Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Carolina Burnay and Version 2 by Lindsay Dong.
Drowning causes significant mortality and morbidity globally, and infants (0–4 years of age) are disproportionately impacted. In a groundbreaking approach to pediatric drowning prevention, ecological psychology has been used to investigate the relationship between infants’ perceptual–motor development and their behavior around bodies of water. Through crawling experience, infants learn to perceive the risk of falling into water and start adapting their behavior to avoid drop-offs leading into water. Infants tend to enter deep water more when the access is via a slope than via a drop-off.
- cliff
- water slope
- child
- development
- environment
- risk
1. Introduction
Drowning has been identified as a public health threat by the World Health Organization (WHO) [1]. The United Nations (UN) General Assembly [2] resolution suggests drowning prevention strategies must be prioritized by governments. Over half of all fatal unintentional drownings globally occur among children and young people under 25 years of age, with children 0–4 years of age recording the highest drowning rates [1]. Drowning often occurs among this age group in water bodies inside the home for children under 1 (such as bathtubs) [2] and in water bodies outside but close to the home (such as ponds, ditches, swimming pools), in children 1–4 years of age [3]. Drowning among young children is due to a range of age-related developmental factors and hazards and risks in the child’s environment (e.g., unrestricted access to water, lapses in or absence of adult supervision) [4].
The first few years of human life are characterized by an extraordinary number of developmental changes that occur at a remarkably rapid pace. Infants younger than 12 months of age are dependent on their caregivers to survive; they are fed, cleaned and, before they start self-locomoting, they are carried. Infants grow every day, their body dimensions and capabilities change, they conquer new skills, they gradually become more independent, and they are eager to explore the world. Although this exploratory behavior is vital for infants to learn to distinguish possible from impossible (or dangerous) actions [5], it also puts them at risk of injuries from failures to accurately perceive risks in the environment.
2. Infant Drowning Risk
Epidemiological data have been used to develop strategies to prevent drowning [6]. This approach is essential to understand who is at risk and where drowning is more likely to occur. Importantly, by having updated epidemiological information, pweople can monitor the effectiveness of drowning prevention strategies. The Global Burden of Disease (GBD) Study estimates that children 1–4 years of age have the highest number of unintentional drowning deaths when compared to other age groups [7]. In 2019, drowning resulted in 32,070 deaths (95% uncertainty interval (UI): 26,399.60–39,587.44) of children 1–4 years of age, an age-adjusted fatality rate of 6.04 (UI: 4.97–7.46) per 100,000 children [8]. Drowning also results in 1469.91 (UI: 975.50–2108.07) years lived with disability (YLDs) among children in the 1–4 years age group [8]. Among infants younger than 1 year of age, unintentional drowning claims the lives of an estimated 867 children (UI: 619.93–1089.83), a mortality rate of 2.64 per 100,000 children [8]. The highest fatal drowning rates are seen in low socio-demographic index (SDI) countries, a rate of 3.99 per 100,000 for children less than 1 year of age and 8.55 per 100,000 for 1–4-year-old children in low SDI countries, compared to a rate of 0.77 for children less than 1 year of age and 1.40 for 1–4-year-old children in high SDI countries [8]. The high proportion of drownings with a fatal outcome in low SDI nations is evident in the lower YLD-related drowning rates for children less than 4 years of age, when compared to those from high SDI nations [8].3. The Multiple Layers of Protection
Drowning prevention is most effective when multiple layers of protection work together [6]. Infants are overrepresented in drowning statistics because they become “mobile but [are] too young to recognize danger or to get out of water” (p. 9) [1]. To protect mobile infants from drowning, the WHO suggests four strategies that constitute layers of defense [1]. The first and most obvious suggested layers of protection are barriers around water, such as pool fencing [9][10][9,10] and adult supervision [1][6][1,6]. However, barriers are not always an option, nor absolutely childproof [11]. Some bodies of water, such as beaches or rivers, cannot be fenced [12]. In addition, research has shown that no barrier can assure a 100% effective means to prevent infants from getting to the water [13]. If the body of water is not fenced or if children manage to overcome the protective physical barriers, adult supervision is the next most effective protective layer. However, as shown by Moran [14], it is not uncommon that children find themselves close to a body of water with limited or no adult supervision. Similarly, young children may be left in the care of older children, unsuited for the provision of supervision required to reduce drowning risk [15][16][15,16], or even distracted adults [15]. Swimming skills are suggested as the third layer that ultimately can help children to survive in the water. However, the benefits of swimming programs to very young children (younger than three years of age) have been historically controversial. In the 1970s and 1980s, experts, including the American Academy of Pediatrics, discouraged swimming programs for children younger than three years, arguing that this kind of exposure would offer a false sense of security to the children and their parents [17][18][17,18]. Recently, a systematic review conducted by Taylor and colleagues reported that children aged 2–4 years can develop age-appropriate aquatic competencies, and the learning of these skills may increase water safety [19]. However, a very limited number of studies have addressed the effect of swimming ability on preventing drowning for young children, and no evidence was found that children under 1 year of age are capable of learning how to survive in the water because they cannot intentionally control their breathing [19]. Therefore, the benefits of swimming courses for infant drowning prevention need to be further investigated [19]. It seems then that if barriers and adult supervision fail, young children are completely vulnerable to drowning. While devices such as lifejackets play an important role in drowning prevention [20], their appropriateness for young children and the typical drowning scenarios seen among this age group are questionable. This leaves a final and least reliable layer of defense, i.e., rescue and resuscitation [21].4. The Ecological Psychology Approach to Infant Drowning Prevention
