Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Teja Senekovič Kojc and Version 2 by Dean Liu.
Novel biomarkers of heart failure are the subject of numerous studies. Biomarkers of heart failure can be determined in the blood and in the urine. The future of biomarker use is in multimarker panels that include a combination of biomarkers with different pathophysiological mechanisms in order to improve their diagnostic and prognostic predictive value.
- biomarkers
- heart failure
- myocardial stretch
- myocyte injury
- myocardial remodeling
- inflammation
- renal dysfunction
- oxidative stress
- child
1. Introduction
Despite advances in medicine, heart failure is still an important cause of morbidity and mortality in the modern world. Consequently, there is a considerable need to find new ways of predicting, screening, and prognosticating heart failure, especially in pediatrics [1]. Laboratory diagnostics is an important part of the decision-making process in everyday clinical practice in order to come to a diagnosis, and additionally for risk stratification and therapeutical choices [2].
Various novel biomarkers of heart failure have been studied in adults. However, reliable novel biomarkers of heart failure in pediatrics have not been sufficiently studied for everyday clinical practice yet, therefore, additional knowledge is very welcome. RIn this researchersview, we try to classify biomarkers according to the pathophysiological mechanisms that contribute to the development of heart failure. Several biomarkers of heart failure are still under evaluation and a detailed review of all of them is beyond the scope of this narrative review.
In pediatrics, biomarkers of heart failure are particularly important for the early identification and risk stratification of patients with systemic diseases and associated risk for early development of heart failure. Good biomarkers have the following characteristics: high sensitivity and specificity, the possibility of simultaneous processing of many samples, short analysis time, low cost, and good clinical applications, thus predicting the risk of heart failure and the associated prognosis as well as the adequacy of monitoring [3].
Two strategies are currently in place to detect newer biomarkers of heart failure, the first is based on proteomics and metabolomics, which means comparing blood and tissue samples from patients with heart failure with healthy individuals. It provides data on the expression of proteins and their breakdown products [4]. This first approach does not provide a lot of information about the pathophysiological processes that lead to the disease, which is typical for the second approach, based on the mechanisms underlying the development of cardiovascular disease [5]. Biomarkers of heart failure can be determined in blood samples and some also in urine samples. RIn this researchers view, we will present seven groups of newer biomarkers that are associated with heart failure based on pathophysiological mechanisms, as seen in Table 1. Normal values of some biomarkers of heart failure are presented in Table 2 [6][7][8][9][6,7,8,9]. In addition, rwesearchers will also highlight the possibilities of determining biomarkers in the urine, which allows less invasive sampling and better participation of patients and healthy individuals in potential clinical studies.
Table 1.
Biomarkers of heart failure based on pathophysiological mechanisms.
| Myocardial Stretch | Myocyte Injury | Myocardial Remodeling | Inflammation | Renal Dysfunction | Neurohumoral Activation | Oxidative Stress | |||
|---|---|---|---|---|---|---|---|---|---|
| Biomarker | Adult Population | Pediatric Population | |||||||
| BNP 1 | CTn | ||||||||
| BNP 1 | 5 (TnI 6, TnT 7) | galectin-3 | GDF-15 12 | NGAL 19 | MR-proADM 24 | ceruloplasmin | |||
| <35 ng/L | NT-proBNP 2 | hs-cTn 8 | sST2 11 | EMPs 13 | KIM-1 20 | ||||
| NT-proBNP 2 | <125 ng/L | <3569 ng/L (0–1 Y | copeptin | 11) | MPO | 26 | |||
| <178 ng/L (1–19 Y) | ANP 3 | H-FABPs 9 | microRNAs | EPCs 14 | cystatin C | MMPs 25 | SUA 27 | ||
| MR-proANP 3 | <40 pmol/L | MR-proANP 4 | GSTP1 10 | CRP 15 | IL-18 21 | ||||
| HsTnT 4 | <14 ng/L | <78 ng/L (0–6 M 12) <34 ng/L (6 M–1 Y) <6 ng/L (1–19 Y) | vitamin D3 | ||||||
| hs-CRP 16 | |||||||||
| HsTnI 5 | L-FABP | 22 | 8-hydroxy-2-0-deoxyguanosine | ||||||
| <6 ng/L | <93.8 ng/L (<1 M) | <52.1 ng/L (1–12 M) <48.1 ng/L (1–12 Y) <3.9 ng/L (13–18 Y) |
TNF-α 17 | NAG 23 | |||||
| H-FABPs 6 | <19 ng/mL | IL-6 18 | β-2 microglobulin | ||||||
| glutathione-S-transferase |
1 BNP, brain natriuretic peptide; 2 NT-proBNP, N-terminal-proBNP; 3 ANP, atrial natriuretic peptide; 4 MR-proANP, mid-regional proatrial natriuretic peptide; 5 cTn, cardiac troponins; 6 TnI, troponin I; 7 TnT, troponin T; 8 hs-cTn, high-sensitivity cardiac troponin; 9 H-FABPs, heart-type fatty acid-binding proteins; 10 GSTP1, glutathione transferase P1; 11 sST2, soluble isoform of suppression of tumorigenicity 2; 12 GDF-15, growth differentiation factor-15; 13 EMPs, endothelial microparticles; 14 EPCs, endothelial progenitor cells; 15 CRP, C-reactive protein; 16 hs-CRP, high-sensitivity C-reactive protein; 17 TNF-α, tumor necrosis factor alpha; 18 IL-6, interleukin-6; 19 NGAL, neutrophil gelatinase-associated lipocalin; 20 KIM-1, kidney injury molecule-1; 21 IL-18, interleukin-18; 22 L-FABP, liver-type fatty acid-binding protein; 23 NAG, N-acetyl-β-D-glucosaminidase; 24 MR-proADM, mid-regional pro-adrenomedullin; 25 MMPs, matrix metalloproteinases; 26 MPO, myeloperoxidase; 27 SUA, serum uric acid.
