1. Introduction
The American Cancer Society estimates that there will be 268,490 and 34,500 new cases of and deaths due to prostate cancer (PCa) in the United States (US) in 2022, respectively
[1]. Over the past two decades, PCa screening via serum prostate-specific antigen (PSA) led to substantial increases in detection of low-risk PCas (Gleason score ≤ 6), which pose little risk of either metastatic spread or death
[2][3][4][5][2,3,4,5]. Conversely, over-treatment is a well-documented consequence of over-detection of PCa, predominantly occurring among men with low-risk PCa who may be subject to multiple treatment-related morbidities with negligible or no benefit towards cancer-specific survival
[4][6][4,6]. Thus, the recommended guideline for the management of low-risk disease is active surveillance (AS). However, there are several identified challenges with AS, ranging from concerns with under-grading
[7][8][9][10][11][12][13][7,8,9,10,11,12,13], patient-related factors (e.g., anxiety, depression, doubts about the possible progression of disease), and higher decisional conflict regarding the selection of AS
[14][15][16][14,15,16], leading many to ultimately opt for a treatment that does not beneficially change tumor characteristics. On the other hand, men on AS are a highly motivated subgroup eager to make positive lifestyle changes to reduce their risk of PCa progression
[16][17][18][19][20][21][16,17,18,19,20,21], providing an optimal opportunity to intervene during this window with promising chemopreventive agents for PCa.
Previous strategies for PCa chemoprevention included 5-alpha-reductase inhibitors, finasteride, dutasteride
[22][23][24][22,23,24], trace element selenomethionine, and/or vitamin E. Collectively, these agents demonstrated greater risk for high grade disease
[25] or no reduction in risk of PCa progression in large phase III trials, severely limiting their clinical adoption
[23]. To date, there is minimal evidence available for the efficacy of any one agent or strategy for chemoprevention of PCa among men on AS. Therefore, the goal of our team for PCa chemoprevention is to utilize a systematic, broad-spectrum approach
[26] that involves an agent shown to (a) be bioavailable; (b) have an excellent safety profile; (c) produce robust targeting of multiple relevant molecular pathways; and (d) modulate measurable intermediate endpoint biomarkers correlated with early clinical progression of PCa—an approach that collectively may be more effective than agents evaluated to date. Our team and others have evaluated several approaches (i.e., diet interventions) and agents (selenium, vitamin E, isoflavones, lycopene n-3 fatty acids, and green tea catechins, or GTCs) targeting prostate carcinogenesis.
Human PCa is a complex heterogeneous disease. The central driving forces of prostate carcinogenesis include acquisitions of diverse sets of hallmark capabilities, aberrant functioning of androgen receptor signaling, deregulation of vital cell physiological processes, inactivation of tumor-suppressive activity, and disruption of prostate gland-specific cellular homeostasis. Thus, the molecular complexity and redundancy of oncoprotein signaling in PCa demands for concurrent inhibition of multiple hallmark-associated pathways
[27]. The ultimate goal for clinical cancer chemoprevention is to utilize a systematic, broad-spectrum approach that involves identifying and evaluating agents that can: (a) produce robust and concurrent inhibition of multiple hallmark-associated pathways in the target tissue/microenvironment; (b) address the underlying biology of carcinogenesis; and (c) enhance bioavailability and half-life with minimal toxicity in exceptionally high-risk populations
[26][28][26,28]. GTCs comprise (−)-epigallocatechin-3-gallate (EGCG), (−)-epicatechin, (−)-epigallocatechin (EGC), and (−)-epicatechin-3-gallate. Among the agents evaluated to date, EGCG in particular has been demonstrated to affect molecular pathways implicated in prostate carcinogenesis.
2. Green Tea CatechinCs: Promising Agent for Prostate CancerCa Chemoprevention
The most abundant constituents of green tea are the polyphenols, which are catechins that represent 30–40% of the dry weight of the tea leaves. The catechins in green tea belong to the flavon-3-ols of the polyphenol family
[29][34]. Laboratory studies have identified EGCG as the most potent modulator of molecular pathways thought to be relevant to prostate carcinogenesis
[30][31][32][33][35,36,37,38]. In the past two decades, research studies have shown that GTCs influence multiple biochemical and molecular cascades that inhibit several hallmarks of carcinogenesis relevant to prostate carcinogenesis. With an acceptable safety profile, GTCs are ideal candidates for PCa chemoprevention. Laboratory studies demonstrate that EGCG can affect several cancer-related proteins, including p27, Bcl-2 or Bcr-Abl oncoproteins, Bax, matrix metalloproteinases (MMP-2 and MMP-9), the androgen receptor (particularly important in PCa development and progression), epidermal growth factor receptor, activator protein 1, and some cell cycle regulators
[30][34][29,35]. Using cell culture systems, Adhami et al.
