Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Ioana-Andreea Lungu and Version 5 by Conner Chen.
The resistance of microorganisms has appeared since the first antimicrobial was used [132]. Antimicrobial resistance is the ability of microorganisms (such as bacteria, viruses, fungi, or parasites) to resist the action of an antimicrobial agent.
- antimicrobial resistance
- microorganisms
- bacteria
1. Antimicrobial Resistance
The resistance of microorganisms has appeared since the first antimicrobial was used [1][132]. Antimicrobial resistance is the ability of microorganisms (such as bacteria, viruses, fungi, or parasites) to resist the action of an antimicrobial agent. Antimicrobial resistance may be due to intrinsic resistance (when microorganisms are naturally resistant to the action of certain antibiotics) or acquired (due to the adaptation of microorganisms through genetic modification) [2][3][4][5][133,134,135,136].
It is essential to find out which mechanism underpins the resistance to learn how to combat this threatening phenomenon. Additionally, knowledge of the mechanisms involved helps in the design of new molecules of antimicrobials to overcome resistance. The general mechanisms of antimicrobial resistance are genetic (transfer of genes), mutations, target-mediated mechanisms, inactivation or modification of antimicrobial molecules, reduced uptake of antimicrobials, active efflux, and biofilms [6][7][8][9][137,138,139,140]. Another important aspect is the prudent use of antimicrobials by avoiding their misuse or overuse [10][11][141,142]. Research shows that antibiotic resistance may also occur independently of antibiotic exposure [12][13][143,144].
2. Highlights of the Most Resistant Bacteria Worldwide
According to the World Health Organization (WHO), the most resistant bacteria currently existing are divided into three categories according to how urgent the need to discover new antibiotics is (Table S3, Supplementary Materials) [14][145]. Out of these pathogens, some are resistant to fluoroquinolones (FQNs). The mechanisms by which bacteria develop resistance to FQNs are alterations in target enzymes, altered drug permeation (both in Gram-positive and Gram-negative bacteria), and plasmid acquisition [15][146]. Over time, resistance to FQNs developed alongside researchers’ efforts to improve the molecules of this class [16][17][18][25,147,148].
3. The Development of Antibacterial Resistance over Time
Since the introduction of the first antibiotic in therapy, there have been different levels of interest in the antibiotic resistance phenomenon. Podolsky (2018) described five eras of response to antibiotic resistance. Between 1945 and 1963, when antibiotic resistance appeared to be controlled by the pharmaceutical industry, little effort was undertaken to combat this threat, mainly on a local scale. During 1963–1981, a growing concern arose, fueled by the discovery of bacterial resistance spread across strains or species through what pweople now know as plasmids [19][20][149,150]. Then, from 1981–1992, this threat was beginning to be approached from a more global perspective, raising awareness of the misuse of antibiotics on multiple levels. From 1992–2013, concerns over antibiotic resistance increased; this is a shared global problem that requires interventions spread across various sectors. Finally, from 2013 to the present, the burden of antibiotic resistance is still viewed with great concern while emerging infections with resistant pathogens continue to spread globally [21][151].
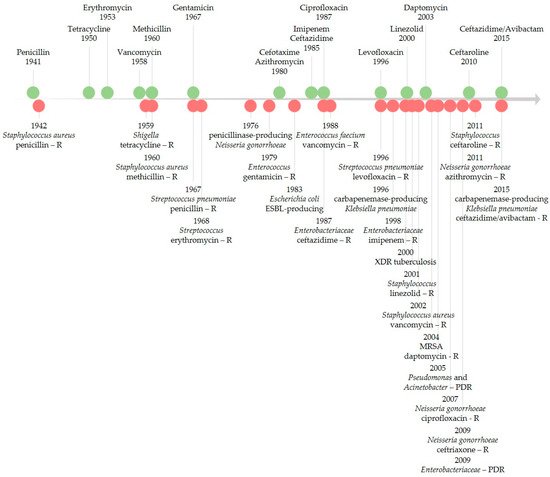
Figure 14 illustrates the timeline of key points of antibiotic resistance occurrences based on early literature reports of resistance and reports of healthcare transmission or outbreaks [22][23][24][152,153,154]. FQNs were no exception for the development of antibacterial resistance [18][25][26][5,148,155]. Resistance to FQNs has arisen after widespread use in humans and animals [27][28][4,156]. Between 2001 and 2006, FQN-resistant E. coli isolates dramatically increased in the United Kingdom (from 6% to 20%). By 2010, it decreased to 17%, a phenomenon possibly linked to changes in prescribing [29][157]. For Enterobacteriaceae (e.g., E. coli), even higher quinolones (QNs) resistance rates were recorded worldwide. In 2015, in the US, reports showed the problematic fact that up to 30% of community-associated isolates were FQN non-susceptible [30][158]. As the figure highlights, antibiotic resistance is a never-ending phenomenon, unfortunately directly linked to the number of used antibiotics [31][159].
