- health policy
- cancer
- costs
- Disability-Adjusted Life Years
- cost-per-DALY ratio
- economic evaluation
1. Introduction
2. Costs in Cancer-Related Disability-Adjusted Life Years
The pooled cost-per-DALY ratio equals around 9000 USD per DALY accountable to cancer. The total cost per DALY equals approximately one third of the national GDP per capita (32% [95% CI: 24–42%]) (Figure 1).
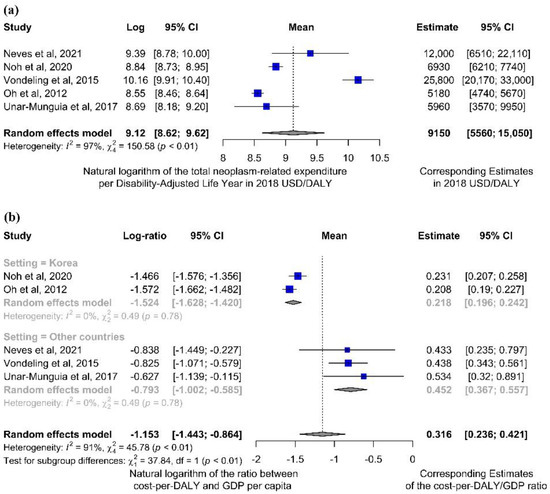
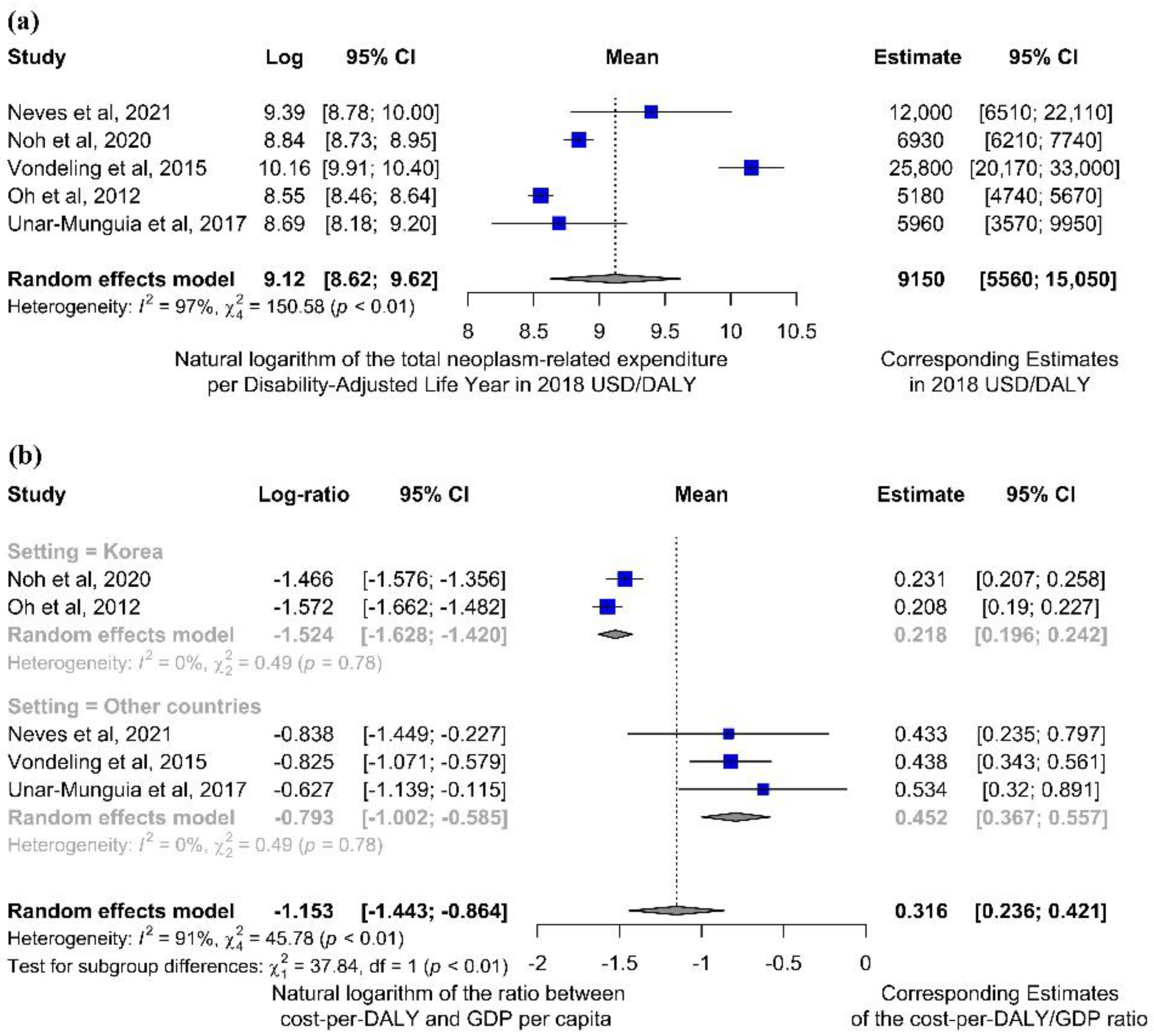
Figure 1. Forest plots for outcomes related to the cost-per-DALY ratio, according to meta-analytic computations described in the Methods. A meta-analytic estimate of the average cost per DALY ascribable to cancer (and its 95% CI), performed considering all studies eligible for the quantitative synthesis [13][14][15][16][17] (a). Expenditures per DALY were also considered in relation to the corresponding GDP per capita; (b) given that two studies were set in the same context (Korea) [14][16], a post-hoc subgroup analysis was also performed by separating them from other settings.
Considering only indirect costs, the pooled ratio was around 4000 USD. Relating the indirect costs-per-DALY ratio to the national GDP results in indirect expenditure per DALY equaling one seventh of the annual country’s economic output per person (Figure 2).
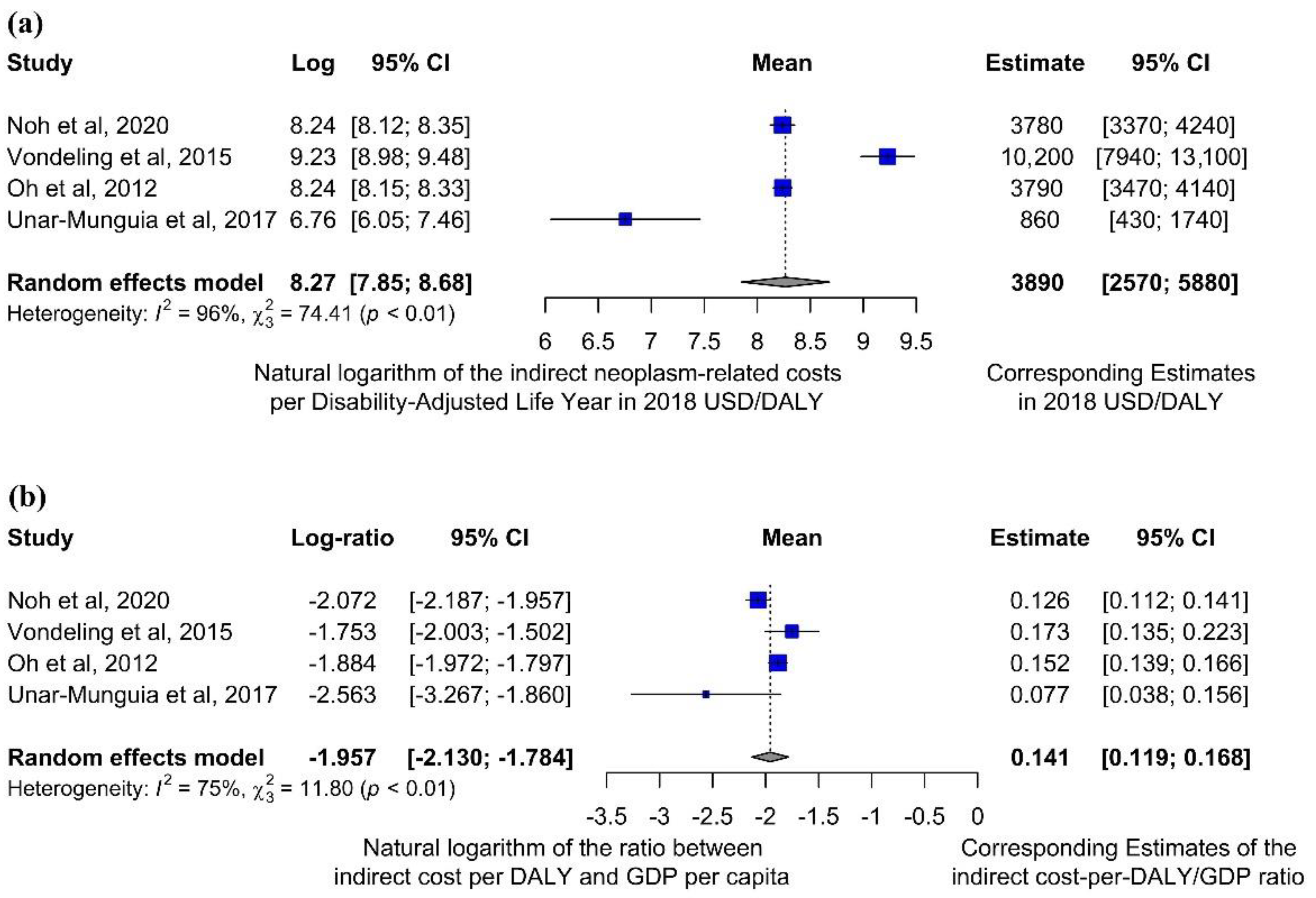
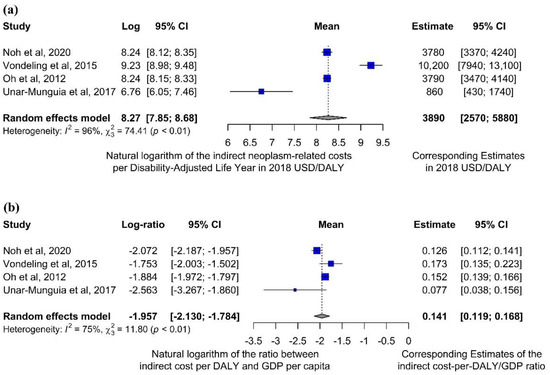 Figure 2. Forest plots for outcomes related to the ratio between indirect costs and DALYs, according to meta-analytic computations described in the Methods. A meta-analytic estimate of the average indirect cost per DALY ascribable to cancer (and its 95% CI), performed considering all studies reporting indirect cost data [14][15][16][17] (a). Indirect expenditures per DALY were also considered in relation to the corresponding GDP per capita (b). One study [13] was not included in this computation due to absence of indirect cost data.