[35][39] were able to show that EGCG induces apoptosis, cyclin kinase inhibitor WAF-1/p21-mediated cell cycle-dysregulation, and cell growth inhibition. In cDNA microarrays, EGCG treatment of LNCaP cells induced genes that exhibit growth-inhibitory effects and repressed genes belonging to the G-protein signaling network
[36][40]. The ubiquitin/proteasome pathway plays a critical role in activation of the cellular apoptotic program and the regulation of apoptosis
[37][41]. Our work demonstrated that GTC specifically inhibits the chymotrypsin-like activity of the proteasome in several tumor and transformed cell lines, including prostate cell lines, resulting in the accumulation of two natural proteasome substrates–p27 (Kip1) and nuclear factor kappa B (NF-ĸB) inhibitor alpha, which inhibit transcription factor NF-ĸB, leading to growth arrest in the G(1) phase of the cell cycle. Synthetic analogs of EGCG were observed to be more potent as proteasome inhibitors compared to EGCG. Polyphenon E
® (Poly E) and Sunphenon
® 90D are standardized formulations of green tea containing 50% of the catechins from EGCG.
SearchersWe observed that Poly E
® (>50% EGCG, 80% total catechins) preferentially inhibits the proteasomal chymotrypsin-like activities over other activities, with an IC50 value of 0.88 µM
[37][38][39][40][41,42,43,44]. Standardized GTC formulations of Poly E
® and Sunphenon
® 90D in equal concentrations were evaluated in vitro. Pre-treatment with Sunphenon
® 90D downregulated NF-ĸB in H
2O
2-treated C2C12 cells, while activating caspase-3 (
Figure 1)
[41][45]. Incubation of human primary osteoblasts with Sunphenon
® 90D significantly reduced oxidative stress and improved cell viability
[42][46]. EGCG has been shown to have both anti-inflammatory properties, such as through the influence of T-cell proliferation and inhibition of NF-ĸB, and neuroprotective properties by acting as a free radical scavenger
[43][44][47,48]. More specifically, EGCG’s antioxidant properties deplete reactive oxygen species, thus preventing DNA damage and inhibiting NF-ĸB-induced inflammation, angiogenesis, and cell survival that could otherwise propel cancer development and progression
[45][49]. In summary,
rwe
searchers and others have reported convincing evidence suggesting that GTCs inhibit proliferation and cell cycle events and induce apoptosis through multiple mechanisms.
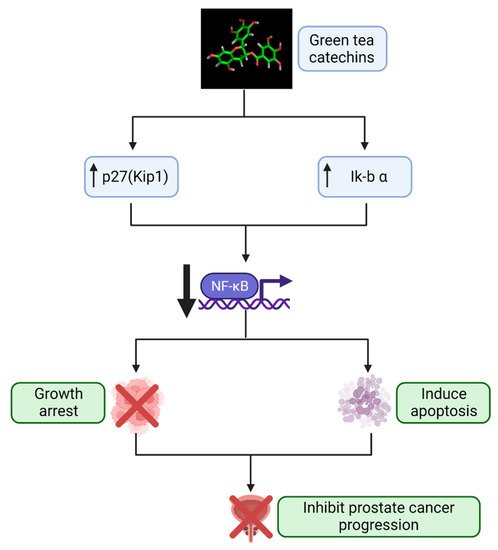
Figure 1. Mechanistic pathway by which GTCs prevent PCa progression. In vitro studies
[37][38][39][40][41,42,43,44] demonstrate that GTCs block proteasomal activity in PCa cells, leading to build-up of proteasomal substrates Kip1 and Ik-b α that subsequently downregulate the activity of NF-κB. This inhibits the cell cycle and elicits apoptosis in these PCa cells. GTCs, green tea catechins; Ik-b α, NF-κB inhibitor alpha; NF-κB, nuclear factor kappa B; PCa, prostate cancer. Created with Biorender.com (accessed on 1 July 2022).
