Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Gianluca Aguiari and Version 2 by Catherine Yang.
Renal cell carcinoma (RCC) in metastatic form is a lethal pathology difficult to treat; therefore, the research of new therapeutic options for the treatment of metastatic patients is crucial to improve quality of life and overall survival.
- kidney cancer
- signaling
- autophagy
1. Introduction
Metastatic renal cell carcinoma (mRCC) is a lethal form of RCC that is very hard to cure. In fact, subjects with mRCC at 5 years from diagnosis show an overall survival (OS) lower than 10% [1]. Approximately 30% of RCC patients develop metastatic disease at diagnosis, and disease recurrence occurs in about 30% of patients after surgical treatment [2]. The detection of altered signals involved in the pathogenesis of this disease has allowed for the development of specific drugs. In particular, sunitinib and sorafenib (VEGFR inhibitors), as well as other tyrosine kinase inhibitors (TKI), such as pazopanib, axitinib and cabozantinib, have been approved by the FDA for the first-line treatment of mRCC [3]. Temsirolimus and everolimus, inhibitors of the mammalian target of rapamycin (mTOR), were recommended in the first- and second-line treatment of mRCC, respectively [3][4][3,4]. The treatment using these drugs has shown improvements in progression-free survival (PFS) after phase III clinical trials compared with interferon-alpha or other drugs [3][4][3,4]. However, no advantages in survival rate were seen with these agents due to treatment toxicity and drug resistance [2][5][2,5].
2. Clinical Aspects
Worldwide, renal cell carcinoma (RCC) is the sixth most frequently diagnosed cancer in men and the tenth in women, accounting for 5% and 3% of all oncological diagnoses, respectively [6][7]. RCC is mainly divided into three well-defined histotypes; clear cell renal cell carcinoma (ccRCC) makes up about 70% of all kidney cancers. Papillary RCC (pRCC) is the second most common renal tumor. Two subtypes of papillary renal cell cancer have been recognized: papillary type 1 and papillary type 2. The third most common RCC is chromophobe (chRCC) which has a largely empty cytoplasm and low mitotic rate. In general, this tumor has the lowest risk of developing metastases [7][8][8,9].
2.1. Tumor Staging
The therapeutic options and management of RCC are stage-dependent; consequently, accurate staging is essential to effective management [8][9]. Kidney primary tumors can be classified in the following groups:
T1: Tumor is confined to the kidney and is subdivided into T1a and T1b. T1a: tumor is 4 cm or less in size; T1b: tumor is between 4 and 7 cm.
T2: Tumor is limited to the organ and is divided into T2a and T2b. T2a: tumor is between 7 and 10 cm; T2b: tumor is more than 10 cm.
T3: Tumor extends into major veins or perinephric tissues and is divided into T3a, T3b, and T3c. T3a: tumor extends into the renal vein or invades the pelvicalyceal system or spreads into perirenal and/or renal sinus fat; T3b: tumor extends into vena cava below diaphragm; T3c: tumor extends into the vena cava above the diaphragm or invades the wall of the vena cava.
T4: Tumor invades beyond Gerota fascia (including contiguous extension into the ipsilateral adrenal gland).
Renal cancer staging is based on the tumor node metastasis (TNM) classification system and includes four different stages.
Stage I: Includes T1 tumors without lymph node or distance metastasis. Partial nephrectomy (PN) or radical nephrectomy (RN) are recommended.
Stage II: Includes T2 tumors without lymph node or distance metastasis. Surgery including PN and RN is an option for the resection of tumor masses.
Stage III: Includes T3 tumors without lymph node or distance metastasis and T1–T3 tumors with metastasis in regional lymph nodes, but not distance metastasis. RN or PN (if clinically indicated) are recommended as surgical treatment.
Stage IV: Includes T4 tumors with any lymph node without distance metastasis as well as T1–T4 tumors with any lymph node and distance metastasis. RN could be an option for patients with localized disease. Cytoreductive nephrectomy (CN) before systemic therapy might be an option for mRCC patients with surgically treatable primary tumors. In fact, studies conducted in the cytokine era showed that combined treatment with CN and interferon enhanced the survival of patients compared with subjects treated with interferon alone. Conversely, the CARMENA study reported that OS in patients treated with sunitinib alone was not inferior to CN followed by sunitinib [9][10][10,11]. Based on these observations, the immediate systemic treatment for mRCC patients is recommended [9][10].