Figure 2. Forest plots for outcomes related to the ratio between indirect costs and DALYs, according to meta-analytic computations described in the Methods. A meta-analytic estimate of the average indirect cost per DALY ascribable to cancer (and its 95% CI), performed considering all studies reporting indirect cost data [14][15][16][17] (a). Indirect expenditures per DALY were also considered in relation to the corresponding GDP per capita (b). One study [13] was not included in this computation due to absence of indirect cost data.
Hence, the overall cancer-related indirect expenditure and productivity losses per DALY ascribable to the disease were much lower than the numerical value of the GDP per-capita, and the same held for the total expenditure (i.e., also including direct costs). This implies that the actual estimates of global costs of the disease may be quite different from the “economic value” obtained multiplying DALYs by the GDP per capita. For example, the fact that cost estimates would be cut by around 70% implies that, if a posteriori computed parameters were used, the global cancer cost estimate forecast in a previous study [13][18] would be reduced from one billion to 300 million 2018 USD.
This might be explained by the fact that GDP measures the monetary value of all final goods and services produced in a country in a given period (generally a year). Consequently, GDP is composed of goods and services produced for sale in the market and includes some non-market production (e.g., defense or education services provided by the government) [14][19], which may entail an excess computation of costs in relation to the actual economic burden of the disease when