Post-COVID syndrome or long COVID is defined as the persistence of symptoms after confirmed SARS-CoV-2 infection, the pathogen responsible for coronavirus disease. The content herein presented reviews the reported long-term consequences and aftereffects of COVID-19 infection and the potential strategies to adopt for their management. Recent studies have shown that severe forms of COVID-19 can progress into acute respiratory distress syndrome (ARDS), a predisposing factor of pulmonary fibrosis that can irreversibly compromise respiratory function. Considering that the most serious complications are observed in the airways, the inhalation delivery of drugs directly to the lungs should be preferred, since it allows to lower the dose and systemic side effects.
Although further studies are needed to optimize these techniques, recent studies have also shown the importance of in vitro models to recreate the SARS-CoV-2 infection and study its sequelae. The information reported suggests the necessity to develop new inhalation therapies in order to improve the quality of life of patients who suffer from this condition.
- post-COVID syndrome
- long COVID
- inhalation therapy
- post-COVID sequelae
1. Introduction
2. Long-Term Consequences and After-effects of COVID Infection
Coronavirus disease 2019 (COVID-19) is caused by a novel coronavirus known as Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and it was declared a pandemic by the World Health Organization on 11 March 2020 [11]. Coronaviruses are single-stranded, positive-sense RNA viruses that can infect animals and humans. COVID-19 is transmitted between people through small airborne droplets emanated by an infected individual, personal contact (shaking hands), and by touching infected surfaces [12]. This disease often causes no symptoms or mild symptoms in the patients affected by the virus; consequently, they usually have a good prognosis. However, many of these cases develop symptoms in a more severe form that can lead to complications that persist long after the infection [13]. In particular, although COVID-19-associated symptomatology was more evident in individuals with severe disease, individuals with mild and moderate disease also reported a wide range of manifestations after the resolution of the clinical disease [14]. Since the new SARS-CoV-2 is genetically comparable to previously discovered coronavirus strains, such as SARS-CoV and MERS-CoV, it is highly expected that the consequences in patients recovered from COVID-19 are analogous to those of SARS and MERS [15]. Thus, a careful evaluation of the data available in follow-up studies of these infections could provide a useful scenario for identifying effective therapeutic protocols in the treatment of long-COVID syndromes. SARS-CoV-2 infection mostly affects the respiratory system [8] with complications ranging from mild fatigue to severe forms requiring long-term oxygen therapy or even lung transplantation [16]. The primary pulmonary manifestations of SARS-CoV-2 include hypoxemia, dyspnea, and cough while severe ones include hypoxemic respiratory failure and ARDS. ARDS may progress into pulmonary fibrosis, which in turn leads to irreversible impairment of respiratory function. Respiratory manifestations typical of post-COVID syndrome include chronic cough and persistent dyspnea [17]. Some patients develop important neuropsychiatric and musculoskeletal symptoms of COVID-19 including cerebrovascular accidents, olfactory and gustatory impairments, delirium, and myalgia. Some of the neuropsychiatric and musculoskeletal symptoms of post-COVID syndrome include sleep abnormalities, encephalopathy, chronic headache, delirium, brain fog, and small joint arthritis [18]. Regarding cardiovascular effects, during the acute phase of the infection, patients may report symptoms of shortness of breath, chest pain, and palpitations. These symptoms may persist up to 6 months after infection. Coagulopathies, thrombotic events that may become recurrent or persistent, hyperglycemia, acute kidney injury, and hepatocellular damage have also been observed (Figure 1) [17,19].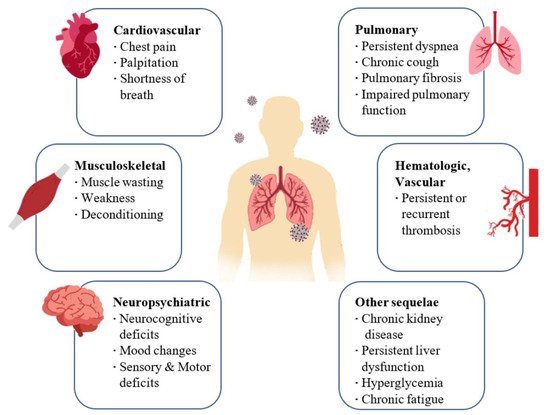
