Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by YUANZHE LI and Version 2 by Camila Xu.
Self-healing polymers are categorized as smart materials that are capable of surface protection and prevention of structural failure. Polyurethane/polyurea, as one of the representative coatings, has also attracted attention for industrial applications.
- polyurea coating
- self-healing
- self-healing mechanism
- formulation optimization
1. Introduction
Many times, structures that require protection are in poorly accessible areas, which makes maintenance work difficult. As an industrial class of smart materials, self-healing polymers are distinguished by the fact that they can repair themselves without detection or manual intervention [1]. The concept of self-healing in polymers was introduced in the 1980s [2]. Interest in the self-healing of polymers grew when significant research progress was made by Sottos [3] in 1993 and White et al. [4] in 2001. Eventually, the European Space Agency [5] and the US Air Force [6] saw the advantages and made investments for further advances in self-healing polymers. In 2007, the first international conference on self-healing materials was held [7][8][7,8]. In recent years, studies have been conducted to equip self-healing polyurethane and polyurea with adequate mechanical properties by changing the bonds present in the polymers. The goal is to achieve an optimal balance between self-healing efficiency and mechanical properties. Lee [9] added azomethine groups to polyurethane and obtained a self-healing efficiency of 86% and a tensile strength of 50 MPa. Qian [10] introduced alkyl diselenide to polyurethane and managed to recover 100% of the polymer’s initial mechanical properties [11]. Without the need for detection or manual intervention, this can ensure that protective coatings are capable of providing continuous protection against corrosion for a prolonged time, even in the absence of short-windowed routine checks. This can also reduce the high cost of corrosion and maintenance work in poorly accessible areas. With such benefits provided by self-healing polymers, it is anticipated that the self-healing market will continue to expand significantly until at least 2025 [12].
Both polyurea and polyurethane are commonly found in coatings that protect against moisture, corrosion, abrasion, and chemicals. However, there are some differences between polyurea and polyurethane that make one a better choice over the other in different applications. Polyurea is the product of the reaction between polyamine and isocyanate (R-NCO + R’-NH2 → R-NH-CO–NH–R’), while polyurethane is the product of the reaction between polyol, isocyanate, and a catalyst (R-NCO + H2O → R-NH2 + CO2 & R-NCO + R’-NH2 → R-NH-CO–NH–R) [3][12][3,12]. Comparing polyurethane and polyurea, polyurea has higher tensile strength and a shorter curing time. Despite these superior properties, research in recent years has mainly focused only on the self-healing of polyurethane. Lee [9] and Hu et al. [13] used azomethine diols to achieve self-healing polyurethane elastomers with tensile strengths of at least 40 MPa. Li et al. [14] and Wang et al. [15] incorporated the Diels–Alder structure to achieve self-healing polyurethane with up to 95% healing efficiency [16]. Only limited work conducted is related to the self-healing of polyurea, and the frequency of conducting maintenance work can be greatly reduced, which makes it more capable of protecting existing structures against weathering effects [17][18][17,18] and corrosion [19]. Polyurea coatings are also known to have good corrosion resistance against seawater [20] and are capable of providing both underwater and on-land blast resistance [21] to underlying structures.
There are also varieties of formulation possibilities, incorporated with various additives, to achieve the desired performance. Much like that for polyurethane chemistry, these formulation possibilities are made possible by the selection of different types of raw materials. Thus, the selection of appropriate raw materials for the polyurea coating system can be a very complex procedure. The formulation consists of two main components (Part A: isocyanate component, reactive diluent; Part B: polyether amines, chain extenders, and additives and pigments). The most commonly used Part A components are toluene-2,4-diisocyanate (TDI) and diphenylmethane diisocyanate (MDI). TDI prepolymers with NCO content of 45 wt.% to 55 wt.% or MDI prepolymers with NCO content of 14 wt.% to 17 wt.% are preferred for standard preparations of polyurea spray coatings. In contrast, Part B, which is also named Part R, the resin blend component or polyether part, is normally a mixture of amine-terminated ethylene oxide and/or propylene oxide polyether with molecular weights varying from 200 to 5000 g/mole. Polyether amines are mainly used to increase flexibility, toughness, hydrophilicity, or hydrophobicity, and they also offer various reactivities, good thermal stabilities, colorlessness, and low viscosity.
