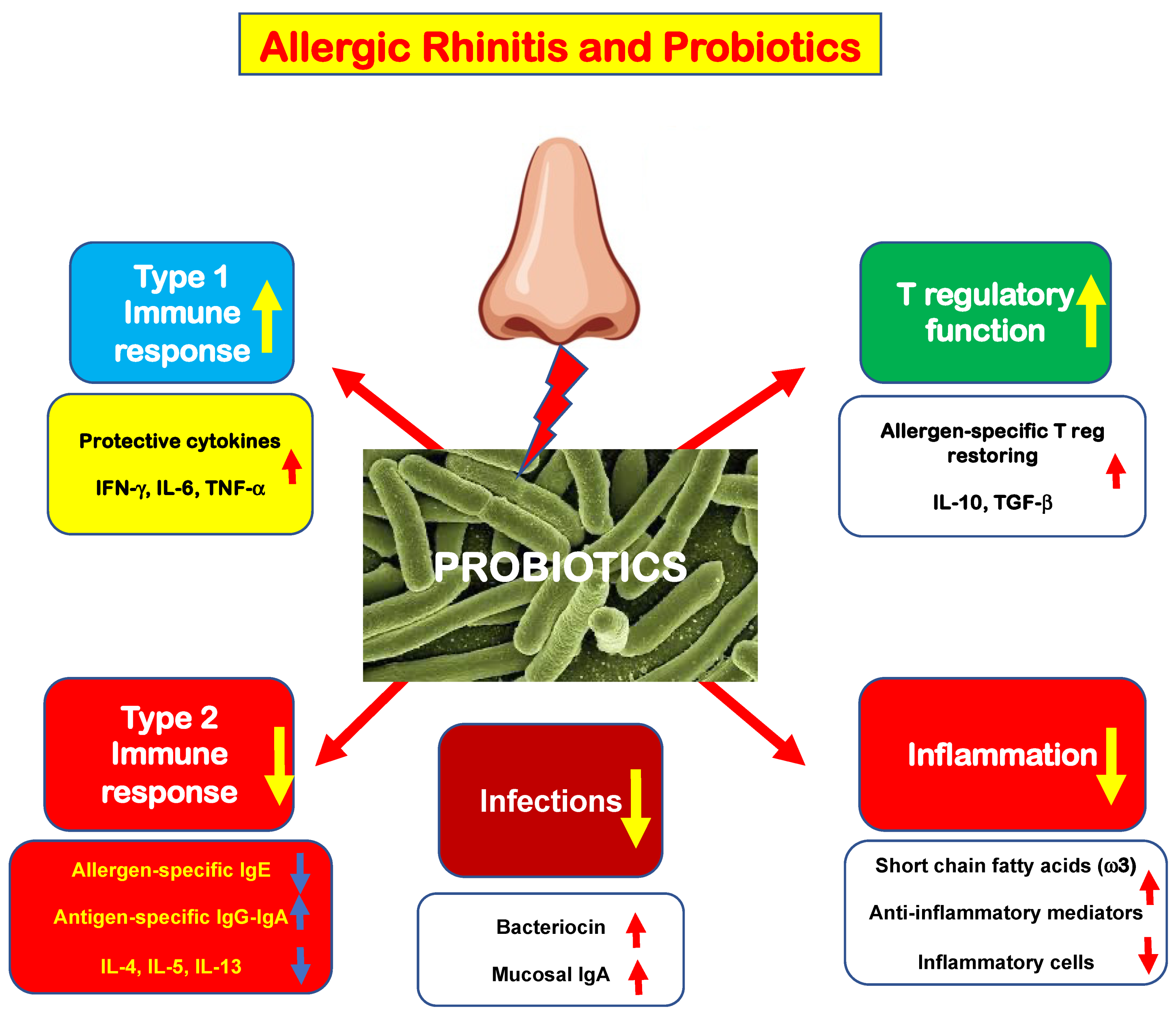
Allergic rhinitis (AR) is a common medical condition affecting up to 40% of the general population. A type 2 immunity determines eosinophilic inflammation that, in turn, elicits typical nasal symptoms. Type 2 immunity is eminently characterized by polarization of innate and adaptative B and T cells, increased production of type 2 cytokines, including interleukin-4 (IL-4), IL-5, and IL-13, and impaired function of allergen-specific T regulatory cells (Tregs). This immunologic derangement promotes allergic inflammation, characterized by an abundant eosinophilic infiltrate and the presence of mast cells. The mast cells are activated by allergen exposure and release pro-inflammatory mediators, including histamine. These mediators interact with specific receptors and, consequently, are responsible for the appearance of typical AR symptoms: nasal itching, sneezing, rhinorrhea, and nasal congestion.
