Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Luca Colangeli and Version 4 by Jessie Wu.
Bariatric surgery (BS) is the most effective treatment in patients with severe obesity in terms of durable weight loss and reduction of comorbidity burden and mortality. Pre-operative weight loss can limit anesthesiological and surgical risks. Ketogenic diet (KD) is an “umbrella term” under which different low-carbohydrate dietary protocols are included. The effect of KD for preoperative weight reduction in BS is described.
- ketogenic diet
- VLCKD
- bariatric surgery
1. Introduction
Bariatric surgery (BS) is the most effective treatment in patients with severe obesity in terms of durable weight loss and the reduction of comorbidity burden and mortality [1][2][1,2].
Among the different surgical techniques, Roux-en-Y gastric bypass (RYGB) and sleeve gastrectomy (SG) are the most commonly used [3] and they are usually performed laparoscopically [4], but in these patients surgical laparoscopic procedures represent a challenge because of the thickness of the abdominal wall, the considerable accumulation of visceral adipose tissue and the increased liver volume [5]. As a matter of fact, despite the overall low mortality rate, surgical complications such as anastomotic leakage, bleeding and infections remain quite common (5–20%) [6]. The excess of visceral fat increases the risk of surgical complications and also increases the conversion rate and operative time [7]. For example, an enlarged liver and the accumulation of visceral fat may hamper the surgical field and this is the cause of the conversions in RYGB in approximately 50% of conversions cases [8]. Moreover, a large neck circumference (>44 cm) often results in difficult intubation and problems with mechanical ventilation [9].
It has been reported that immediate pre-operative weight loss can limit anesthesiological and surgical risks [10] and also seems to improve short- and long-term outcomes [11], but its role is still matter of discussion [12]. In 2016 the American Society for Metabolic and Bariatric Surgery stated that “insurance-mandated preoperative weight loss is not supported by medical evidence and has not been shown to be effective for preoperative weight loss before BS or to provide any benefit for bariatric outcomes” [13]. Indeed, there is a lack of multicenter, randomized, controlled trials on this specific topic [14], so most of the evidence on the effects of pre-operative weight loss come from retrospective studies. Thus, at present, guidelines do not provide any conclusive indication about pre-operative weight reduction [15][16][15,16].
Different approaches used to induce weight loss before surgery have been investigated, such as pharmacotherapy with glucagon-like peptide-1 receptor agonists (GLP-1 RAs) [17] or the combination of a hypocaloric diet with intragastric balloon placement [18], which significantly decreased the rate of conversions and complications in a case-control study [19]. However, diet is probably the most common approach in clinical practice and previous studies have already described the beneficial effect of a Mediterranean diet on weight loss before and after BS [20][21][20,21]. Some authors have reported that patients who show greater adherence to a diet before surgery are also those who lose more weight after surgery, for example, following a low-calorie diet (LCD) [22]. For patients at higher risk, in order to obtain more rapid weight reductions, a very-low-calorie diet (VLCD), characterized by a daily caloric intake of about 600–800 kcal, may be a valid option [23].
Another interesting dietary approach that is more and more frequently used is a ketogenic diet (KD). KD is an “umbrella term” under which different low-carbohydrate dietary protocols are included. The common feature of these diets is that most of the caloric intake is derived from proteins and fats, inducing a fasting-like state with the development of physiological ketosis. For example, a very-low-calorie ketogenic diet (VLCKD) is characterized by a very important reduction in carbohydrate consumption (less than 50 g per day, providing approximately 13% of caloric intake), with adequate protein introduction (about 0.8–1.2 g for each kg of ideal body weight, providing approximately 45% of caloric intake) and a relatively increased consumption of fats (approximately 42% of caloric intake), with an average energy intake of 800 kcal/day [24] (Figure 1). KD is gaining growing popularity because patients usually report satisfaction with this nutritional approach, probably because ketone bodies have anorexigenic, euphoric and mood-stabilizing effects which lead to the reduction of hunger and a feeling of rapid satiety [25].
