Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by John David Heiss and Version 2 by Dean Liu.
Medulloblastoma is the most common pediatric brain tumor, comprising one-third of all pediatric brain tumors, and originating in the posterior fossa of the brain. The disease is categorized into four subtypes: WNT, Sonic hedgehog (SHH), Group 3, and Group 4. Each subtype has unique pathogenesis, biomarkers, prognosis, response to therapy, and potential for further pharmacologic investigation.
- pediatric brain tumors
- medulloblastoma
- molecular subtype
1. Introduction
Medulloblastoma is a central nervous system (CNS) tumor of cerebellar origin that comprises approximately 1% of all brain tumors [1][2][1,2]. However, medulloblastoma is the most common malignant brain cancer in children, accounting for 25–30% of childhood brain tumors and over 40% of posterior fossa childhood tumors [3]. Thus, medulloblastoma is primarily a childhood cancer, with an annual incidence of 300–350 new cases in the United States [4]. Most patients present before 16 years of age, with over 70% before 10, a third of which are younger than 3 years old; very few cases present under 1 year old [5][6][5,6]. The median age of diagnosis in children is about 5–7 years [7]. This age distribution highlights the current understanding of these tumors as remnants of aberrant embryonic cerebellar cells [8].
2. Characteristic and Presentation
Medulloblastoma typically arises within the posterior fossa in the cerebellum or its junction with the brainstem [9][13]. Recent studies have provided great insight into how the developmental biology of these tumors predicts their clinical behavior. For example, a recent lineage tracing study of the SHH subtype of medulloblastoma demonstrated that these tumors arise during the post-natal period from aberrantly persistent undifferentiated neural crest cells within the transient external germinal layer, which forms by embryonic migration of another transient structure, the rhombic lip. These cells ultimately become mature granule neurons within the internal granular cell layer of the cerebellum after the first year of life. These cells may not complete migration—establishing themselves anywhere along a path from the rhombic lip, which forms a critical interface between the cerebellum and brainstem in the embryo—into their proper position within the cerebellum. The tumor location critically affects the clinical course of these tumors in early childhood. A relationship between molecular pathogenesis, tumor location, and clinical behavior is seen not only in the SHH medulloblastoma subtype but also in the other medulloblastoma subtypes [10][14]. Typically, medulloblastoma arises within the medulla and expands the cerebellum to obstruct the fourth ventricle, creating signs of increased intracranial pressure such as major morning headaches, nausea, vomiting, and altered mental status. Compression of the adjacent brainstem structures and exiting cranial nerves may produce focal neurological deficits. For example, tumors within the cerebellar vermis and hemispheres cause gait ataxia and focal limb incoordination, respectively [11][15]. If left unchecked, tumor cells may disseminate through the cerebrospinal fluid (CSF) to the spinal canal. In rare instances, medulloblastoma may metastasize systemically to bone and bone marrow [12][13][16,17]. Tumors confined to the cerebellum have different symptoms than those metastasizing through the CSF and bloodstream.3. Diagnosis
Medulloblastoma should be suspected clinically in children presenting with signs and symptoms of a posterior fossa mass, such as those listed above. Diagnosis requires brain imaging. The most accurate imaging modality is magnetic resonance imaging (MRI). Medulloblastoma typically appears hypointense and hyperintense relative to grey matter on T1- and T2-weighted MRI, respectively. Intravenous contrast injection produces contrast enhancement throughout the tumor on MRI or CT [14][18]. The location of the tumor on imaging reflects the developmental pathogenesis described above. The mass usually originates in the inferior vermis, and enlarges to compress the fourth ventricle. Depending on the molecular subgroup, the tumor may involve the cerebellar hemispheres, the cerebellopontine angle, or it may mimic meningioma by originating in the tentorium [15][16][19,20]. Medulloblastoma may spread to the spinal canal, forming leptomeningeal “drop metastasis” on the nerve roots of the cauda equina. Medulloblastoma may also originate in extra-axial locations [17][18][19][20][21,22,23,24]. The various molecular and histopathological subtypes of medulloblastoma have distinguishing MRI features (Figure 1) [21][25]. Diffusion-weighted imaging is characteristic of medulloblastoma compared to other posterior fossa tumors [22][23][26,27]. While radiographic imaging can hone in on the correct diagnosis, confirmation of medulloblastoma is made on hematoxylin and eosin staining of histopathologic specimens obtained during surgical resection, which is part of the standard treatment regimen as outlined below. Molecular techniques further subtype the medulloblastoma [24][9]. Surgical resection improves prognosis, although near-total resection (NTR) does not increase recurrent risk compared to gross total resection (GTR). It is not recommended to achieve GTR over NTR at the cost of neurologic deficits [3][25][3,28].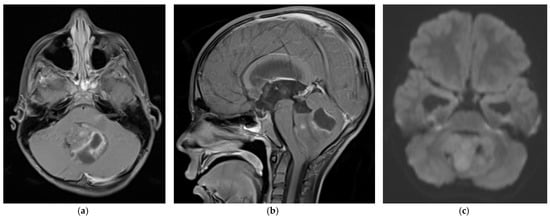
Figure 1. 5 year old boy with non-SHH/WNT medulloblastoma. Axial (a) and sagittal (b) T1-weighted MRI scans after intravenous contrast demonstrate a mass with cystic and solid components that enhances and extends into the fourth ventricle. The axial diffusion-weighted image (DWI) (c) shows restricted diffusion (higher signal intensity) within the tumor. The temporal horns of the lateral ventricles are distended, signifying obstructive hydrocephalus.