the GDP is taken as a predetermined proxy of the cost per DALY. Thus, the remarkable differences highlighted by our analysis cast doubts on the reliability of estimates obtained by valuing the monetary burden from simple analyses based on DALYs and GDP per capita, a methodology widely used not only for cancer [15][20] but also in many other sectors such as infectious disease [16][21], injuries [17][22] and maltreatment-related illnesses [18][23].
3. Conclusions
Cancer represents a major health issue, concerning both the clinical burden (in terms of morbidity and mortality) and the consequent economic implications. With regard to the latter, DALYs are often used to measure the burden of disease since they are a compound unit encompassing both disability and mortality, but substantial heterogeneity occurs when they are translated to monetary value. Each DALY due to cancer has shown to cost, on average, around 9000 USD in high- and upper-middle income countries, although this computation can be strongly influenced by fluctuations depending on cancer type and other parameters (e.g., country, prices). Moreover, the cost per cancer-related DALY has been found to be, on average, 32% (95% CI: 24–42%) of the corresponding countries’ GDP per capita, which implies that the use of a priori established parameters, such as GDP or VSL, might lead to presenting rough estimates highly different (even threefold) from what a posteriori emerges after directly retrieving figures and/or building models out of available data. Therefore, further research is needed to understand the actual value of DALYs connected to cancer, and to provide reliable cost estimates that may provide reasonable ground to policy-makers for appropriate decision-making.References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249.