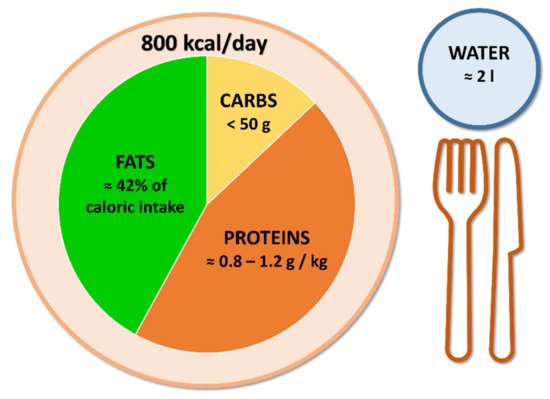
Figure 1.
Very-low-calorie ketogenic diet principles.
Originally used to treat epilepsy in children [26], KD has been demonstrated to be a valid tool for weight management in patients with obesity. Particularly, a recent metaanalysis [27] reported that VLCKD is associated with a mean BMI reduction of 3.25 kg/m2 (95% CI: 2.63 to 3.86) already at 1-month follow-up and up to 7.11 kg/m2 (95% CI: 5.38 to 8.84) after 12-month follow-up, which are also very encouraging results for individuals who are not planning to undergo bariatric surgery. Significant reductions have also been reported in glycated haemoglobin (HbA1c) of 0.43% (95% CI: 0.16 to 0.70) and in low density lipoprotein (LDL) cholesterol of 9.04 mg/dL (95% CI: 4.15 to 13.94), which makes VLCKD a valid nutritional strategy for cardiovascular disease prevention as well, although these results are not superior in comparison with other weight loss interventions.Originally used to treat epilepsy in children [26], KD has been demonstrated to be a valid tool for weight management in patients with obesity. Particularly, a recent metaanalysis [27] reported that VLCKD is associated with a mean BMI reduction of 3.25 kg/m2 (95% CI: 2.63 to 3.86) already at 1-month follow-up and up to 7.11 kg/m2 (95% CI: 5.38 to 8.84) after 12-month follow-up, which are also very encouraging results for individuals who are not planning to undergo bariatric surgery. Significant reductions have also been reported in glycated haemoglobin (HbA1c) of 0.43% (95% CI: 0.16 to 0.70) and in low density lipoprotein (LDL) cholesterol of 9.04 mg/dL (95% CI: 4.15 to 13.94), which makes VLCKD a valid nutritional strategy for cardiovascular disease prevention as well, although these results are not superior in comparison with other weight loss interventions.
Overall, KD has proven to be a valid strategy to induce rapid weight loss [28] and its use before surgery, especially in short-time-available conditions, is particularly attractive [29].
2. Current Evidence and Future Perspectives
The results obtained from studies on KD before BS are summarized in Table 1.
Table 1.
