Rimón, M.; Miguel, M. Antinutrients: Lectins, Goitrogens, Phytates and Oxalates, Friends or Foe? J. Funct. Foods 2022, 89.
- Gaitan, E. 9 Goitrogens. Baillieres. Clin. Endocrinol. Metab. 1988, 2, 683–702.
- Speck, U. X-ray Contrast Media: Overview, Use and Pharmaceutical Aspects; Springer: Berlin/Heidelberg, Germany, 2018.
- Bourin, M.; Jolliet, P.; Ballereau, F. An Overview of the Clinical Pharmacokinetics of X-ray Contrast Media. Clin. Pharmacokinet. 1997, 32, 180–193.
- Crivello, J.V. Diaryliodonium Salt Photoacid Generators. In Iodine Chemistry and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 457–478.
- Krause, W. Iodinated X-ray Contrast Agents. In Iodine Chemistry and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; Volume 9781118466, pp. 353–374.
- Zhibin, Y. FDA Approved Radiopharmaceuticals. Foreign Med. Sci. Sect. Radiat. Med. Nucl. Med. 2000, 24, 161–163.
- Bartolozzi, C.; Lencioni, R.; Caramella, D.; Palla, A.; Bassi, A.M.; Di Candio, G. Small Hepatocellular Carcinoma. Acta Radiol. 1996, 37, 69–74.
- Wallers, K.J.; McDermott, P.; James, W.B. Intravenous Cholangiography by Bolus Injection of Meglumine Iotroxamate and Meglumine Iodoxamate: A Comparative Trial of Two New Contrast Media. Clin. Radiol. 1981, 32, 457–459.
- Miszczuk, M.A.; Chapiro, J.; Geschwind, J.-F.H.; Thakur, V.; Nezami, N.; Laage-Gaupp, F.; Kulon, M.; van Breugel, J.M.M.; Fereydooni, A.; Lin, M.; et al. Lipiodol as an Imaging Biomarker of Tumor Response After Conventional Transarterial Chemoembolization: Prospective Clinical Validation in Patients with Primary and Secondary Liver Cancer. Transl. Oncol. 2020, 13, 100742.
- Karmaker, N.; Maraz, K.M.; Islam, F.; Haque, M.M.; Razzak, M.; Mollah, M.Z.I.; Faruque, M.R.I.; Ruhul, A. Khan Fundamental Characteristics and Application of Radiation. GSC Adv. Res. Rev. 2021, 7, 064–072.
- Shirakami, Y. Radioactive Iodine. In Iodine Chemistry and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; Volume 9781118466, pp. 603–624.
- Zerdoud, S.; Giraudet, A.-L.; Leboulleux, S.; Leenhardt, L.; Bardet, S.; Clerc, J.; Toubert, M.-E.; Al Ghuzlan, A.; Lamy, P.-J.; Bournaud, C.; et al. Radioactive Iodine Therapy, Molecular Imaging and Serum Biomarkers for Differentiated Thyroid Cancer: 2017 Guidelines of the French Societies of Nuclear Medicine, Endocrinology, Pathology, Biology, Endocrine Surgery and Head and Neck Surgery. Ann. Endocrinol. 2017, 78, 162–175.
- Braghirolli, A.M.S.; Waissmann, W.; Da Silva, J.B.; Dos Santos, G.R. Production of Iodine-124 and Its Applications in Nuclear Medicine. Appl. Radiat. Isot. 2014, 90, 138–148.
- Piel, M.; Rösch, F. Radiopharmaceutical Chemistry; Springer: Berlin/Heidelberg, Germany, 2012; Volume 71.
- Crișan, G.; Moldovean-Cioroianu, N.S.; Timaru, D.-G.; Andrieș, G.; Căinap, C.; Chiș, V. Radiopharmaceuticals for PET and SPECT Imaging: A Literature Review over the Last Decade. Int. J. Mol. Sci. 2022, 23, 5023.
- Kondev, F.G.; Wang, M.; Huang, W.J.; Naimi, S.; Audi, G. The NUBASE2020 Evaluation of Nuclear Physics Properties. Chinese Phys. C 2021, 45, 030001.