4. The Emergence of Resistance to Antibiotics Relatively Recently Introduced in Therapy
There have also been reports of resistance or possible mechanisms of resistance development to antibiotics relatively recently introduced in therapy [32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48][49][50][51][52][53][54][55][56](Table S4, Supplementary Materials) [160,161,162,163,164,165,166,167,168,169,170,171,172,173,174,175,176,177,178,179,180,181,182,183,184]. The leading causes of antibiotic resistance’s rapid emergence are overuse, inappropriate prescribing, and extensive agricultural use. Concerning the availability of new antibiotics, the economic and regulatory obstacles are mainly incriminated in hindering the development of these substances [32][57][58][59][60][61][160,185,186,187,188,189]. Improper or excessive use of antimicrobial agents accelerates the natural process of resistance [62][190]. Without effective antibiotics, the possibility of treating infectious diseases is endangered. Additionally, various medical procedures such as organ transplantation or major surgery could become even riskier. Antimicrobial resistance also impacts rising costs due to extended hospital stays and the need for longer-term intensive care [4][135].
5. New Mechanisms for Bacterial Resistance
Bacteria are constantly gaining resistance due to their genetic plasticity, suffering mutations frequently. They include new genes in their DNA relatively easily through transformation, transduction, and conjugation. These processes allow sharing of the resistance genes from a “gene carrier” bacteria to another. These mutations lead to multiple modifications in the cell and, in the end, to a form of resistance [2][63][64][133,191,192].
A good example is the resistance of Bacteroides fragilis to metronidazole. Bacteroides fragilis is an anaerobic colon resident, but it was found in many extraintestinal infections such as foot, brain, and abdominal infections. The resistance of Bacteroides fragilis is mainly correlated with nim genes in the chromosome or plasmid and multi-drug efflux pumps [65][193].
A complex mechanism of resistance is bacteria-forming biofilms. For example, Pseudomonas aeruginosa is a dangerous pathogen that manifests adaptive antibiotic resistance in addition to its existing resistance mechanisms such as efflux systems, antibiotic-inactivating enzymes, and decreased outer membrane permeability. Adaptive resistance is a response to environmental conditions, and it consists in forming a biofilm and existing in the form of persisting cells that tolerate the antibiotic. The biofilm is an aggregate of bacteria in a polymeric material. Living bacteria in the biofilm are more resistant to antibiotics due to the decreased permeability. In addition, the persisting cells in the biofilm are incapable of replicating in the presence of the antibiotic. Moreover, when the antibiotic is no longer present, they repopulate the biofilm and are responsible for the reactivation of chronic infections [66][194]. In this regard, some ciprofloxacin-nitroxide hybrids synthesized by Verderosa, A.D. et al. (2017) demonstrated the potential to overcome the resistance of biofilms to antimicrobials in two ways: stimulation of biofilm dispersal or direct cell killing [67][195].
On the other hand, the persistence of antibiotics is less understood nowadays. Eisenreich W. et al. (2022) addressed this phenomenon in a recently published review article. They proposed a new theory related to the persistence state of bacteria. So, in this state, bacteria become more susceptible to mutation-based antibiotic resistance [68][196].
6. Resistance to FQNs
There are a few reasons why bacterial resistance to FQNs develops. The dose and duration of administration of the drug are two essential factors. In addition, repetitive exposure and administration of low doses of FQN can enhance bacterial resistance, causing multiple mutations. Therefore, a critical aspect of avoiding bacterial resistance is maintaining a proper schedule of drug administration to ensure that the serum concentrations of FQN are higher than the minimum inhibitory concentration (MIC). Additionally, repeated use of the same agent should be avoided [69][197].