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M.; et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-Adjusted life-years for 29 cancer groups, 1990 to 2017: A systematic analysis for the global burden of disease study. JAMA Oncol. 2019, 5, 1749–1768.
- Davies, S.; Easterbrooke, L.; Taylor, S. The Financial Impacts of Cancer. Available online: https://www.bristol.ac.uk/media-library/sites/geography/pfrc/pfrc1210-financial-impacts-of-cancer-report.pdf (accessed on 13 April 2022).
- Brown, M.L.; Lipscomb, J.; Snyder, C. The Burden of Illness of Cancer: Economic Cost and Quality of Life. Annu. Rev. Public Health 2001, 22, 91–113.
- Cole, A.; Lundqvist, A.; Lorgelly, P.; Norrlid, H.; Schaffer, S.K.; Lewis, F.; Hernandez-Villafuerte, K.; Lindgren, P.; Garau, M.; Welin, K.-O.; et al. Improving Efficiency and Resource Allocation in Future Cancer Care. Available online: https://www.ohe.org/publications/improving-efficiency-and-resource-allocation-future-cancer-care (accessed on 13 April 2022).
- Mattiuzzi, C.; Lippi, G. Cancer statistics: A comparison between World Health Organization (WHO) and Global Burden of Disease (GBD). Eur. J. Public Health 2020, 30, 1026–1027.
- Murray, C.J. Quantifying the burden of disease: The technical basis for disability-adjusted life years. Bull. World Health Organ. 1994, 72, 429–445.
- Murray, C.J.L.; Acharya, A.K. Understanding DALYs. J. Health Econ. 1997, 16, 703–730.
- McCormick, P.J. Cancer Tsunami: Emerging Trends, Economic Burden, and Perioperative Implications. Curr. Anesthesiol. Rep. 2018, 8, 348–354.
- National Cancer Institute Financial Burden of Cancer Care. Available online: https://progressreport.cancer.gov/after/economic_burden#field_most_recent_estimates (accessed on 28 January 2022).
- Schlueter, M.; Chan, K.; Lasry, R.; Price, M. The cost of cancer—A comparative analysis of the direct medical costs of cancer and other major chronic diseases in Europe. PLoS ONE 2020, 15, e0241354.
- World Health Organization (WHO). Cancer—Key Facts. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 8 December 2021).
- Neves, M.; Trigo, F.; Rui, B.; João, C.; Lúcio, P.; Mariana, N.; Mendes, J.; Pedrosa, H.; Geraldes, C. Multiple Myeloma in Portugal: Burden of Disease and Cost of Illness. Pharmacoeconomics 2021, 39, 579–587.
- Noh, J.; Jang, H.; Cho, J.; Kang, D.R.; Kim, T.H.; Shin, D.C.; Kim, C. Estimating the disease burden of lung cancer attributable to residential radon exposure in Korea during 2006–2015: A socio-economic approach. Sci. Total Environ. 2020, 749, 141573.
- Vondeling, G.; Rozenbaum, M.; Dvortsin, E.; Postma, M.; Zeevat, F. Burden of Early and Advanced Breast Cancer in The Netherlands. Value Health 2016, 19, A756.
- Oh, I.H.; Yoon, S.J.; Yoon, T.Y.; Choi, J.M.; Choe, B.K.; Kim, E.J.; Kim, Y.A.; Seo, H.Y.; Park, Y.H. Health and economic burden of major cancers due to smoking in Korea. Asian Pac. J. Cancer Prev. 2012, 13, 1525–1531.
- Unar-Munguía, M.; Meza, R.; Colchero, M.A.; Torres-Mejía, G.; de Cosío, T.G. Economic and disease burden of breast cancer associated with suboptimal breastfeeding practices in Mexico. Cancer Causes Control 2017, 28, 1381–1391.
- John, R.M.; Ross, H. Economic value of disability adjusted life years lost to cancers. J. Clin. Oncol. 2010, 28, 1561.