Main findings of studies on KD before BS.| Reference | Population | Intervention Description and Duration | Control Group | Main Findings |
|---|---|---|---|---|
| Leonetti F et al., 2014 [30] | 50 patients (31 F/19 M) |
OPOD regimen: VLCKD for 10 days, VLCD for 10 days, LCD for 10 days |
30 patients (18 F/12 M) standard LCD for 30 days |
Reduction in BMI from 53.5 ± 8.4 kg/m2 to 49.2 ± 8.7 kg/m2 (p < 0.001); improvement in fasting plasma glucose levels; mean 30% reduction in liver volume; improvement of steatosis pattern. |
| Pilone V et al., 2018 [31] | 119 patients (75 F/44 M) |
Sequential diet regimen: VLCKD for 10 days, hypocaloric scheme for 20 days. In addition: multimineral and multivitamin supplements. |
Absent | Reduction in BMI from 41.5 ± 7.6 kg/m2 to 34.1 ± 5.2 kg/m2 (p < 0.001); reduction of fat mass; preservation of fat-free mass; mean 30% reduction in liver volume; improvement of steatosis pattern. |
| Schiavo L et al., 2018 [32] | 27 patients (17 F/10 M) |
Ketogenic micronutrient-enriched diet for 4 weeks | Absent | Reduction in BMI from 46.9 ± 11.7 kg/m2 to 43.0 ± 13.4 kg/m2 (p < 0.001) in females; reduction in BMI from 44.5 ± 10.5 kg/m2 to 40.6 ± 6.5 kg/m2 (p < 0.001) in males; mean 19.8% reduction of left hepatic lobe; improvement in micronutrient status. |
| Albanese A et al., 2019 [33] | 72 patients (60 F/12 M) |
VLCKD for 3 weeks | 106 patients (79 F/27 M) VLCD for 3 weeks |
Total weight loss better in VLCKD than in VLCD group (5.8 ± 2.4 vs. 4.8 ± 2.5 kg, p = 0.008). Surgical outcomes: mean operative time slightly shorter in VLCKD group; percentage of patients requiring a longer-than-anticipated hospital stay lower in VLCKD group; lower drainage output and higher post-operative hemoglobin levels in VLCKD group. |
| Schiavo L et al., 2022 [34] | 34 patients (12 F/22 M) |
CPAP + LCKD for 4 weeks | 36 patients (14 F/22 M) CPAP for 4 weeks |
Apnea-hypopnea score improved in both groups; reduction in BMI (from 50.1 ± 5.9 kg/m2 to 45.3 ± 6.5 kg/m2, p < 0.001) was observed only in CPAP + LCKD group; reduction in CRP levels, blood pressure, HOMA index and cholesterol levels were observed only in CPAP + LCKD group. |
F: females. M: males.
Abbreviations: BMI, body mass index; CPAP, continuous positive airway pressure; CRP, c-reactive protein; F, females; HOMA, homeostasis model assessment; LCD, low-calorie diet; LCKD, low-calorie ketogenic diet; M, males; OPOD, obese pre-operative diet; VLCD, very-low-calorie diet; VLCKD, very-low-calorie ketogenic diet.
Altogether, these studies confirm the usefulness of losing weight before BS and show the potential advantages of VLCKD (Figure 2), particularly if associated with micronutrient integration.
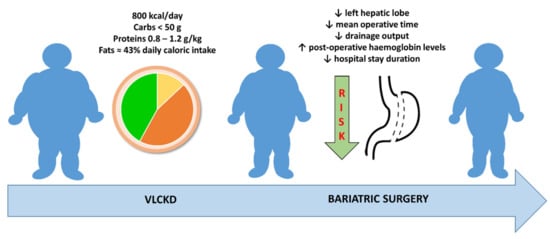
Figure 2.
A very-low-calorie ketogenic diet can be a valid tool to induce weight loss before bariatric surgery, leading to the reduction of surgical risks.
However, the current evidence has some limitations. First of all, the studies presented here are highly heterogeneous in terms of the intervention proposed: because of the small number of studies regarding this subject, rwesearchers decided to take in consideration not only better-defined protocols such as VLCKD [35] but also more generic KDs. Similarly, studies evaluated different outcomes in addition to weight loss, varying from micronutrient status to drainage output. The designs of the studies and the absence of a control group did not allow researcherus to obtain an understanding of the advantages exclusive to KD, other than those generically provided by weight loss. Particularly, regarding improved surgical outcomes, there could be many other explanations other than diet that were not properly analyzed. The number of patients included in these studies is limited and most of the patients were female. Finally, the absence of a follow-up excludes the possibility of investigating potential post-surgery effects. In fact, the reported outcomes should be considered associations rather than being causally related to KD. These issues can be addressed in future research, with the planning of randomized controlled trials with clearly defined dietary protocols, larger populations (with both genders equally represented), clinically relevant outcomes and longer follow-up times to evaluate potential effects that have not yet been investigated.