2. Self-Healing Mechanisms of Polyurea
Figure 1 shows the performance of original material and self-healing material over time. Performance is defined as the original property of the material, be it tensile strength, hardness, or corrosion resistance. Service lifetime is defined as the period of time in which the material is above its limit of reliability and in working condition before it needs to be replaced. Curve (a) represents original material with a decrease in performance over time and a limited-service lifetime. Curve (b) represents traditionally improved material with a slight extension of the service lifetime. Curve (c) represents self-healing material. When there is damage inflicted on the material, its performance drops. After healing, the performance increases again and decreases due to wear over time. Once there is more damage, the cycle repeats. Due to the ability to enhance performance after healing, self-healing material is able to extend the service lifetime to a greater extent.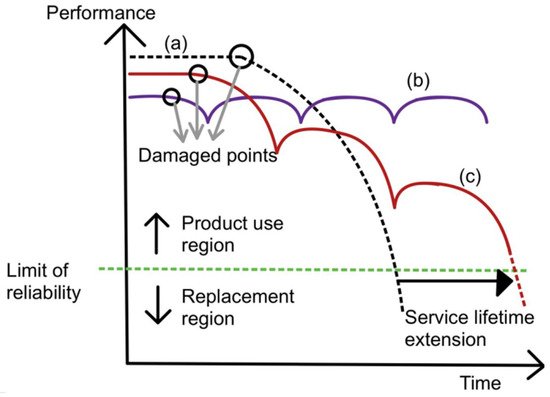
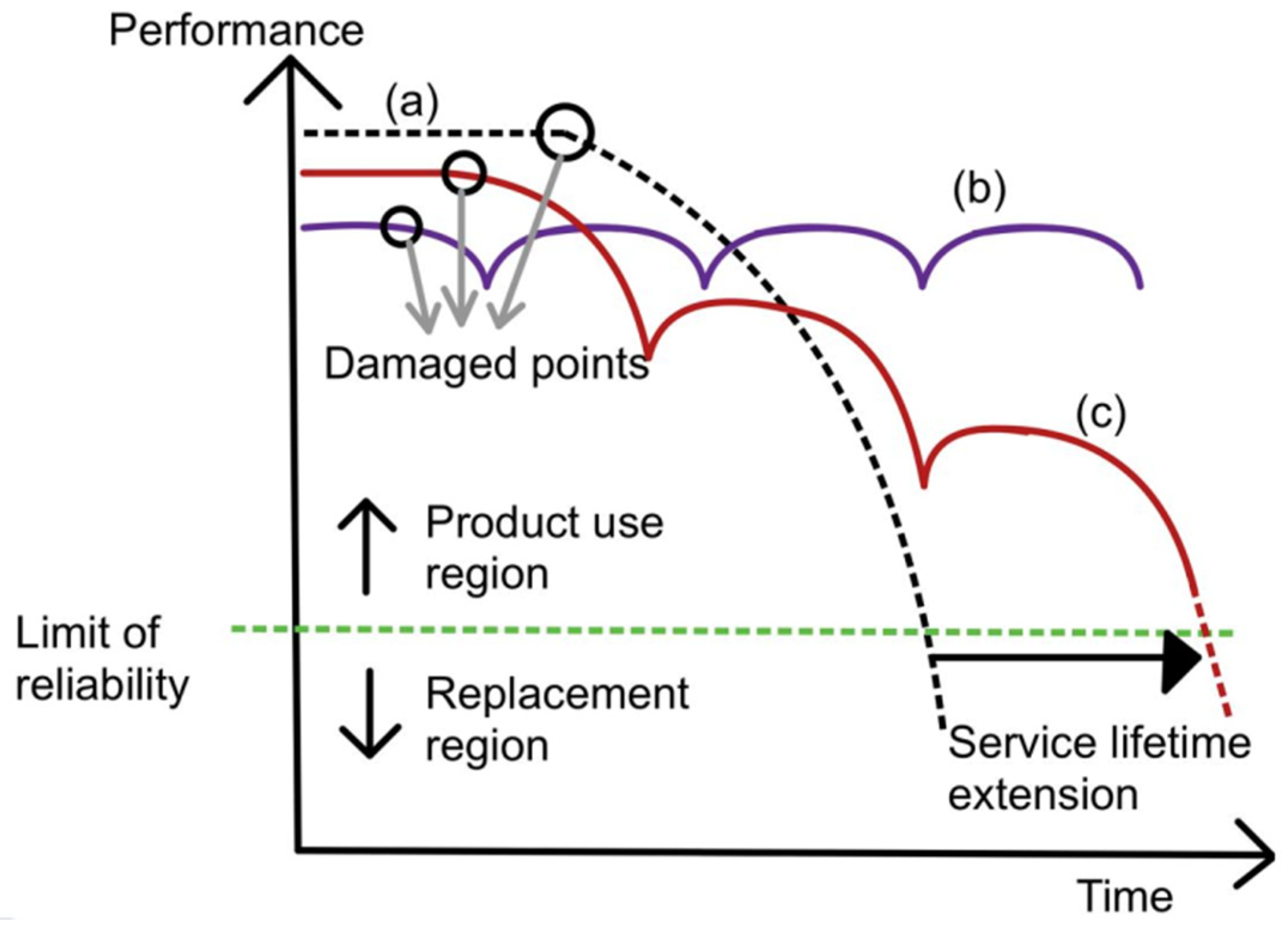
Figure 1. Graph of performance plotted against time for curve (a) (normal material), curve (b) (ideal self-healing material), and curve (c) (self-healing material) [22].
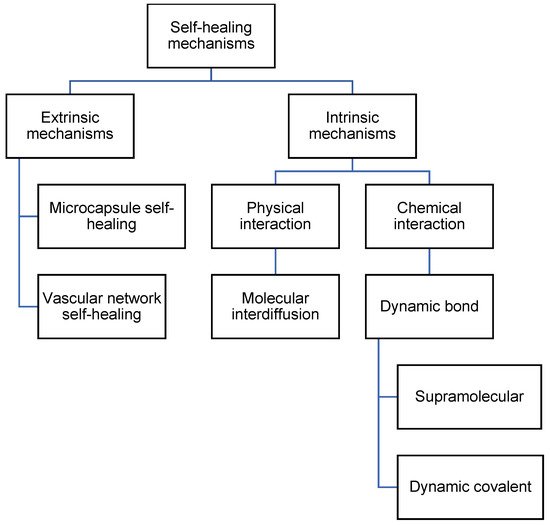
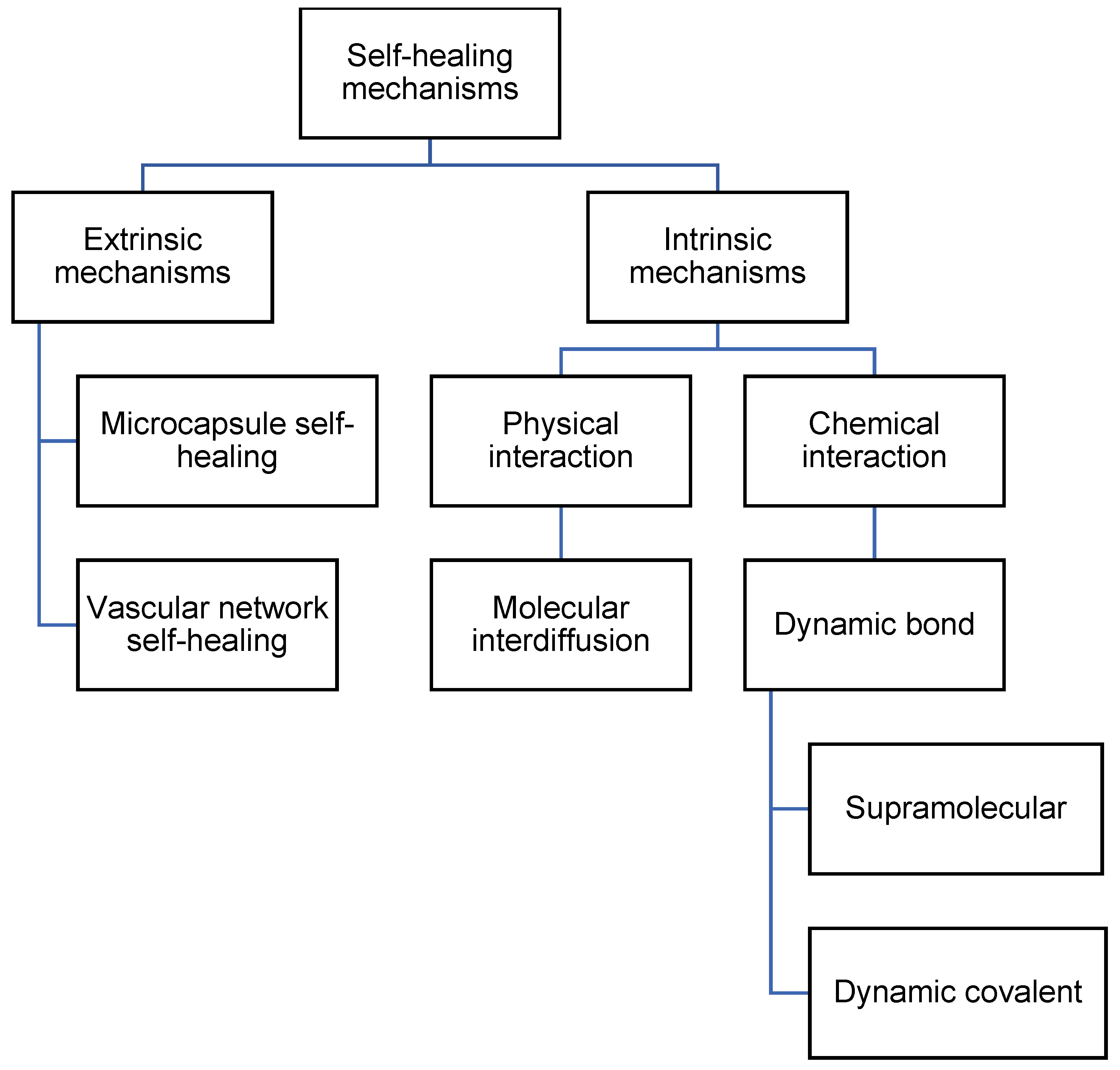
Figure 2. Flowchart listing the types of self-healing mechanisms in polyurea.