- Callen, T. Gross Domestic Product: An Economy’s All. Available online: https://www.imf.org/external/pubs/ft/fandd/basics/gdp.htm (accessed on 13 December 2020).
- De la Jara, J.J.; Bastias, G.; Ferreccio, C.; Moscoso, C.; Sagues, S.; Cid, C.; Bronstein, E.; Herrera, C.; Nervi, B.; Corvalan, A.; et al. A snapshot of cancer in Chile: Analytical frameworks for developing a cancer policy. Biol. Res. 2015, 48, 10.
- Townsend, J.; Greenland, K.; Curtis, V. Costs of diarrhoea and acute respiratory infection attributable to not handwashing: The cases of India and China. Trop. Med. Int. Health 2017, 22, 74–81.
- Dalal, K.; Svanström, L. Economic Burden of Disability Adjusted Life Years (DALYs) of Injuries. Health 2015, 7, 487–494.
- Mo, X.; Gai, R.T.; Tachibana, Y.; Bolt, T.; Takahashi, Y.; Nakayama, T. The burden of disease and the cost of illness attributable to child maltreatment in Japan: Long-term health consequences largely matter. BMC Public Health 2020, 20, 1296.
- Ranganathan, K.; Singh, P.; Raghavendran, K.; Wilkins, E.G.; Hamill, J.B.; Aliu, O.; Newman, L.A.; Hutton, D.; Momoh, A.O. The Global Macroeconomic Burden of Breast Cancer. Ann. Surg. 2021, 274, 1067–1072.
- Ashenfelter, O.; Greenstone, M. Estimating the Value of a Statistical Life: The Importance of Omitted Variables and Publication Bias. Am. Econ. Rev. 2004, 94, 454–460.
- Kniesner, T.J.; Viscusi, W.K. The Value of a Statistical Life. Vanderbilt Law Research Paper No. 19-15. 2019. Available online: https://law.vanderbilt.edu/phd/faculty/w-kip-viscusi/368_Value_of_Statistical_Life_Oxford.pdf (accessed on 14 December 2021).
- Bellavance, F.; Dionne, G.; Lebeau, M. The value of a statistical life: A meta-analysis with a mixed effects regression model. J. Health Econ. 2009, 28, 444–464.
- Gong, J.; Cheung, S.; Fasso-Opie, A.; Galvin, O.; Moniz, L.S.; Earle, D.; Durham, T.; Menzo, J.; Li, N.; Duffy, S.; et al. The impact of inherited retinal diseases in the united states of america (Us) and canada from a cost-of-illness perspective. Clin. Ophthalmol. 2021, 15, 2855–2866.
- Lebeau, M.; Duguay, P.; Boucher, A. Costs of occupational injuries and diseases in Québec. J. Saf. Res. 2014, 50, 89–98.
- Herrera-Araujo, D.; Mikecz, O.; Pica-Ciamarra, U. Placing a monetary value on the human health component of zoonotic diseases: A methodological note with an application to cysticercosis in Africa. Prev. Vet. Med. 2020, 175, 104862.
- Miller, T.R.; Waehrer, G.M.; Oh, D.L.; Boparai, S.P.; Walker, S.O.; Marques, S.S.; Harris, N.B. Adult health burden and costs in California during 2013 associated with prior adverse childhood experiences. PLoS ONE 2020, 15, e0228019.
- Hirth, R.A.; Chernew, M.E.; Miller, E.; Fendrick, A.M.; Weissert, W.G. Willingness to pay for a quality-adjusted life year: In search of a standard. Med. Decis. Mak. 2000, 20, 332–342.
- Viscusi, W.K.; Masterman, C.J. Income Elasticities and Global Values of a Statistical Life. J. Benefit-Cost Anal. 2017, 8, 226–250.
- World Cancer Leaders’ Summit. The Economics of Cancer Prevention & Control. 2014. Available online: https://www.uicc.org/sites/main/files/atoms/files/WCLS2014_economics_of_cancer_FINAL.pdf (accessed on 13 April 2022).
- Cheatley, J.; Aldea, A.; Lerouge, A.; Devaux, M.; Vuik, S.; Cecchini, M. Tackling the cancer burden: The economic impact of primary prevention policies. Mol. Oncol. 2021, 15, 779–789.
- Emmons, K.M.; Colditz, G.A. Realizing the Potential of Cancer Prevention—The Role of Implementation Science. N. Engl. J. Med. 2017, 376, 986–990.