2.2. Trends in the Surgical Management of RCC
RN remains the gold standard treatment for localized renal masses in any patient not suitable for nephron-sparing surgery (NSS). In particular, the laparoscopic technique shows equivalent oncologic outcomes as compared to open RN (ORN), but with a faster recovery, lower blood loss, and decreased complication rates [11][12]. Laparoscopy quickly became the favorite approach for patients with localized renal cancer requiring RN [12][13][13,14]. The emergence of the robotic platform in the early 2000s has again shifted the surgical approach to this disease. This technique has also affected RN, as seen by the increasing utilization of the robotic platform. The Premier Healthcare database shows that the use of the robotic approach increased from 1.5% in 2003 to 27% in 2015 [14][15]. However, RN with the robotic approach shows no clear benefit as compared to a laparoscopic one but is significantly easier to learn and perform as compared to the laparoscopic approach [15][16]. Recently, the rise of the robotic platform has significantly changed the NSS approach. Outcome data for robotic partial nephrectomy (RPN) compared to laparoscopic (LPN) and open (OPN) have been promising, showing RPN to be superior to the other techniques. Different studies have shown that RPN is better than OPN for blood loss, transfusions, complications, hospital stay, readmissions, overall mortality, and the recurrence rate of disease [16][17]. The rapid evolution of the robotic-assisted approach has become the most common and favorable surgical approach for the management of RCC.
2.3. Management of RCC Patients after Diagnosis
Nonmetastatic RCC patients with localized disease and subjected to partial or radical nephrectomy are monitored by surveillance. Follow-up should be personalized based on the patient’s needs. Adjuvant therapy, by using TKIs for high-risk nonmetastatic RCC patients after nephrectomy, was approved by the FDA, but is not recommended by EAU guidelines. In fact, the S-TRAC study showed that treatment with sunitinib improved disease-free survival (DFS), yet without any OS benefit [9][10]. Recently, the availability of novel drugs, including ICIs, has improved the efficacy of adjuvant therapies. In this regard, the Keynote-564 trial reported that treatment with pembrolizumab enhanced DFS in high-risk nonmetastatic RCC patients subjected to nephrectomy as compared to placebo [9][17][10,18]. These observations indicate that pembrolizumab could be used as adjuvant therapy for high-risk RCC. However, before recommending this therapy, it would be appropriate to know the data on OS, currently not yet available [9][10].
Metastatic RCC patients are risk-stratified into favorable, intermediate, and poor-risk categories. Recently, the integration of molecular data with annotated genomic models showed an improved stratification of patients across the different risk groups. In particular, the standard of care for the treatment of favorable risk patients is the use of pembrolizumab/Axitinib, pembrolizumab/Lenvatinib, or nivolumab/cabozantinib. For intermediate and poor-risk, the recommended treatment is nivolumab/cabozantinib, pembrolizumab/axitinib, pembrolizumab/Lenvatinib, or nivolumab/ipilimumab [18][6].
3. Signaling Related to RCC
The most common RCC (ccRCC histotype) is linked to well-known altered-signaling pathways such as the von Hippel–Lindau (VHL), vascular endothelial growth factor receptor (VEGFR), and the phosphoinisitide-3 kinase/mammalian target of rapamycin (PI3K/mTOR) protein kinases. Currently, it has emerged that new pathways, including receptor tyrosine kinases (RTKs) hyper-activation, p53 damage, and autophagy dysfunction, are involved in ccRCC pathogenesis and drug resistance.
The main biological processes involved in renal carcinogenesis are described below and in Figure 1.