Flowchart listing the types of self-healing mechanisms in polyurea.
2.1. Extrinsic Mechanisms
Extrinsic mechanisms are defined as self-healing processes that make use of different types of containers holding prefilled healing agents that are then embedded in the matrix. Extrinsic mechanisms include microcapsule self-healing and vascular network self-healing.2.1.1. Microcapsule Self-Healing
The microcapsule self-healing approach involves the use of healing agents that are encapsulated in capsules to heal cracks in the material. White et al. [4] prepared urea–formaldehyde microcapsules with sizes of 50–200 micrometers that are filled with dicyclopentadiene (DCPD). These DCPD-filled microcapsules are then embedded in the matrix together with Grubb’s catalyst. During service time, cracks form in the matrix. As the cracks propagate, the microcapsules rupture and release their contents. The DCPC flows out of the capsules onto the matrix. Eventually, when DCPD interacts with Grubb’s catalyst, polymerization takes place and fills the crack. Hence, self-healing occurs. This process is illustrated in Figure 3.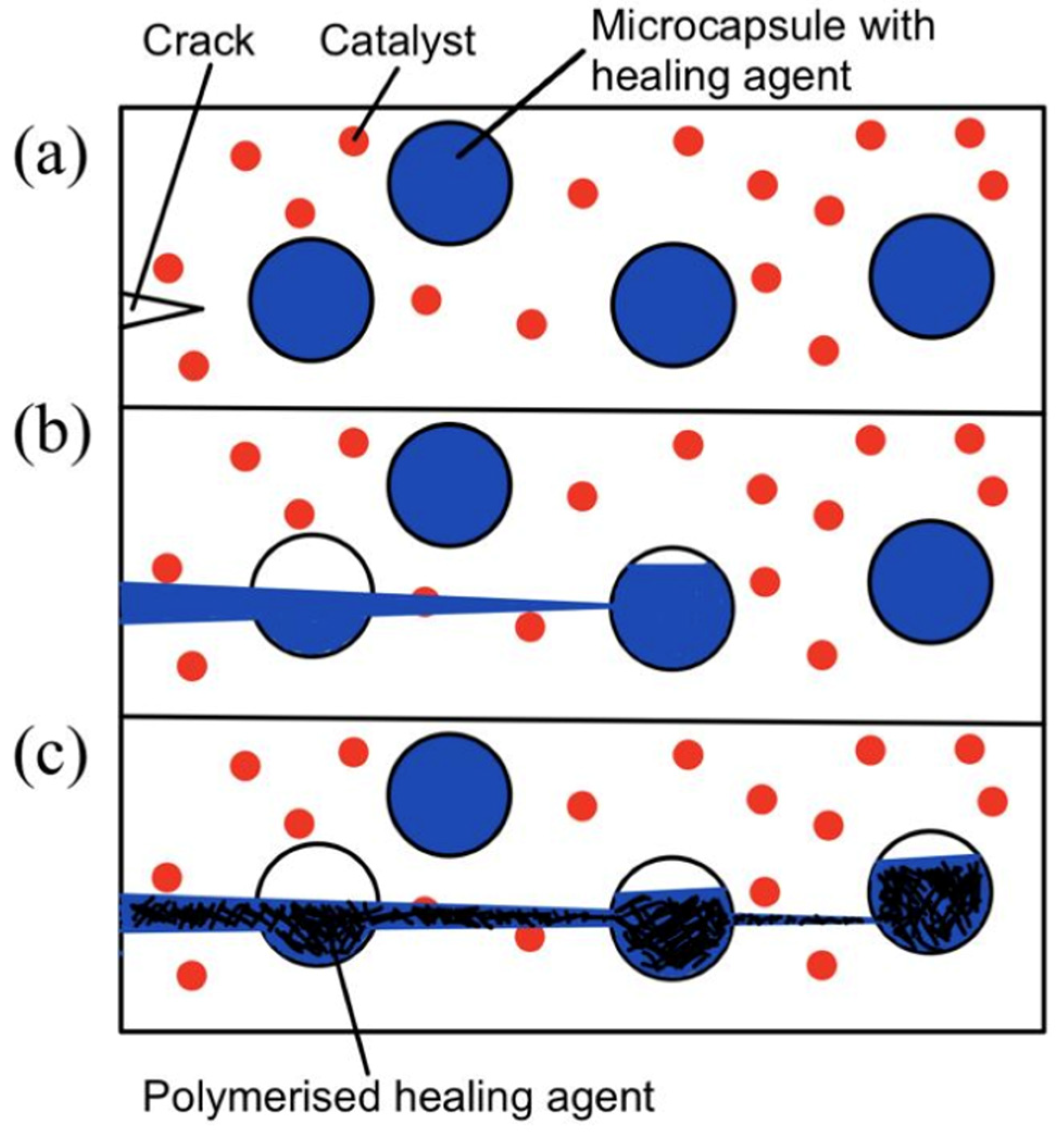
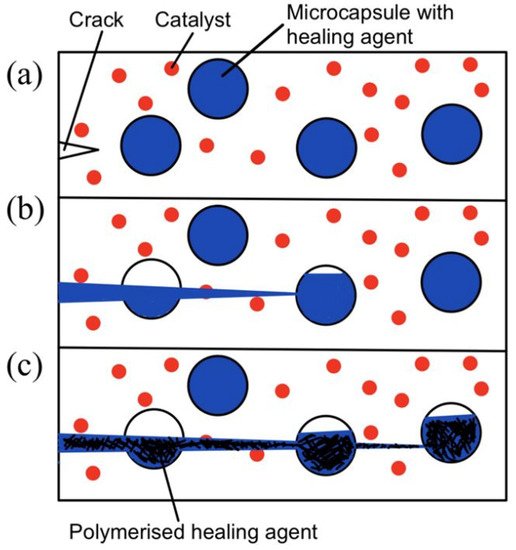
Figure 3. (a) Crack nucleation occurs in the matrix, (b) crack propagation takes place and ruptures microcapsules, and (c) microcapsules’ contents flow out and polymerize upon contact with the catalyst [4].