- oral probiotics
- allergic rhinitis
- dysbiosis
- inflammation
- immunity
1. The Rationale for Probiotic Use in Allergic Rhinitis Management
2. New Evidence in the Literature
Four more studies on the use of probiotics in the treatment of AR have been published in the past year, which were not covered by the meta-analyses mentioned above. Therefore, they will be presented here to provide updated knowledge about this issue. The first study aimeds to investigate the probiotic prophylactic treatment in children with AR [48][25]. The tested compound was a probiotic mixture including Bifidobacterium animalis subsp. Lactis BB12 and Enterococcus faecium L3. The outcome measures were nasal symptom scores and the need for rescue medication. The study included 250 children and adolescents. Subjects were stratified into two groups: actively treated (150) or control (100). The probiotic mixture was administered three months before the pollen season. Patients treated with probiotics experienced less severe symptoms than controls. Consistently, probiotic-treated children used less symptomatic drugs than controls. Consequently, the investigators concluded that the mixture containing BB12 and L3 exerted significant preventive effects on the AR course. The second study explored the effects of a commercial probiotic preparation containing four strains: Lactobacillus acidophilus LA02, Lactobacillus delbrueckii LDB01, Lactobacillus rhamnosus LR04, and Streptococcus thermophilus FP04 [49][26]. Twenty-eight AR patients took the probiotic mixture for 60 days; they were evaluated at baseline, after the treatment, and during a two-month follow-up. The probiotic product significantly reduced rhinitis total symptom scores and visual analog scale. Consistently, probiotics reduced the peripheral eosinophils, the levels of type 2 cytokines IL-4 and IL-5, and increased biodiversity in stool microbiota composition. Interestingly, the microbiota changes correlated with clinical and immunological parameters. Consequently, the study concluded that this probiotic preparation could be envisaged as a helpful add-on strategy in AR patients. The outcomes provided by this study were particularly impressive, mainly concerning the cytological and immunological results. It has to be noted that such positive results were not observed by most other studies exploring these aspects. However, it should be emphasized that this study should be considered a preliminary study conducted on a small sample of patients. Therefore, these results, which are undoubtedly attractive, need confirmation by studies conducted with a more robust and appropriate methodology. Another study evaluated an intranasally administered probiotic assemblage containing Lactobacillus rhamnosus SP1, Lactobacillus paracasei 101/37, and Lactococcus lactis L1A, compared with placebo [50][27]. Participants were subdivided into two groups: actively treated (12) and placebo-treated (12). Treatment lasted three weeks. Outcome measures were quality of life scores, total nasal symptom score, peak nasal inspiration flow, fractional exhaled nitric oxide, and cytokines assay. Cultures were also performed to detect the colonization of strains. Unfortunately, the only significant result concerned a slight decrease in IL-17. Therefore, the authors concluded that the topical administration of a probiotic mixture was ineffective in AR patients. Probably, the duration and the topical route were inadequate to observe benefits. Finally, an Australian study investigated the effects of a probiotic drink (“NC-Seasonal-Biotic”) containing four strains: Lactobacillus reuteri GL 104, Lactobacillus plantarum LPL28, Lactobacillus rhamnosus MP108, and Bifidobacterium lactis BI04, and a fructooligosaccharide as prebiotic, compared with placebo [51][28]. Forty patients concluded the 10–12-week intervention period. The active group showed a significant improvement in clinical parameters and consistent quality of life scores. In addition, the probiotic drink restored the Th1/Th2 ratio. These recent studies, therefore, added new proof evidencing that probiotics could help manage patients suffering from AR. However, two main lessons have to be acknowledged. First, the probiotic supplementation duration should be adequate to allow colonization and completion of the immunological mechanism of action. Second, the effectiveness depends on the specificity of single strains. Moreover, the outcomes reported in AR were substantially consistent with what has been reported in the asthma model [52,53,54][29][30][31].References
- Strachan, D.P. Hay fever, hygiene, and household size. BMJ 1989, 299, 1259–1260.