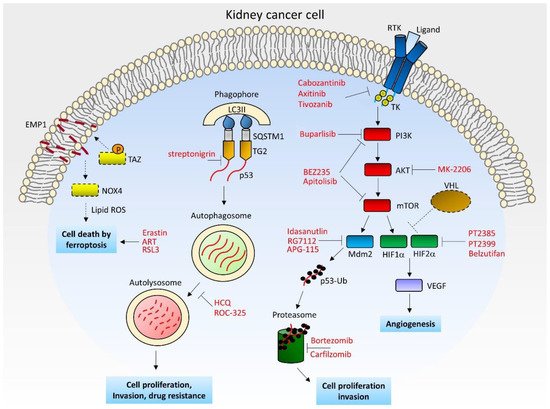
Figure 1. Schematic model of kidney cancer cell with the mainly pathogenic pathways/processes and relative inhibitors/activators. Dashed lines and boxes indicate the inactivated components in RCC. ART: Artesunate; EMP1: Epithelial membrane protein 1; HCQ: Hydroxychloroquine; HIF: Hypoxia-inducible factor; LC3II: Microtubule-associated protein light chain 3B; MDM2: Mouse double minute 2 homolog; mTOR: Mammalian target of rapamycin; NOX4: NADPH oxidase 4; PI3K: Phosphatidylinositol 3-kinase; ROS: Reactive oxygen species; RTK: Receptor tyrosine kinase; SQSTM1: Sequestosome-1; TAZ: Transcriptional co-activator with PDZ-binding motif; TG2: Transglutaminase 2; TK: Tyrosine kinase domain; Ub: Ubiquitin; VEGF: Vascular endothelial growth factor; VHL: von Hippel–Lindau.
4. Current and New Targeted Therapies for RCC Treatment
The pharmacological therapies for the treatment of mRCC patients move fast. In fact, the monotherapy with tyrosine kinase inhibitors targeting the VEGF receptor to inhibit angiogenesis was replaced with more effective therapies.
4.1. TK Inhibitors
Treatment with first-generation TKIs such as sunitinib, sorafenib, and pazopanib in mRCC patients leads to the development of primary and acquired resistance to these drugs. Thus, these therapeutic agents could be replaced with more efficient TKIs, such as cabozantinib, axitinib, Lenvatinib, and tivozanib [19][20][42,43]. Cabozantinib is an inhibitor of multiple tyrosine kinases, including VEGFR, MET, and Axl, which are associated with aggressive disease and poor survival [19][42]. The treatment with cabozantinib showed an increased PFS in mRCC patients compared with sunitinib [21][44]. Axitinib is an anti-angiogenic multi-receptor inhibitor that, in clinical trials, showed greater objective response rates and improved median PFS compared with sorafenib [4][20][4,43]. Lenvatinib is a multitarget tyrosine kinase inhibitor that inhibits VEGFR, FGFR, PDGFR, RET, and KIT. The administration of this drug has shown antitumor properties against mRCC [22][45]. Finally, tivozanib, a novel selective VEGFR inhibitor, was approved for the treatment of advanced RCC by the European Medicines Agency (EMA) [20][23][43,46]. The treatment with tivozanib showed a PFS advantage compared with sorafenib; however, overall survival results favored sorafenib, yet other studies should be carried out to evaluate the efficacy of this drug [23][24][46,47]. The combination of axitinib, cabozantinib, and lenvatinib with different PD-1 immune checkpoint inhibitors in a first-line setting has shown superior efficacy in patients with advanced RCC compared with single-drug therapies [18][25][6,48]. Therefore, the latest guidelines recommend the use of these TKIs in first-line treatment in combination with immunotherapeutic drugs [18][6].
4.2. HIF2 Alpha Antagonists and PI3K-Related Inhibitors
The targeting of the HIF pathway seems a promising option for treating patients with metastatic ccRCC. In fact, treatment with the HIF2 antagonist PT2399 showed greater activity than sunitinib and was well tolerated in mice models for ccRCC [26][49]. However, prolonged PT2399 treatment leads to resistance. Moreover, some cases of drug resistance were observed despite HIF2 inactivation, suggesting that some ccRCCs are HIF2-independent [26][49]. The same research group has also developed and tested a second HIF2 antagonist (PT2385) that is able to inhibit HIF2 binding as well as HIF-2-related gene expression. PT2385 was safe and active in a first-in-human phase I clinical trial of patients with extensively pre-treated ccRCC; however, follow-up data on PFS and OS are not yet available. As with PT2399, the prolonged treatment with PT2385 leads to drug resistance, likely due to HIF2 mutations [27][50]. Another HIF2 inhibitor, belzutifan, is an oral small molecule used for the treatment of solid tumors, including renal cell carcinoma. In a phase-1 study, belzutifan was well tolerated and demonstrated preliminary anti-tumor activity in patients pre-treated with antiangiogenic drugs. The main side effect in patients treated with belzutifan is anemia due to erythropoietin reduction [28][51]. Recently, a phase-II clinical trial using belzutifan in patients with renal carcinomas associated with VHL disease was completed. Results indicate that the treatment with belzutifan induces a reduction in tumor size in most patients [29][52]. In particular, about half of enrolled patients (49%) treated with belzutifan have shown an objective response. Only a few patients (3%) had progressive disease, and one subject (2%) discontinued the treatment because of an adverse event [29][52]. The efficacy of belzutifan, combined with these modest side effects, make this drug an important option for mRCC treatment.