2.1.2. Vascular Network Self-Healing
Unlike the microcapsule self-healing approach, the healing agents in a vascular network self-healing system are not stored in capsules. The healing agents in a biomimetic vascular network [38] are stored in microchannels that resemble blood vessels in the human body. This vascular network self-healing approach was first demonstrated by C. Dry [23][24][23,24]. The basic working principle behind vascular network self-healing is illustrated in Figure 4.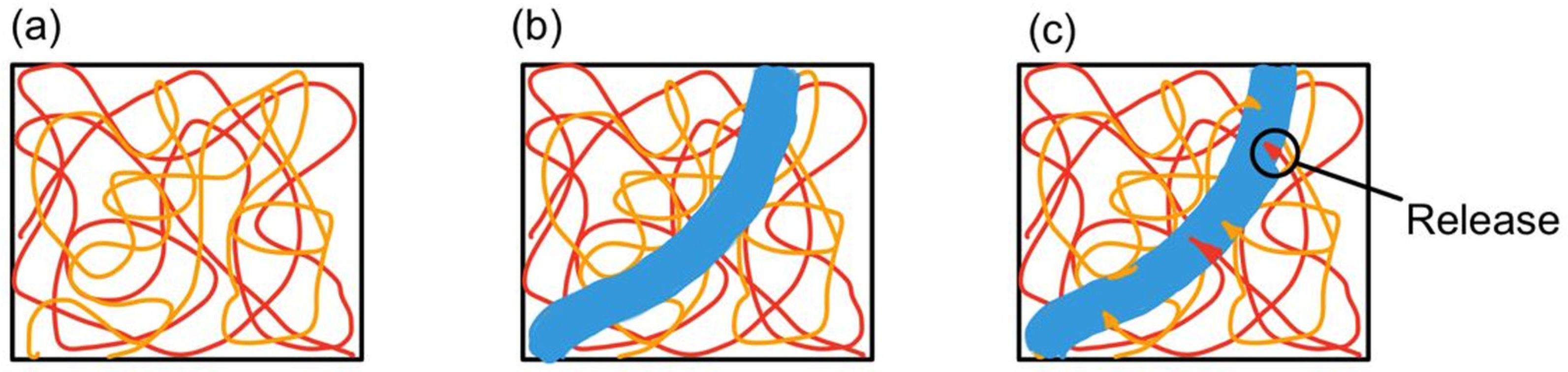
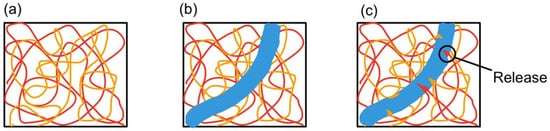
Figure 4. (a) Vascular network embedded in polymer composite matrix, (b) a cut is made (blue region), and (c) monomers from microchannel leak into the matrix [39].
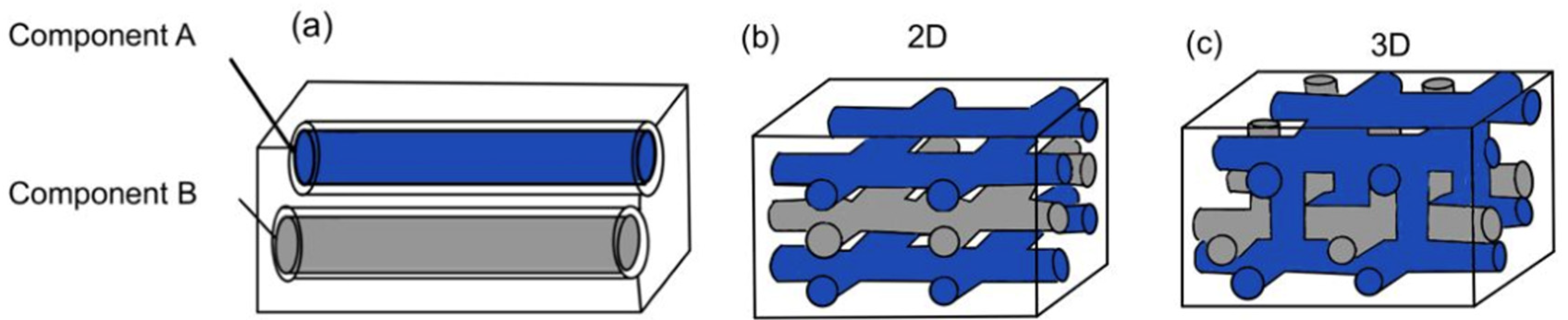
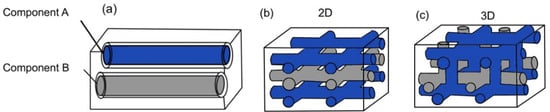
Figure 5. (a) One-dimensional vascular network system, (b) two-dimensional vascular network system, and (c) three-dimensional vascular network system [28].
