Nitrogen oxides (NOx) are gaseous pollutants contributing to pollution in their primary form and are also involved in reactions forming ground-level ozone and fine particulate matter. Thus, NOx is of great interest for targeted pollution reduction because of this cascade effect. To achieve a holistic understanding of the correlation between NOx and human health, both the physical and mental health implications must be accounted for. This re following contentview is intended to be illustrative in nature, and not exhaustive of all research conducted in the field.
- air pollution
- air quality
- mental health
- nitrogen oxides
- NOx
- physical health
1. Nitrogen Oxides (NOx) as a Targeted Pollutant
2. Physical Health Impacts of NOx
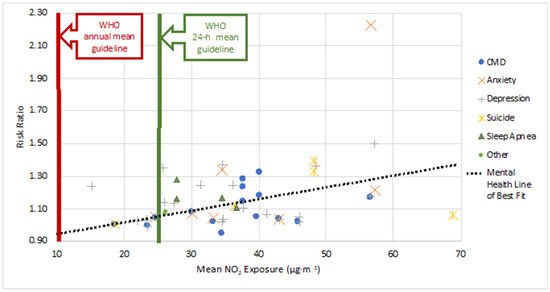
3. Mental Health Impacts of NOx
| Category | Symptom | Exposure Duration | Risk Ratio (95% CI) per 10 μg·m−3 Increase in NO2 (Unless Otherwise Specified) *-Calculated from OR |
Mean NO2 Exposureug μg·m−3 | Reference | ||||
|---|---|---|---|---|---|---|---|---|---|
| Common Mental Disorders (CMD) |
CMD | Chronic | 1.35 (1.26, 1.35)* for NO2 1.23 (1.19, 1.27)* for NOx |
[65][81] | |||||
| High Blood Pressure | |||||||||
| CMD | Chronic | 1.01 | Chronic | 1.28 (1.05, 1.46)* for NO2 1.27 (1.04, 1.45)* for NOx[20][42] |
|||||
| 35.8–39.6 (NO | 2 | ) | 57.0–67.4 (NOx) |
[66][13] | Headache | Chronic | 1.13 | [20 | |
| Physical Symptoms | Chronic | 1.23 (1.02, 1.39)* for NO2 | ][42] | ||||||
| 1.22 (1.02, 1.38)* for NO | x | Stroke | Chronic | 1.01 | [20][42] | ||||
| Self-Rated Health | Chronic | 1.15 (0.94, 1.32)* for NO2 1.13 (0.93, 1.30)* for NOx |
Nose and Throat Irritation | Acute | |||||
| Chronic | [ | 1 | ][4] | ||||||
| 1.07 (1.05, 1.10)* per IQR | 23.4 | [ | 67][82] | Increased sensitivity and susceptibility to respiratory illness and disease | Chronic | [1][3][8][18][19][21][4,7,17, | |||
| Chronic | 40 | , | 0.95 (0.39, 1.31)* highest vs. lowest tertile range41,43] | ||||||
| 34.64 | [ | 68 | ][83] | Respiratory Illness | Chronic | [17][39] | |||
| Psychological Distress | Chronic | Positive, statistically significant relationship with NOx | [69][84] | Chest Colds, Chronic Cough and Wheezing, Chest Cough | Acute and Chronic | [8][15][17][22][23][24][7,11 | |||
| Mental Health Service Use | Chronic | 1.32 (1.25, 1.38) per IQR for NO2 1.31 (1.24, 1.37) per IQR for NOx | ,37,39,44,45] | ||||||
| 40.2 (NO | 2 | ) | 71.1 (NOx) |
[70][85] | Dyspnea | Chronic | [1][4] | ||
| Reduced Lung Function | Acute and Chronic | [8][15][18][7[,3723,40],44] | |||||||
| Bronchitis and Bronchitis Symptoms | Chronic | 1.021 | [1][2][17][18]28][4,16,39,40[25][26][,4627,47],48[,49] | ||||||