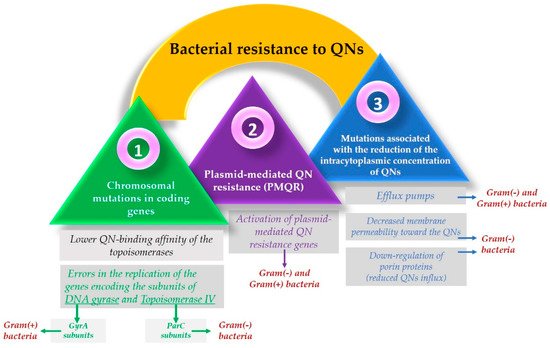
Resistance to FQNs occurs because bacteria use multiple mechanisms to adapt and survive when interacting with the drug [70][71][198,199]. One of the most used resistance mechanisms is the mutation of the genes that encode the type II Topoisomerases. This mechanism focuses on the alteration of the target site known as the quinolone resistance-determining region (QRDR) [72][130] and leads to a lower quinolone-binding affinity of the Topoisomerase enzymes [73][200]. Usually, concerning Gram-negative bacteria, FQNs affect the gyrase while in Gram-positive bacteria, FQNs target the Topoisomerase IV [69][197]. These mutations allow the bacteria to adapt after contact with the FQN [25][5]. So, as a result, it is considered that in Gram-negative bacteria, resistance occurs due to alterations in the DNA gyrase. In contrast, in Gram-positive bacteria, it is due to Topoisomerase IV mutations [74][201].
As DNA gyrase and Topoisomerase IV are cytoplasmic enzymes, achieving low cytoplasmic FQN concentrations is considered another bacteria solution that confers resistance [15][146]. Another mechanism includes mutations that reduce drug accumulation [69][197], such as downregulation of chromosome-encoded porins or increased drug elimination, by multi-drug efflux pumps [73][200]. The maintenance of low concentrations of FQN in the bacterial cells of Gram-positive bacteria results from the action of three efflux pumps, members of the major facilitator superfamily (MFS) of transporters [75][202]. One of them (NorA) is involved in the resistance development of hydrophilic FQN (e.g., norfloxacin). At the same time, the other two (NorB and NorC) are responsible for the resistance to hydrophilic and hydrophobic QNs (e.g., moxifloxacin, sparfloxacin). The efflux pumps are also present in Gram-negative bacteria, part of the transporters’ resistance nodulation-division (RND) superfamily [15][146].
However, unlike Gram-positive bacteria, where resistance results from active efflux transporters [76][33], Gram-negative bacteria have a structural advantage conferred by their double-membrane structure. The cell wall of Gram-negative bacteria acts as a barrier for hydrophilic molecules since the ability to infiltrate through the outer membrane is conditioned by the presence of porin proteins. Mutations that result in the downregulation of these proteins reduce cellular FQN accumulation as a consequence, especially that of the hydrophilic molecules [69][72][74][130,197,201].
Resistance mechanisms can also be encoded in mobile genes called plasmids [69][197], known as plasmid-mediated quinolone resistance (PMQR) genes [77][203]. Some of them encode transporters that can export drugs such as FQNs. Plasmids’ efflux pumps are essential in supporting the resistance to FQNs because they can remove the drug from the bacterial cell [72][130]. Additionally, to protect the bacterial cell from the FQN effect, they can encode topoisomerase-binding proteins or a modified enzyme that decreases FQN activity [73][200].
The activity of older FQNs has been studied to enhance the properties of new compounds regarding the installation of bacterial resistance. It was concluded that with newer FQNs, the bacterial resistance installs less rapidly because of their dual activity against DNA gyrase and Topoisomerase IV [72][78][14,130]. Furthermore, since both targets are equally affected, it would be less likely to elicit mutational resistance [69][197].
Specific structural changes to FQNs have been made to achieve this more complex targeting. This is the example of some fourth-generation representatives of FQNs; they are the result of improving the old FQN’s structure by adding a methoxy radical at the C8 position. This structural change can be found in moxifloxacin and gatifloxacin. In addition to this modification, gatifloxacin has a methyl group on the piperazinyl ring and moxifloxacin has a bicyclic ring in position C7. These structural changes were thought to be responsible for the mechanism of action targeting both DNA gyrase and Topoisomerase IV in Gram-positive bacteria. However, the exact reason these compounds act like this is still unclear. Initially, it was considered that their C8 methoxy group was the trigger for this action. Moreover, it was concluded that this type of targeting was not just the result of the methoxy group because delafloxacin, another FQN, does not possess this radical and is also responsible for the exact targeting [25][74][5,201]. Furthermore, delafloxacin is a more acidic FQN and is consequently more susceptible to deprotonation at a neutral pH. Therefore, as a consequence, delafloxacin shows an improved cellular uptake in acidic conditions [25][5]. The mechanisms involved in the development of bacterial resistance to QNs are illustrated in Figure 25.