3. Management of Patients with Post-COVID Syndrome and after Effects of SARS-CoV-2 Infection
Considering the events occurring after the infection, several classes of active ingredients may be useful in relieving the effects of infection in the airways (Table 1):
|
Drug |
Category |
Mode of Action |
References |
|
Flavonoids (luteolin, apigenin, kaempferol, fisetin, quercetin, genistein and epigallocatechin gallate) |
Mast cell level Stabilizers |
Anti-inflammatory and mast cell stabilizing effects |
|
|
Antihistamine drugs (olopatadine, rupatadine and ketotifen) |
Mast cell level stabilizers |
Anti-inflammatory and mast cell stabilizing effects |
|
|
Clarithromycin |
Mast cell level Stabilizers |
Anti-inflammatory and mast cell stabilizing effects |
|
|
Dexamethasone |
Corticosteroids |
Anti-inflammatory action |
[48] |
|
Ciclesonide |
Corticosteroids |
Anti-inflammatory action |
[53] |
|
Azithromycin |
Antibiotics |
Inhibit the proliferation of fibroblasts, reduce the production of collagen and the levels of TGF-β |
[57] |
|
Pirfenidone |
Antifibrotic |
Inhibit the synthesis of collagen induced by TGF-β; suppresses the production of TNF-α, IFN-γ, IL-1β and IL-6; suppresses the differentiation of fibroblasts associated with TGF-β |
[61] |
|
Curcumin |
Antifibrotic |
Decreasing the expression of the TGF-β II receptor (TGF-ß RII), as well as in directly reducing the expression of the TGF-β protein and its mRNA |
[22] |
|
N-Acetylcysteine (NAC) |
Antioxidants |
Inhibits virus replication and expression of pro-inflammatory molecules. boosting a type of cell in your immune system that attacks infections |
[63] |
|
GSH |
Antioxidants |
Blocks viral replication through redox state modulation |
[64] |
|
Molnupiravir |
Antivirals |
Inhibits the replication of SARS-CoV-2, acting on the enzyme that the virus uses to generate copies of itself by introducing errors into its genetic code |
[66] |
|
Zofin |
Derived from human amniotic fluid |
Suppressor of cytokine activation |
[67] |
|
Ampion |
Biological Drug |
Modulate inflammatory cytokine levels |
[69] |
Recently, Ampio Pharmaceuticals launched a phase I randomized study to evaluate the safety, tolerability, and efficacy of nebulized Ampion in improving the clinical outcomes of 40 patients hospitalized with COVID-19 infections, with persistent respiratory symptoms. Details on the study will be published as soon as they are ready [69] Ampion is the low molecular weight filtrate of human serum albumin and as an immunomodulatory agent with anti-inflammatory effects; it has the potential to modulate inflammatory cytokine levels related to COVID-19 disease and respiratory complications, such as respiratory distress syndrome. acute (ARDS). Administration of Ampion to patients by inhalation allows the drug to reach the target site directly and attenuate lung inflammation [12].
6. Conclusions
Post-COVID syndrome is a new condition that can adversely affect quality of life, regardless of age and the presence of pre-existing diseases. Unfortunately, it is not yet possible to know which patients are most at risk of developing long-term consequences and whether these problems will solve, improve, or become permanent. This review examined the reports of the scientific community on the long-term consequences of COVID-19 and its after-effects, particularly in the lung, as the main site of infection, and possible treatment options useful for alleviating its symptoms. Active ingredients demonstrating a biological logic in the treatment of post-COVID sequelae have been reported, concluding that the most appropriate type of formulation for their administration is inhalation, allowing forthe release of the drug directly on the site of action with a reduction in dose and systemic side effects. Considering also that pulmonary fibrosis has been reported as one of the most serious consequences, the development of new in vitro experimental models, able to faithfully recreate the infection, will help scientists and pharmaceutical companies around the world to develop therapeutic strategies for similar conditions; although, further studies are needed to overcome the limitations of these techniques.