| Allergic Reactions | Chronic | [1][8][19][4,7,41] | |||||||
| Inflammatory Responses | Chronic | [2][13]16[14][15][16][17],35[,3622,37][,3826][11,,39,47] | |||||||
| 1.0494 (1.0203, 1.0792) per IQR | 39.8 | [ | 74][89] | Potential Reproductive Impacts | Chronic | [1][8][19][4,7,41] | |||
| Acute | 1.0377 (1.0278, 1.0478) | 32.79–53.23 | [75][90] | Cell Damage | Chronic | [2][13][14][15][16][17][22][26][11,16,35,36,37,38,39,47] | |||
| Cardiovascular Disease (CVD) | |||||||||
| Acute | 0.9966 (0.9873, 1.0061) per IQR | 23.57 | [76][91] | Chronic | 1.04–1.22 | [1][3][8][31][32][33] | |||
| Acute | [ | 4 | ,719],17[21],41[29],43[30],50[,51,52,53,54] | ||||||
| 1.0445 (1.0290, 1.0604) | 24.69 | [ | 77][92 | Respiratory Disease | Chronic | [1][2][3][8][19][4,7,16,17,41] | |||
| ] | |||||||||
| Acute | 1.0794 (1.0628, 1.0962) | 30.13 | [77][92] | Asthma | Chronic | 1.05–1.5 | [1][8][19][20][22[4],7[,11,4124,42][34][35],45[,5536,56],57] | ||
| Acute | 1.0219 (0.0051, 1.0389) | 33.35 | [77][92] | Hospital Admissions | General | Acute and Chronic | 1.01 | [25][27][28][37][38][46,48,49,58,59] | |
| Psychosis Mortality | Acute | 1.0010 (0.9999, 1.0021) | 18.7 | [78][93] | Emergency Room | Chronic | 1.1 | [3][39][17,60] | |
| Sleep | Low Sleep Efficiency | Chronic | 1.16 (1.07, 1.25)* | 27.82 | [79][94] | Stroke | Chronic | 1.14 | |
| Sleep Apnea | [ | 40 | ][61] | ||||||
| Chronic | 1.28 (1.03, 1.47)* | 27.82 | [ | 79][94] | Asthma | Acute and Chronic | 1.001–1.27 | [13][38][40][35,59,61] | |
| Sleep Disorder | Chronic | 1.11 (1.02, 1.19)* per IQR | 36.78 | [80][95] | Respiratory Ailments | Chronic | 1.009–1.05 | [38][40][41][42][9,59,61,62] | |
| Sleep Disorder | Chronic | 1.17 (0.77, 1.44)* highest vs. lowest tertile range | 34.64 | [68][83] | Respiratory Disease | Acute | 1.018 | [25][28][46,49] | |
| Anxiety | Anxiety Disorder | Chronic | 1.09 (0.90, 1.25)* | 27.5 | [21][43] | Chronic Obstructive Pulmonary Disease (COPD) | Acute | ||
| Chronic | [ | 13 | ][35] | ||||||
| 1.34 (0.85, 1.62)* highest vs. lowest tertile range | 34.64 | [ | 68][83] | Blood Poisoning | Acute | ||||
| Medication Use | Chronic | 1.21 (0.90, 1.44)* for NO2 1.13 (0.89, 1.32)* for NO[13][35] |
|||||||
| Cardiovascular-Circulatory System Disease | Chronic | 1.05 | [40][61] | ||||||
| Cardiovascular-Myocardial Infraction | Chronic | 1.15 | [40][61] | ||||||
| Cancer-Lung | Chronic | 1.2 | [40][61] | ||||||
| x | 57.3 | [34][44][49][55,63,68] | |||||||
| Prostate | Chronic | [44][63] | |||||||
| Premature Mortality | All-Cause | Acute | 1.003–1.016 | [19][28][50][41,49,69] | |||||
| All-Cause | Chronic | 1.003–1.06 | [2][3]]55][16[ | ||||||