The abnormal activation of PI3K is involved in the development of renal cell carcinoma, making this kinase and its relative signaling an attractive target for therapeutic intervention. Phase-II studies of mRCC patients previously treated with anti-VEGFR drugs by using MK-2206, an allosteric inhibitor of AKT, did not show significant differences when compared to studies of patients treated with the mTOR inhibitor everolimus [30][53]. In addition, a significant number of patients treated with MK-2206 developed a rash and hyperglycemia, as observed in patients treated with other PI3K-pathway inhibitors, such as BEZ235, apitolisib, and buparlisib [30][53]. Treatments with BEZ235 or apitolisib, dual PI3K and mTOR inhibitors in mRCC patients, showed high toxicity without objective improvements [31][32][54,55]. Finally, the treatment with buparlisib, a pan-class I phosphoinositide 3-kinase inhibitor, in combination with bevacizumab, showed different side effects, including elevated lipase/amylase, anorexia, and psychiatric disorders. Moreover, the objective responses obtained by this combined therapy were lower compared with the combination of bevacizumab and mTOR inhibitors [33][56].
The modest efficacy of these agents observed in RCC patients might be explained by the extensive crosstalk and negative feedback mechanisms typical of PI3K-related pathways [30][53].
4.3. Anti MDM2 Drugs and Proteasome Inhibitors
Since p53 may be removed by MDM2-proteasome machinery in kidney tumor cells [34], this system represents a possible target for cancer therapy. In this regard, the inhibition of MDM2 reduced tumor size in pre-clinical models for ccRCC. Furthermore, the combined treatment of MDM2 inhibitors and everolimus showed a synergistic effect decreasing cell growth in ccRCC for “in vitro” and “in vivo” models [35][57]. However, specific clinical trials targeting MDM2 in kidney cancer have to still be planned. Conversely, different clinical trials in solid tumors and hematologic neoplasms by using MDM2 inhibitors, such as RG7112, idasanutlin, APG-115, and ALRN-6924, have already completed phase-1 trials [36][37][58,59]. Most of these seem well tolerated except for RG7112, which shows different side effects. Nevertheless, some MDM2 inhibitors show ineffectiveness, while clinical trials testing other MDM2 antagonists are currently in progress [36][58].
The targeting of proteasome machinery with specific inhibitors might be another way to preserve wild-type p53 and arrest tumor growth. The use of bortezomib, a small inhibitor molecule of proteasome, is able to induce apoptosis in different RCC cell lines. Unfortunately, a phase-II study testing the combination of sorafenib and bortezomib did not show improvements in PFS compared with sorafenib monotherapy despite the combined drugs being well tolerated [38][60]. Another promising proteasome blocker is carfilzomib; this agent is a specific inhibitor for the chymotrypsin-like active site of the 20S proteasome. The treatment with this compound showed antitumoral activity not only in RCC tumor cell lines but also in a patient-derived xerograph (PDX) [39][61]. Nevertheless, in a phase-II study with mRCC patients it emerged that carfilzomib failed clinical trials since all enrolled patients had disease progression and different side effects [40][62]. Taken together, these observations suggest that proteasome inhibitors seem unsuitable for the treatment of metastatic renal carcinoma.
