Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Conner Chen and Version 1 by Kyu-ho Yi.
As wrinkle removal using BoNT is being performed more often, the adverse effects, such as paralysis of the nearby muscles, diplopia, ptosis, and samurai eyebrows have been reported. When treating wrinkles with BoNT in the nasal region, significant problems, such as diplopia may result from unintended paralysis of the rectus inferior or medialis. To prevent these side effects, the injection should be administered at an anatomically accurate location of the targeting muscle, and the initial treatment should be at a reduced dosage.
- nasalis muscle
- procerus muscle
- levator labii superioris alaeque muscles
1. Introduction
Botulinum neurotoxin (BoNT) prevents neural connections by stimulating the release of acetylcholine at the motor endplates, obstructing the muscle from contracting [1,2][1][2]. In aesthetic clinics, BoNT is commonly used primarily to eliminate wrinkles in the nose region by weakening the muscles involved in facial expression, such as the procerus, nasalis, and levator labii superioris alaeque nasi muscles. The primary aesthetic concerns in the nose region are the bunny lines, horizontal radix line, and nasal side wall scrunch wrinkles for many individuals (Figure 1).
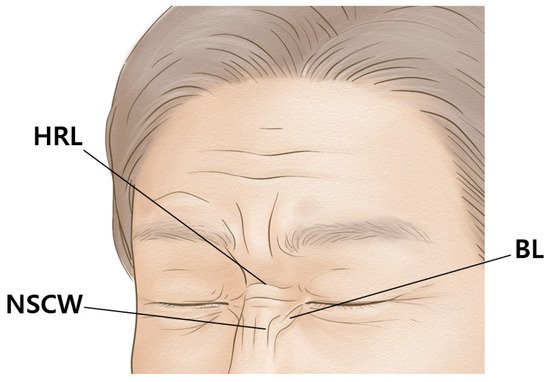
Figure 1. The wrinkles of the nose region are the bunny lines (BL), horizontal radix line (HRL), and nasal side wall scrunch wrinkles (NSCW).
As wrinkle removal using BoNT is being performed more often, the adverse effects, such as paralysis of the nearby muscles, diplopia, ptosis, and samurai eyebrows have been reported [3]. When treating wrinkles with BoNT in the nasal region, significant problems, such as diplopia may result from unintended paralysis of the rectus inferior or medialis [4,5][4][5]. To prevent these side effects, the injection should be administered at an anatomically accurate location of the targeting muscle, and the initial treatment should be at a reduced dosage.
Another factor that should be considered is that large doses and repetitive injections of BoNT create antibodies, leading to inadequate treatment outcomes [6,7,8,9][6][7][8][9]. According to previous research, antibody formation differs with types of botulinum neurotoxin [10,11][10][11].
Numerous studies on BoNT injection points in muscles have previously been published on external anatomical standards (Figure 2) [12,13,14,15,16,17,18,19,20,21,22,23,24][12][13][14][15][16][17][18][19][20][21][22][23][24]. WSe searchedarching for articles using the following keywords: “botulinum neurotoxin in nose region” and “side effect of botulinum neurotoxin injection in nose wrinkle” on Pubmed and Scopus. A total of 16 articles and two textbooks were found; 10 articles were excluded owing to the irrelevance to this studies. The objective of this study is to propose a safe and efficient BoNT injection point and suggest injective techniques for wrinkles in the nasal region.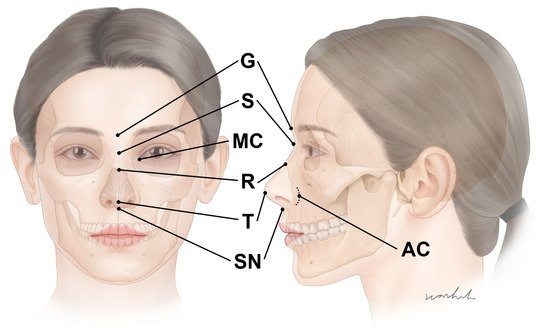
Figure 2. The external anatomical landmarks of the nose regions. G—glabella; S—sellion; R—rhinion; T—nose tip; SN—subnasale; MC—medial canthus; AC—alar crease.
2. The Anatomy of the Muscles in the Nasal Region
The schematic and dissected images of the muscles in the nasal region are presented below (Figure 3 and Figure 4).