| Hospital Admissions | Acute | 1.17 (1.00, 1.36) | 56.75 | [71][86] | |||||
| Hospital Admissions | Acute | 1.0188 (−0.40,4.16) for 1-day lag, moving average concentration | 46 | [72][87] | |||||
| Hospital Admissions | Chronic | 1.18 (1.05, 1.34) per IQR for NO2 1.18 (1.05, 1.34) per IQR for NOx |
40.2 (NO2) 71.1 (NOx) |
[70][85] | |||||
| Emergency Room Visits | Chronic | 1.02 (−0.6, 4.6) | [73][88] | [81][96] | |||||
| Hospital Admissions | Acute | 2.23 (1.02, 4.91) | 56.75 | [71][86] | |||||
| Emergency Room Visits | Acute | 1.0342 (1.0210, 1.0475) | 32.79–53.23 | [75][90] | |||||
| Acute | 1.0506 (1.0233, 1.0786) | 24.69 | [77][92] | Cancer-Kidney | Chronic | 1.2 | [ | ||
| Acute | 40 | ] | 1.0740 (1.0545, 1.0938)[61] | ||||||
| 30.13 | [ | 77 | ][92] | Cancer-Other | Chronic | 1.06 | [ | ||
| Acute | 40 | ] | 1.0429 (1.0217, 1.0645)[61] | ||||||
| 33.35 | [ | 77 | ][92] | Cancer | Lung | Chronic | 1.12 | ||
| Depression | Depressive Symptoms | Chronic | 1.50 (1.27, 1.67)* per 10 μg·m−3 increase NO2 1.38 (1.18, 1.53)* per 20 μg·m−3 increase NOx | [1][8][19][34] | 57.3 (NO2[43][44][45][46][,5547,63],64,65[,6648][3,4,7,41,67] | ||||
| ) | 92.8 (NO | x | ) | [81][96] | Brain | Chronic | [ | ||
| Chronic | 34 | ] | 1.33 (1.27, 1.39)* for highest quartile exposure[49][55,68] | ||||||
| [ | 82 | ][97] | Cervical | Chronic | [34][49][55,68] | ||||
| Acute | 1.25 (1.11, 1.36)* | 36.2 | [83][98] | Breast | Chronic | ||||
| Acute | 1.24 (0.99, 1.43)* per IQR | 31.4 | [84][99] | ||||||
| Chronic | 1.24 (1.06, 1.39)* | 11.7–18.8 | [85][100] | 25 | |||||
| Chronic | 1.35 (1.07, 1.52)* for NO2 1.27 (0.94, 1.50)* for NOx |
25.9 (NO2) 39.6 (NOx) |
[86][101] | ][27,17[,2828],46[50] | |||||
| Chronic | 1.05 (0.98, 1.11)* for NO2 1.05 (0.99, 1.09)* for NOx | , | 48[51],49[52],69[53],70[54],71[,72,73] | ||||||
| [ | 65 | ][81] | Cardiovascular | Chronic | 1.004–1.03 | [ | |||
| Medication Use | 31 | ] | [50][51 | Chronic][28,52,69] | |||||
| 1.03 (1.00, 1.05)* per IQR | 23.4 | [ | 67 | ][82] | Respiratory | Chronic | 1.004–1.03 | [2][50]28[51][56],69[57],74[58][ | |
| Depressive Disorder | Chronic | 16 | 1.13 (0.95, 1.28)*,,75,76] | ||||||
| 27.5 | [ | 21 | ] | [43] | Lung Cancer | Chronic | 1.05 | [19][51][28,41] | |
| Coronary Heart Disease | Chronic | 1.05 | [51][28] | ||||||
| COPD | Chronic | 1.03 | [51][28] | ||||||
| Pneumonia | Chronic | 1.08 | [51][28] | ||||||
| Diabetes | Chronic | 1.04 | [51][28] |
| Acute | |||||
| Chronic | |||||
| 1.05 (0.86, 1.20)* per 188 μg·m | |||||
| −3 | |||||
| -30 days before indexing date | |||||
| 46 | |||||
| [ | |||||
| 87 | |||||
| ] | |||||
| [ | |||||
| 102 | |||||
| ] | |||||
| Chronic | |||||
| 1.05 (0.78, 1.21)* per 188 μg·m | |||||