- Haahtela, T. A biodiversity hypothesis. Allergy 2019, 74, 1445–1456.
- Convention on Biological Diversity. 1992. Available online: www.biodiv.org/convention (accessed on 4 July 2022).
- Hufnagl, K.; Pali-Schoell, I.; Roth-Walter, F.; Jensen-Jarolim, E. Dysbiosis of the gut and lung microbiome has a role in asthma. Sem. Immunopathol. 2020, 42, 75–93.
- Cukrowska, B.; Bierła, J.B.; Zakrzewska, M.; Klukowski, M.; Maciorkowska, E. The Relationship between the Infant Gut Microbiota and Allergy. The Role of Bifidobacterium breve and Prebiotic Oligosaccharides in the Activation of Anti-Allergic Mechanisms in Early Life. Nutrients 2020, 12, 946.
- Kang, Y.B.; Cai, Y.; Zhang, H. Gut microbiota and allergy/asthma: From pathogenesis to new therapeutic strategies. Allergol. Immunopathol. (Madr) 2017, 45, 305–309.
- Dang, A.T.; Marsland, B.J. Microbes, metabolites, and the gut-lung axis. Mucosal Immunol. 2019, 12, 843–850.
- Matsubara, A.; Nomura, A.; Yamaguchi, T. The relationship between allergic rhinitis and gut microbiota. Aerugi. 2022, 71, 191–194.
- Lopez-Santamarina, A.; Gonzalez, E.G.; Lamas, A.; Mondragon, A.D.C.; Regal, P.; Miranda, J.M. Probiotics as a Possible Strategy for the Prevention and Treatment of Allergies. A Narrative Review. Foods 2021, 10, 701.
- FAO/WHO. Expert Consultation Health and Nutrition Properties of Probiotics in Food Including Powder Milk with Live Lactic Acid Bacteria. Available online: http://isappscience.org/wp-content/uploads/2015/12/FAO-WHO-2001-ProbioticsReport.pdf (accessed on 4 July 2022).
- Plaza-Diaz, J.; Ruiz-Ojeda, F.J.; Gil-Campos, M.; Gil, A. Mechanisms of action of probiotics. Adv. Nutr. 2019, 10, 549–566.
- Wang, H.T.; Anvari, S.; Anagnostou, K. The role of probiotics in preventing allergic disease. Children 2019, 6, 24.
- Balta, I.; Butucel, E.; Mohylyuk, V.; Criste, A.; Dezmirean, D.N.; Stef, L.; Pet, I.; Corcionivoschi, N. Novel insights into the role of probiotics in respiratory infections, allergies, cancer, and neurological abnormalities. Disease 2021, 9, 60.
- Maldonado Galdeano, C.; Cazorla, S.I.; Lemme Dumit, J.M.; Velez, E.; Perdigon, G. Beneficial effects of probiotic consumption on the immune system. Ann. Nutrit. Metabol. 2019, 74, 115–124.
- Al Nabhani, Z.; Eberl, G. Imprinting of the immune system by the microbiota early in life. Mucosal Immunol. 2020, 13, 183–189.
- Huang, J.; Zhang, J.; Wang, X.; Jin, Z.; Zhang, P.; Su, H.; Sun, X. Effect of probiotics on respiratory tract allergic disease and gut microbiota. Front. Nutr. 2022, 9, 821900.
- Cristofori, F.; Dargenio, V.N.; Dargenio, C.; Miniello, V.L.; Barone, M.; Francavilla, R. Anti-inflammatory and immunomodulatory effects of probiotics in gut inflammation: A door to the body. Front. Immunol. 2021, 12, 578386.