Table 2.
Normal values of some biomarkers of heart failure with pediatric specificities according to available data.
| Galectin-3 | ||
| <22.1 ng/mL | ||
| <33 ng/mL | ||
| sST2 7 | <49.3 ng/mL (male) <33.5 ng/mL (female) |
<50 ng/mL |
| GDF-15 8 | <584 pg/mL | |
| NGAL 9 | <50 ng/mL | |
| MR-proADM 10 | <0.55 nmol/L | |
| Copeptin | <11.25 pmol/L | <13.1 pmol/L |
1 BNP, brain natriuretic peptide; 2 NT-proBNP, N-terminal-proBNP; 3 MR-proANP, mid-regional proatrial natriuretic peptide; 4 hsTnT, high-sensitivity troponin T; 5 hsTnI, high-sensitivity troponin I; 6 H-FABPs, heart-type fatty acid-binding proteins; 7 sST2, soluble isoform of suppression of tumorigenicity 2; 8 GDF-15, growth differentiation factor-15; 9 NGAL, neutrophil gelatinase-associated lipocalin; 10 MR-proADM, mid-regional pro-adrenomedullin; 11 Y, year; 12 M, month.
2. Biomarkers of Myocardial Stretch
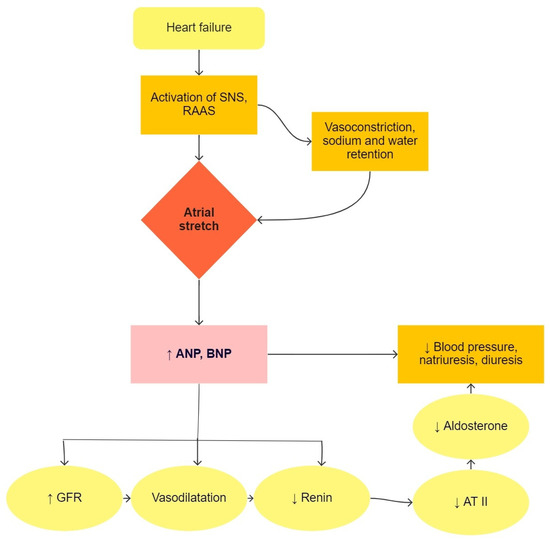
Heart failure is a condition in which the heart is not able to pump enough blood to meet the needs of all tissues [5]. This causes an increase in blood volume by regulating sodium and retaining water in the body. Natriuretic peptides are produced in atrial and ventricular cells due to pressure or volume overload, as seen in Figure 1. ANP (atrial natriuretic peptide) and BNP (brain natriuretic peptide) are used in the diagnosis of heart failure and lead to natriuresis, diuresis, and vasodilatory mechanisms, which are compensatory mechanisms in heart failure [10]. In clinical practice, the precursor of BNP, i.e., NT-proBNP (N-terminal-proBNP), is used primarily in suspected heart failure and in the monitoring of patients with known heart failure. BNP and NT-proBNP values are influenced by age, sex, obesity, renal function, and lung disease [11]. In pediatric patients, NT-proBNP correlates well with the stage of disease and is a better predictive factor of heart failure than BNP [12].Figure 1. The physiological function of natriuretic peptides in heart failure. SNS, sympathetic nervous system; RAAS, renin-angiotensin-aldosterone system; ANP, atrial natriuretic peptide; BNP, brain natriuretic peptide; GFR, glomerular filtration rate; AT II, angiotensin II.
3. Biomarkers of Myocyte Injury
Numerous studies have already been conducted in the field of biomarkers of myocardial damage, as the process of cell death of cardiomyocytes due to apoptosis or necrosis is at the forefront of heart failure. Various mechanisms lead to cell death, such as poorer tissue perfusion, poorer oxygen supply, increased heart muscle load, circulating neurohormones, adrenergic system activation, inflammation, and oxidative stress [13][18].