The association of green tea intake with PCa risk has been investigated in several epidemiological studies. In a meta-analysis of 9 case-control studies, there was a statistically significant 57% lower risk of PCa, comparing subjects with the highest relative to lowest green tea consumption, whereas there was a null association in a meta-analysis of 4 cohort studies
[46][50]. Similar results were observed in a more recent meta-analysis of 3 case-control and 4 cohort studies: no statistically significant associations were observed across cohort studies, while a statistically significant 55% lower odds of PCa was observed for highest versus lowest green tea intake in the case-control studies
[47][51]. This inconsistency could be due, in part, to differences in study design, residual confounding factors such as by diet/lifestyle and biological factors, and varying formulations and subtypes of green tea studied. These studies were mostly limited to men in Asian countries, where approximately 20% of green tea is consumed globally and where mortality from PCa is the lowest compared to Western populations
[31][36], where green tea consumption is a more recent phenomenon. Asian men who migrate to the US have a relatively increased risk of PCa compared to their counterparts in their countries of origin, potentially as a result of acculturation and adoption of Western diets
[33][38]. Although the above study findings have been mixed—potentially due to confounding by variation in geographical location, tobacco and alcohol use, and other lifestyle factors (mainly diets)
[32][48][37,52]—taken together, studies among Asian populations demonstrate a protective effect of GTCs as related to PCa
[32][33][49][37,38,53]. Another highly plausible confounder of GTC-PCa associations is the gut microbiome, which has increasingly been implicated in the modulation of carcinogenesis. The gut microbiome comprises densely populated commensal and symbiotic microbes
[50][54] whose composition is highly influenced by the host’s dietary intake. The gut microbiome also produces metabolically active metabolites that interact with host-signaling pathways and gene expression, impacting cancer initiation and progression
[51][52][55,56]. Multiple studies have observed differences in the gut microbiome between various racial and ethnic groups, even amongst those living in the same community. These differences are potentially attributed to lifestyle, dietary, social, and other uncharacterized exposures that result in variations across racial and ethnic groups
[53][54][57,58]. Using fecal shotgun metagenomic data analyzed amongst 106 Japanese individuals compared with those of 11 other nations, the composition of the Japanese gut microbiome was more abundant in the phylum Actinobacteria, in particular, genus
Bifidobacterium, compared to others
[55][59]. In line with increased PCa rates in Asian populations living in the US, studies have shown that the gut microbiome of Southeast Asian immigrants changes after migration to the US
[56][60], potentially indicative of an incompatibility between the incorporation of Western lifestyles with the traditionally harbored microbiome of this population
[57][61]. These studies have provided the basis for understanding that the gut microbiome can act as an important mediating factor in investigations of diet and lifestyle differences that potentially promote cancer risk.
3. The Gut Microbiome, Prostate Cancer, and Green Tea CatechinTCs
Predictive biomarkers of responses to secondary chemoprevention are presently lacking. Identification of biomarkers, such as the gut microbiome, predictive of favorable clinical responses to secondary chemoprevention has the potential to substantially facilitate clinical decision-making. Numerous studies found that the gut microbiome directly effects drug metabolism, efficacy, and toxicity, potentially affecting disease development and progression
[58][91]. For example, in oncology, there exists convincing evidence to support that the antitumor effects of immunotherapies can be enhanced or inhibited by the gut microbiome
[59][60][92,93].
The gut microbiome likely has critical roles in regulating the bioavailability of GTCs and absorption of bioactive phenolic GTC metabolites, as demonstrated in laboratory and pre-clinical models (
Figure 2). Although dietary polyphenols are absorbed by the small intestine, accumulating evidence suggests that they are metabolized to a greater extent in the colon by bacterial enzymes
[61][62][94,95]. EGCG is hydrolyzed by bacteria to gallic acid or EGC and further converted to multiple metabolites, such as 5-(3,5-dihydroxyphenyl)-4-hydroxyvaleric acid and 5-(3′,5′-dihydroxyphenyl)-g-valerolactone
[62][95]. These metabolites are then either taken up via the portal vein and transported to the liver or excreted in the feces.