- Rasmussen, T.; de Nijs, R.; Olsen, L.K.; Kamper, A.L.; Bang, L.E.; Frimodt-Møller, M.; Kelbæk, H.; Sørensen, S.S.; Kjær, A.; Feldt-Rasmussen, B.; et al. Renal 123I-MIBG Uptake before and after Live-Donor Kidney Transplantation. Diagnostics 2020, 10, 802.
- Qaim, S.M.; Scholten, B.; Neumaier, B. New Developments in the Production of Theranostic Pairs of Radionuclides. J. Radioanal. Nucl. Chem. 2018, 318, 1493–1509.
- Barca, C.; Griessinger, C.; Faust, A.; Depke, D.; Essler, M.; Windhorst, A.; Devoogdt, N.; Brindle, K.; Schäfers, M.; Zinnhardt, B.; et al. Expanding Theranostic Radiopharmaceuticals for Tumor Diagnosis and Therapy. Pharmaceuticals 2021, 15, 13.
- Spitzweg, C.; Dietz, A.; O’Connor, M.; Bergert, E.; Tindall, D.; Young, C.; Morris, J. In Vivo Sodium Iodide Symporter Gene Therapy of Prostate Cancer. Gene Ther. 2001, 8, 1524–1531.
- Boland, A.; Ricard, M.; Opolon, P.; Bidart, J.M.; Yeh, P.; Filetti, S.; Schlumberger, M.; Perricaudet, M. Adenovirus-Mediated Transfer of the Thyroid Sodium/Iodide Symporter Gene into Tumors for a Targeted Radiotherapy. Cancer Res. 2000, 60, 3484–3492.
- Chen, E.; Wang, J.; Zhang, H.; Zhang, Y.; Jia, C.; Min, X.; Liang, Y. Analysis of the Efficacy and Safety of Iodine-125 Seeds Implantation in the Treatment of Patients with Inoperable Early-Stage Non-Small Cell Lung Cancer. J. Contemp. Brachytherapy 2021, 13, 347–357.
- Pavlicek, W.; Walton, H.A.; Karstaedt, P.J.; Gray, R.J. Radiation Safety with Use of I-125 Seeds for Localization of Nonpalpable Breast Lesions. Acad. Radiol. 2006, 13, 909–915.
- Mansouri, M.; Shahbazi-Gahrouei, D. A Review on Theranostic Applications of Iodine Nanoparticles: Recent Findings and Perspectives. Nanomedicine J. 2021, 8, 234–240.
- Zimmermann, M.B. Iodine Deficiency Disorders and Their Correction Using Iodized Salt and/or Iodine Supplements. In Iodine Chemistry and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; Volume 9781118466, pp. 421–431.
- Yoshida, S.; Ojino, M.; Ozaki, T.; Hatanaka, T.; Nomura, K.; Ishii, M.; Koriyama, K.; Akashi, M. Guidelines for Iodine Prophylaxis as a Protective Measure: Information for Physicians. Japan Med. Assoc. J. JMAJ 2014, 57, 113–123.
- Küpper, F.C.; Kroneck, P.M.H. Iodine Bioinorganic Chemistry. In Iodine Chemistry and Applications; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2014; pp. 555–589.
- Dreger, S.; Pfinder, M.; Christianson, L.; Lhachimi, S.K.; Zeeb, H. The Effects of Iodine Blocking Following Nuclear Accidents on Thyroid Cancer, Hypothyroidism, and Benign Thyroid Nodules: Design of a Systematic Review. Syst. Rev. 2015, 4, 126.
- Markou, K.; Georgopoulos, N.; Kyriazopoulou, V.; Vagenakis, A.G. Iodine-Induced Hypothyroidism. Thyroid 2001, 11, 501–510.
- World Health Organization. Protection of the Human Environment. Guidelines for Iodine Prophylaxis Following Nuclear Accidents; Update 1999; World Health Organization: Geneva, Switzerland, 1999; pp. 1–45.