Ecological psychology focuses specifically on the interdependence of humans and their environments. It stresses that perception is an active process and that action and mobility play particularly important roles in modulating perceptual processes and their development [22]. How children perceive possibilities for action, or affordances [23], depends on the relationship between their characteristics, including the interaction of various developing systems (e.g., perceptual, motor, cognitive, etc.), and the characteristics of the environment. Through the use of their own bodies during goal-directed activity, children get acquainted with their surroundings and begin perceiving affordances in the environment [22]. When infants start self-locomoting, a solid surface affords crawling or walking, but the water surface does not. Although infants’ capacity to control locomotion improves rapidly, their perception of the affordances for locomotion lags behind their capacity for control. They need to perceive the relationship between their capabilities and the environment’s features to avoid drowning. Ecological psychology has long been used to investigate child–environment relationships and the effects of perceptual–motor development on infants’ behavior in risky scenarios, such as drop-offs [24], but only recently have researchers begun to investigate infants’ relationship with bodies of water from an ecological perspective. This ecological line of investigation started with the classical Visual Cliff paradigm [25]. Eleanor Gibson and Richard Walk (1960) tested the avoidance behavior of human babies, among other animal species, on a drop-off covered with a transparent glass surface, the visual cliff [25]. They reported that crawling infants would avoid crossing visual cliffs, similar to other young animals [25]. However, Gibson and Walk did not compare infants at different stages of locomotor development [25]. Later studies using the classical visual cliff paradigm and its adaptations have shown that soon after infants start crawling, they tend to cross visual cliffs [26] and risky slopes [27] and to fall into gaps in the surface [28] and even over the edge of real cliffs [29]. After weeks of crawling experience, infants start perceiving the risk of falls and start adapting their behavior to avoid visual cliffs [30], steep slopes [31], impossible-to-transverse gaps [28] and dangerous drop-offs [29]. In a literally “ground-breaking” approach, ecological psychology and the related concept of affordances was used to develop a novel approach to infants’ drowning prevention. To investigate the interaction between infants’ perceptual–motor development and aquatic environments, Burnay and Cordovil [32] adapted the visual cliff paradigm and created the Real Cliff/Water Cliff apparatus (i.e., 75-cm-high platform with no protection from a fall on one side, the real cliff, and one with a tub filled with water on the opposite side, the water cliff) (Figure 1). Burnay and colleagues tested 58 crawling and 44 walking infants [32][33][32,33] and 25 infants who transitioned from crawling to walking in a longitudinal study design [34] on both the real and water cliffs. The results confirmed the effect of crawling experience on infants avoidance of real cliffs and showed the same effect on infants avoidance of the water cliff [32][33][34][32,33,34]. Infants with more crawling experience avoided falling on the real and the water cliffs and their behavior was indiscriminable on the real and the water cliff. For the first time, locomotor experience was linked to infants’ avoidance of bodies of water.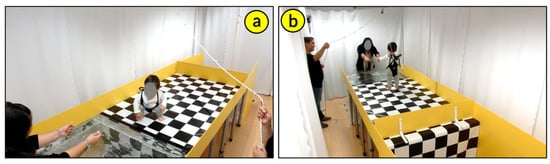
Figure 1. Real Cliff/Water Cliff apparatus synchronized cameras’ view. (a) water cliff camera front view and (b) water cliff camera back view. Photo reproduced with permission of the infant’s mother.
Through crawling, infants learn to perceive information specifying important characteristics of the surface of support and start avoiding situations that do not support safe locomotion. After acquiring the necessary self-produced locomotor experience, when facing a drop-off, filled with water or not, babies avoid going farther because they perceive the environment does not afford safe locomotion.
These studies raised a new question: what if, instead of a sudden drop-off, the access into the water is smooth and gradual? In many natural aquatic environments, such as beaches and ponds, and in swimming pools designed to facilitate entry for people with disabilities, entrances to the water can be less obvious than a sudden drop-off. Would self-produced locomotor experience inform infants’ perception of the risk when slopes lead into deep water?
To answer this question, in a follow-up study, Burnay and colleagues [35] created the Water Slope paradigm to test infants’ perception and action on sloped accessways into deep water. The water slope is a 10° declined platform leading to 75-cm-deep water (Figure 2). Contrary to what was observed on the water cliff, self-produced locomotor experience was not linked to infants’ avoidance of submersion on the water slope (i.e., water touching the infants chin) [35]. Importantly, of the 77 infants tested on the water slope, 62% reached the submersion point [35], while on the water cliff, of the 102 infants tested on a cross-sectional design [35], only 30% fell into the water. The authors argue that if the access into the water affords locomotion (i.e., smooth slope), infants tend to locomote, presumably because locomotor experience has no influence on infants’ perception of the risk of deep water.
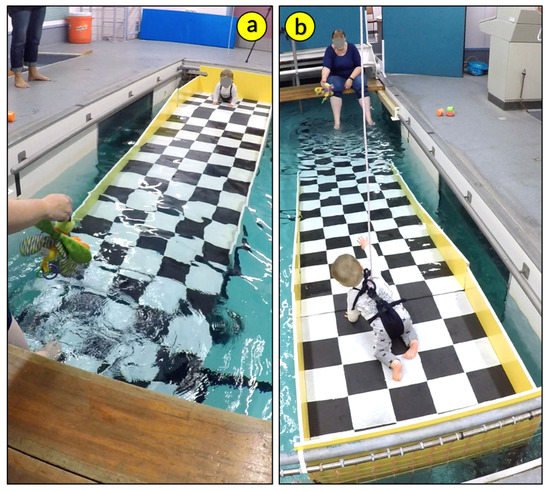
Figure 2. Water slope apparatus synchronized cameras’ view. (a) camera front view and (b) camera back view. Photo reproduced with permission of the infant’s mother.