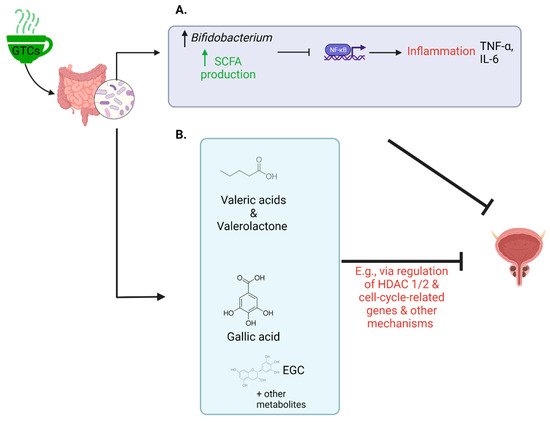
Figure 2. Examples of chemopreventive effects of GTCs in the context of PCa via gut microbiome modulation. (
A) GTCs like EGCG have been evidenced to alter microbial composition, such as increasing abundance of Bifidobacterium
[62][95]. This genus, for example, is known to increase production of SCFAs
[62][63][95,96] which inhibit inflammatory pathways initiated by NF-κB that would otherwise propel carcinogenesis
[64][97]. (
B) The gut microbiome can enzymatically alter GTCs like EGCG to produce metabolites including gallic acid, EGC, valeric acid, and valerolactone, that subsequently travel to the bloodstream to exert potential chemopreventive benefits (e.g., regulating HDAC 1 and 2 and suppressing cell-cycle-related genes)
[62][65][66][67][95,98,99,100]. EGC, epigallocatechin; EGCG, epigallocatechin gallate; GTCs, green tea catechins; HDAC, histone deacetylase; IL-6, interleukin-6; NF-κB, nuclear factor kappa B; SCFA, short chain fatty acid; TNF-α, tumor necrosis factor alpha. Created with Biorender.com (accessed on 1 July 2022).
On the other hand, several pharmacologic agents, including GTCs, were shown to influence gut microbiome composition and function. For example, in a study of 10 volunteers who drank 1000 mL of green tea daily for 10 days, Bifidobacteria abundance was increased
[68][101]. In multiple animal studies, green tea polyphenols had similar effects on Bifidobacteria and other effects, including decreasing the Firmicutes/Bacteroidetes ratio
[69][70][102,103]. In turn, gut microbiome composition and function may directly and indirectly influence PCa progression, such as through production of metabolically active metabolites or regulation of hormones and inflammation, as described below
[71][72][73][104,105,106]. Given the substantial preliminary evidence for interrelationships among GTCs, the gut microbiome, and prostate carcinogenesis, it is highly likely that the gut microbiome may mediate etiological effects of GTCs, including effects on PCa progression and development of adverse events; however, little is known regarding these interrelationships among humans.
The gut microbiome has biologically plausible roles in PCa such as via its influence on hormone and inflammation regulation and production of metabolically active metabolites
[71][72][73][104,105,106]. For example, gut microbes produce sex hormones, such as androgen, and, in a study by Pernigoni et al., multiple species among mice and humans produced androgens from androgen precursors, in turn promoting progression of castrate resistant PCa
[74][107]. In a study of both mice and PCa patients, Proteobacteria was increased after antibiotic exposure, and was in turn associated with development of PCa in mice and with metastasis of PCa among humans
[75][108]. In a study of mice on a high-fat diet, the resultant alterations to the mice fecal microbiome promoted histamine biosynthesis and increased inflammatory cancer cell growth
[76][109]. Previous human studies of the gut microbiome and PCa included a case-control study comparing 16S rRNA sequenced fecal bacteria among 64 men with PCa and 41 without PCa, finding differences in beta diversity, higher abundances of Bacteroides and Streptococcus species, and differences in folate and arginine pathways
[77][110]. Another case-control study compared the gut metagenome among 8 men with benign prostatic conditions and 12 men with intermediate or high risk clinically localized PCa, finding higher relative abundance of Bacteriodes massiliensis and lower relative abundances of Faecalibacterium prausnitzii and Eubacterium rectalie amongst men with intermediate/high-risk PCa
[78][111]. In a comparison of men with and without prostate enlargement, the ratio of Firmicutes to Bacteroidetes was higher among men with enlarged prostates, potentially related to prostate inflammation
[79][112]. Finally, evidence supports the study of the gut microbiome across the disease continuum of PCa, with evidence demonstrating that the gut microbiome may be modified by PCa treatment, including androgen deprivation therapy, among more advanced PCa patients
[80][113].