| −3 | |||||
| -365 days before indexing date | |||||
| 46.1 | |||||
| [ | |||||
| 87 | |||||
| ] | |||||
| [ | |||||
| 102 | |||||
| ] | |||||
| Acute | |||||
| 1.04 (0.99, 1.08)* per IQR | |||||
| 34.78 | |||||
| [ | |||||
| 88 | ] | [ | 103] | ||
| Chronic | 1.37 (0.99, 1.60)* highest vs. lowest tertile range | 34.64 | [68][83] | ||
| Major Depressive Disorder | Chronic | 1.14 (0.72, 1.41)* highest IQR for NO2 1.30 (0.96, 1.53)* highest IQR for NOx |
26.04 (NO2), 35.19 (NOx)–mean 39.85 (NO2), 59.71 (NOx)–Q4 | [89][104] | |
| Emergency Room Visits | Acute | 1.039 (1.013, 1.066)-Cold Season 1.066 (1.012, 1.124)-Warm Season |
41.17 | [90][105] | |
| Acute | 1.10 (1.066, 1.136) per 20.1 ppb NO2-All Season 1.20 (1.133, 1.272) per 20.1 ppb NO2-Warm Season 1.064 (1.021, 1.108) per 20.1 ppb NO2-Cold Season |
37.79 | [90][105] | ||
| Acute | 1.03 (0.98, 1.04)*-Warm Season, Male 1.03 (1.00, 1.05)*-Warm Season, Female |
22.18 | [91][106] | ||
| Acute | 1.0369 (1.0224, 1.052) | 32.79–53.23 | [75][90] | ||
| Acute | 1.08 (1.03, 1.12)* | [92][107] | |||
| Acute | 0.9875 (0.9704, 1.0049) per IQR | 23.57 | [76][91] | ||
| Acute | 1.36 (0.44, 2.28) | 48.5 | [93][108] | ||
| Acute | 1.0494 (1.0270, 1.0723) | 24.69 | [77][92] | ||
| Acute | 1.0802 (1.0623, 1.0984) | 30.13 | [77][92] | ||
| Hospital Admissions | Acute | 1.18 (0.55, 2.53) | 56.75 | [71][86] | |
| Acute | 1.0178 (1.0073, 1.0283)-1-day Lag | 34.6 | [94][109] | ||
| Suicide | Emergency Room Visits | Acute | 1.112 (1.006, 1.228) All Seasons, Male, 1-day Lag 1.239 (1.078, 1.424)-Cold Season, Male, 1-day Lag |
36.47 | [95][110] |
| Acute | 0.9990 (0.9730, 1.0258) per IQR | 23.57 | [76][91] | ||
| Risk of Death by Suicide | Chronic | 1.33 (1.09, 1.64) | 48.20 | [96][111] | |
| 1.39 (1.03, 1.87)-for individuals with pre-existing physical or mental disease | 48.20 | [96][111] | |||
| Acute | 1.06 (1.01, 1.12)*-All Gender, Under 30 years old, 0-day Lag 1.04 (1.00, 1.08)*-All Age, Warm Season, 0-day Lag |
68.94 | [97][112] | ||
| Acute | 1.019 (0.999, 1.039)-0–1 day Lag | [98][113] | |||
| Acute | 1.0057 (1.0023, 1.0081) | 18.7 | [78][93] | ||
| Completed Suicide | Acute | 1.17 (1.04, 1.29)*-all 1.26 (1.09, 1.40)*-Spring and Fall Transitions | [99][114] | ||
| Alzheimer’s Disease | Hospital Admissions | Chronic | 1.06 (0.96, 1.17) | 26.2 | [40][61] |
| Parkinson’s Disease | Parkinson’s Disease | Chronic | 1.08 (0.94, 1.24) | 26.2 | [40][61] |
Citation of original work: Shaw, S.; Van Heyst, B. An Evaluation of Risk Ratios on Physical and Mental Health Correlations due to Increases in Ambient Nitrogen Oxide (NOx) Concentrations. Atmosphere 2022, 13, 967. https://doi.org/10.3390/ atmos13060967