4.4. Autophagy and TG2 Inhibitors
Patients suffering from mRCC treated with multiple targeted therapies have acquired drug resistance and a loss of efficiency. Therapy resistance might be caused by drug sequestration in lysosomal vesicles. Actually, it was demonstrated that autophagy is able to remove and degrade the tyrosine kinase inhibitor sunitinib in kidney cancer cells [41][63]. Therefore, the targeting of autophagy could be an appealing idea for the treatment of metastatic kidney cancer. It was observed that the modulation of autophagy might enhance the cytotoxicity of therapeutic agents and reduce drug resistance [42][64]. In particular, clinical trials using the autophagy inhibitor hydroxychloroquine (HCQ) in combination with everolimus have shown a better PFS compared with everolimus alone in mRCC patients previously treated with tyrosine kinase inhibitors. Moreover, the combined treatment was well tolerated since only in some cases drug-related toxicity was observed [43][65]. Other promising autophagy inhibitors, including ROC-325, are currently being used in pre-clinical studies and have shown anticancer activity [42][64]. Recent studies have further demonstrated that p53 sequestration into autophagosomes occurs through its interaction with the enzyme TG2, which connects p53 with the autophagic protein SQSTM1/p62 [44][38]. Moreover, autophagy-related drug resistance appears to be mediated by TG2; therefore, the inhibition of this enzyme might prevent drug resistance, improving cancer therapy [45][66]. Consistently, it was reported that treatment with streptonigrin, a TG2 inhibitor, was able to reduce cancer cell growth in a xenograft model of RCC, confirming that the targeting of TG2 exerts anticancer properties [45][66].
4.5. Ferroptosis Activators
Different studies have demonstrated that the induction of ferroptosis by erastin and sorafenib is able to inhibit tumor progression and retrieve therapeutic effectiveness. Therefore, the combination of chemotherapeutic drugs and ferroptosis inducers could be a further option to improve the overall survival of patients with advanced kidney carcinoma [46][41]. Recently, it was reported that treatment with artesunate (ART), a traditional Chinese medicine drug, has shown anticancer properties. In fact, ART is able to reduce cell proliferation and kill tumor cells in different RCC cell lines. In particular, ART works by increasing the number of ROS species and inhibiting GPX4 in a mechanism involving p53, ultimately leading to cell death by ferroptosis in KTCTL-26 cells. However, the mechanism of cell killing induced by ART in other RCC cell lines, such as Caki-1, 786-O, and A-498, is different since increased ferroptosis activity in these cells was not observed [47][67]. Taken together, these observations indicate that ART might act in different ways depending on tumor type or tumor heterogeneity. Another study has demonstrated that the induction of ferroptosis by erastin and RSL-3 in combination with everolimus inhibits the viability of RCC cells and may overcome drug resistance problems observed after everolimus treatment [48][68]. To evaluate the possible anticancer properties of ferroptosis in RCC, clinical trials using ferroptosis activators alone or in combination with other chemotherapeutic agents should be approached.
4.6. Immunotherapy
The continuous demand for more efficient therapies for the treatment of mRCC has led to the discovery of new agents, including immune-oncology drugs such as immune checkpoint inhibitors (ICIs). Immunotherapy for the treatment of advanced RCC by using interleukins or interferon has already been attempted, but with poor results [49][69]. Currently, new immune-based drugs such as nivolumab, ipilimumab, pembrolizumab, and avelumab, have been generated. Interestingly, it was observed that adjuvant treatment with pembrolizumab, an anti-programmed death 1 (PD-1) monoclonal antibody, prolongs DFS in high-risk patients with nonmetastatic RCC subjected to nephrectomy [17][18]. As previously mentioned, the treatment with ICIs combined with TKIs is recommended for the first-line treatment of mRCC [18][6]. In addition, dual treatment using the monoclonal antibody anti-PD ligand-1 (PD-L1), avelumab, and the TK inhibitor axitinib, was also approved by the FDA for the treatment of all risk groups of RCC [50][70]. Importantly, the combination of nivolumab (anti-PD-1 monoclonal antibody) and ipilimumab (anti-cytotoxic T-lymphocyte-associated protein-4 (CTLA4)) represents the standard of care for RCC patients under intermediate or poor-risk [18][6]. Other innovative immunotherapies include the use of modified cytokines, cellular therapies, and anticancer vaccines [51][71]. Despite promising results obtained with ICI-based therapies, long-term treatments using ICIs in RCC patients may induce mechanisms of resistance, decreasing the clinical benefits [49][69]. Therefore, the research of predictive biomarkers for the therapeutic response in RCC patients treated with ICIs is needed.