4. World Health Organization Classification and Grade
As discussed above, a panel of experts agreed at a conference held in Boston in 2010 to use molecular profiling to subdivide medulloblastoma into four different subtypes (WNT, SHH, Group 3, and Group 4) [9][13]. The molecular subtyping was separate from the 2016 WHO classification of medulloblastoma into four histologic subtypes: classic, desmoplastic/nodule, large cell/anaplastic, and medulloblastoma with extensive nodularity (MBEN). Most large cell/anaplastic medulloblastoma tumors belong to the SHH, Group 3, and Group 4 molecular subtypes, while the classic morphology was more typical of WNT tumors. Some SHH subtype tumors have desmoplastic/nodular morphology [26][27][29,30]. The updated 2021 World Health Organization (WHO) central nervous system tumor classification combined the four histologic subtypes into a single type, “Medulloblastoma, histologically defined.” The 2021 WHO classification further elaborated the medulloblastoma molecular subtypes: the SHH subgroup was divided into four groups, and the Group 3 and 4 subtypes (non-SHH, non-WNT) into eight groups [28][10]. These separations enabled more precise therapeutic targeting of the different medulloblastoma subtypes by conventional therapies and experimental therapies like gene therapy. As described below, each subtype group was defined by tumor genotyping, immunohistochemistry, and an individual prognosis.5. Molecular Subtyping
Molecular subtypes of medulloblastoma are characterized by unique molecular features and anatomic features, as described in Figure 2. Subgroup-specific treatments are summarized in Table 1.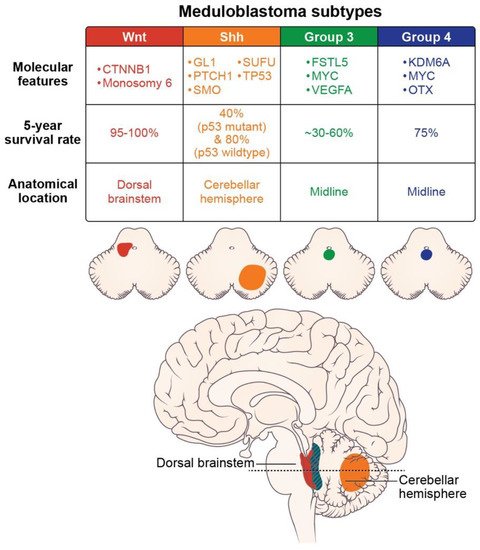
Table 1. Clinical trials and therapies in development for the four pediatric medulloblastoma subtypes.
| WNT Subtype | ||
| Clinical trial: Reducing doses of craniospinal radiation and chemotherapy | NCT01878617: A Clinical and Molecular Risk-Directed Therapy for Newly Diagnosed Medulloblastoma | |
| NCT02066220: International Society of Paediatric Oncology (SIOP) PNET 5 Medulloblastoma | ||
| NCT02724579: Reduced Craniospinal Radiation Therapy and Chemotherapy in Treating Younger Patients with Newly Diagnosed WNT-Driven Medulloblastoma | ||
| Proposed therapy: WNT antagonists | Phoenix, et al. (2016) [29] reported that WNT antagonists block the formation of a blood-brain barrier, and thereby promote chemotherapy penetration and high intratumoral drug concentrations. | Phoenix, et al. (2016) [31] reported that WNT antagonists block the formation of a blood-brain barrier, and thereby promote chemotherapy penetration and high intratumoral drug concentrations. |
| SHH Subtype | ||
| Proposed therapy: nanoparticles | Valcourt, et al. (2020) [30] and Caimano, et al. (2021) [31] reported their development of nanoparticles that encapsulate SMO or GLI inhibitors to improve drug delivery to this tumor subtype. | Valcourt, et al. (2020) [32] and Caimano, et al. (2021) [33] reported their development of nanoparticles that encapsulate SMO or GLI inhibitors to improve drug delivery to this tumor subtype. |
| Group 3 Subtype | ||
| Proposed therapy: Ribavirin | Huq, et al. (2021) [32] reported therapeutic potential for ribavirin to reduce medulloblastoma cell growth and prolong survival. | Huq, et al. (2021) [34] reported therapeutic potential for ribavirin to reduce medulloblastoma cell growth and prolong survival. |
| Proposed therapy: Anti-vascularization therapy | Thompson, et al. (2017) [33] reported increased vascularity in Group 3 tumors and proposed using anti-VEGFA anti-vascularization therapy to inhibit tumor growth. | Thompson, et al. (2017) [35] reported increased vascularity in Group 3 tumors and proposed using anti-VEGFA anti-vascularization therapy to inhibit tumor growth. |
| Group 4 Subtype | ||
| Proposed therapy: anti-ERBB4-SRC receptor tyrosine kinase | Forget, et al. (2018) [34] demonstrated that the combination of TP53 inactivation and aberrant signaling of the ERBB4-SRC receptor tyrosine may induce Group 4-like tumor growth. They suggested molecular therapies to inhibit these effects. | Forget, et al. (2018) [36] demonstrated that the combination of TP53 inactivation and aberrant signaling of the ERBB4-SRC receptor tyrosine may induce Group 4-like tumor growth. They suggested molecular therapies to inhibit these effects. |