- Lin, C.; Lin, Y.; Zhang, H.; Wang, G.; Zhao, J.; Zhang, H.; Chen, W. Intestinal “Infant-Type” Bifidobacteria mediate immune system development in the first 1000 days of life. Nutrients 2022, 14, 1498.
- Das, R.R.; Naik, S.S.; Singh, M. Probiotics as additives on therapy in allergic airway diseases: A systematic review of benefits and risks. BioMed Res. Int. 2013, 2013, 231979.
- Guvenc, I.A.; Bayar Muluk, N.; Mutlu, F.S.; Eski, E.; Altintoprak, N.; Oktemer, T.; Cingi, C. Do probiotics have a role in the treatment of allergic rhinitis? A comprehensive systematic review and meta-analysis. Am. J. Rhinol. Allergy. 2016, 30, 157–175.
- Lin, J.; Zhang, Y.; He, C.; Dai, J. Probiotics supplementation in children with asthma: A systematic review and meta-analysis. J. Ped. Child Health 2018, 54, 953–961.
- Du, X.; Wang, L.; Wu, S.; Yuan, L.; Tang, S.; Xiang, Y.; Qu, X.; Liu, H.; Qin, X.; Liu, C. Efficacy of probiotic supplementary therapy for asthma, allergic rhinitis, and wheeze: A meta-analysis of randomized controlled trials. Allergy Asthma Proc. 2019, 40, 250–260.
- Wei, X.; Jiang, P.; Liu, J.; Sun, R.; Zhu, L. Association between probiotic supplementation and asthma incidence in infants: A meta-analysis of randomized controlled trials. J. Asthma 2020, 57, 167–178.
- Meirlaen, L.; Levy, E.I.; Vandenplas, Y. Prevention and management with pro-, pre- and synbiotics in children with asthma and allergic rhinitis: A narrative review. Nutrients 2021, 13, 934.
- Anania, C.; Di Marino, V.P.; Olivero, F.; De Canditiis, D.; Brindisi, G.; Iannilli, F.; De Castro, G.; Zicari, A.M.; Duse, M. Treatment with a Probiotic Mixture Containing Bifidobacterium animalis Subsp. Lactis BB12 and Enterococcus faecium L3 for the Prevention of Allergic Rhinitis Symptoms in Children: A Randomized Controlled Trial. Nutrients 2021, 13, 1315.
- Torre, E.; Sola, D.; Caramaschi, A.; Mignone, F.; Bona, E.; Fallarini, S. A Pilot Study on Clinical Scores, Immune Cell Modulation, and Microbiota Composition in Allergic Patients with Rhinitis and Asthma Treated with a Probiotic Preparation. Int. Arch. Allergy Immunol. 2022, 183, 186–200.
- Mårtensson, A.; Nordström, F.U.; Cervin-Hoberg, C.; Lindstedt, M.; Sakellariou, C.; Cervin, A.; Greiff, L. Nasal administration of a probiotic assemblage in allergic rhinitis: A randomised placebo-controlled crossover trial. Clin. Exp. Allergy. 2022, 52, 774–783.
- Ried, K.; Travica, N.; Paye, Y.; Sali, A. Effects of a Probiotic Formulation on Seasonal Allergic Rhinitis in Adults-A Randomized Double-Blind Placebo-Controlled Trial: The Probiotics for Hay Fever Trial. Front. Nutr. 2022, 9, 887978.
- Jakubczyk, D.; Górska, S. Impact of Probiotic Bacteria on Respiratory Allergy Disorders. Front. Microbiol. 2021, 12, 688137.
- Ciprandi, G.; Schiavetti, I.; Cioffi, L.; Pane, M.; Drago, L. The Probiotics in Pediatric Asthma Management (PROPAM) study: A Post Hoc analysis in allergic children. Ann. Allergy Asthma Immunol. 2022, in press.
- Ciprandi, G.; Tosca, M.A. Probiotics in children with asthma. Children 2022, 9, 978.