2.2. Intrinsic Mechanisms
Intrinsic mechanisms are defined as self-healing processes that take place without the need for a healing agent or catalyst. These mechanisms are based on the inherent reversibility of the chemical bonds present in the polymeric matrix, which can be rearranged [28][39][28,39]. Intrinsic mechanisms are further divided into physical interaction and chemical interaction. With physical interaction, there is molecular interdiffusion. With chemical interaction, there is dynamic bonding.2.2.1. Physical Interaction
The phenomenon of molecular interdiffusion was first discovered when two pieces of the same polymer were brought together at temperatures above their glass transition temperatures [44]. The interfaces between the two pieces disappear, and the mechanical strength at the interface increases [44][45][44,45]. As a result, extensive research was conducted around the 1980s [25][46][47][25,46,47]. In particular, the Wool and O’Connor model [25] to explain the process of crack healing was more widespread. In the 1990s, research in this area slowed down [44]. The crack-healing process consists of five stages, as summarized in Table 1.| Stages | Definition |
|---|

Figure 6.
(
a
) Cleavage and recombination of disulfide bond; (
b) 3 steps in disulfide exchange mechanism.
) 3 steps in disulfide exchange mechanism.
2.3. Comparison between Extrinsic and Intrinsic Mechanisms
A brief summary and challenges faced when using extrinsic and intrinsic mechanisms are listed in Table 2.| Advantages | Disadvantages | |||||
|---|---|---|---|---|---|---|
| 1. Surface rearrangement | The roughness or topography of the surface changes with external factors (pressure, time, and temperature). | |||||
| Microcapsules (Extrinsic) |
|
| ||||
| 2. Surface approach | Healing can only occur when surfaces are brought together, or a gap is filled with healing fluid. | |||||
| Vascular network (Extrinsic) | 3. Wetting | Surfaces have to wet each other and form an interface before healing can occur. | ||||
| 4. Diffusion | The most critical stage of strength development. | |||||
| 5. Randomization | Refers to the equilibration of the non-equilibrium conformations of chains near the surfaces. |
2.2.2. Chemical Interaction
Dynamic bonds refer to any type of bonds capable of undergoing repetitive breaking and reformation at an equilibrium rate [52]. Dynamic bonds can be further split into supramolecular and dynamic covalent self-healing. Supramolecular self-healing can take place at equilibrium, while dynamic covalent self-healing requires an additional intervention, such as heat or UV [28].- (a)
-
Supramolecular
- (b)
-
Dynamic Covalent
 Generally, microcapsules (extrinsic) face the limitation of being single-use. The vascular network (extrinsic) faces the potential blockage of core fibers due to its network, which compromises its healing properties. On the other hand, dynamic bonds (intrinsic) are capable of infinite healing cycles. This researchtudy aims to find the optimum formulation of self-healing polyurea that is capable of healing even after multiple cuts. This is to meet the practical needs of industrial uses. Hence, this research study focuses on intrinsic self-healing mechanisms.
Generally, microcapsules (extrinsic) face the limitation of being single-use. The vascular network (extrinsic) faces the potential blockage of core fibers due to its network, which compromises its healing properties. On the other hand, dynamic bonds (intrinsic) are capable of infinite healing cycles. This researchtudy aims to find the optimum formulation of self-healing polyurea that is capable of healing even after multiple cuts. This is to meet the practical needs of industrial uses. Hence, this research study focuses on intrinsic self-healing mechanisms.- Multiple healing cycles
- Healing agents evenly distributed
-
Blockage of core fiber during filling and releasing of healing fluid
-
Matrix carrying healing fluid reduces composite strength
Dynamic bonds
(Intrinsic)-
Do not require any catalyst or healing agent
-
Heal for infinite cycles
-
External stimuli to trigger healing