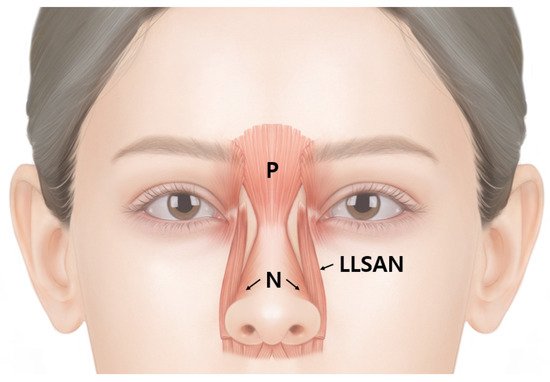
Figure 3.
Schematic image of the procerus (P), nasalis (N), and levator labii superioris alaeque nasi (LLSAN).
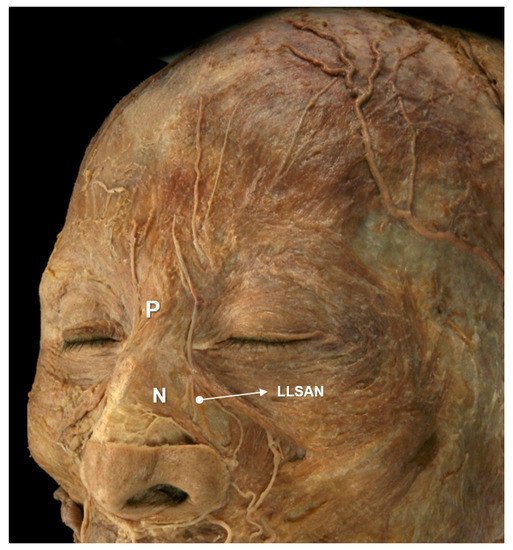
Figure 4.
The dissected image of the procerus (P), nasalis (N), and levator labii superioris alaeque nasi (LLSAN).
2.1. Nasalis Muscle
The nasalis muscle is composed of transverse and alar parts [25]. The transverse part of the nasalis muscle is a morphologically triangular structure originating from the maxillary canine fossa which inserts into the lateral cartilage of the nose [26]. The alar part of the nasalis is a square-like muscle that originates from the maxillary lateral incisor and inserts into the lower alar cartilage [26]. These two parts of the nasalis muscle both contribute to the narrowing of the nostrils. However, the transverse muscle contracts the nasal aperture while the alar muscle widens the nostrils.
2.2. Procerus Muscle
The procerus muscle originates deep from the lateral cartilage of the nose and nasal bone, inserting superficially into the skin at the glabella and radix [27]. In the glabella, the muscle fibers of the procerus muscle combine with the frontalis muscle [28]. The procerus muscle acts by pulling down the medial portion of the eyebrow while creating a transverse wrinkle between the glabella and the sellion.
2.3. Levator Labii Superioris Alaeque Nasi Muscle
The levator labii superioris alaeque nasi muscle is a long running muscle originating in the maxillary frontal process, and involves the nasal ala and upper lip [29]. The levator labii superioris alaeque nasi muscle can be divided into deep and superficial bellies [30]. The deep belly runs deep to the levator labii superioris muscle, whereas the superficial belly runs superficial to the levator labii superioris muscle [29].
3. Injection Techniques
3.1. Horizontal Radix Line
The horizontal radix lines are mainly caused by the procerus muscle; thereby, targeting the procerus muscle is the critical injection point. A dose of 2 U should be injected into the nasal dorsum. An accurate point should be located in the middle of the glabella and sellion. The glabella is the midline bony prominence between the frontal bone and supraciliary arches. In addition, the glabella presents the most anterior part of the forehead (Figure 2). The sellion is located at the midline of the base of the nasal root. It is the most posteriorly located landmark of the frontonasal contour (Figure 2) [31].3.2. Nasal Side Wall Scrunch Wrinkles (Vertical Lines)
Scrunch wrinkles on the nasal side wall are affected by the transverse part of the nasalis muscle. A dose of 2 U should be injected into the superior ala of the nose on both sides. The injection should be conducted in the middle of the rhinion and the medial end of the supra-alar crease (Figure 5).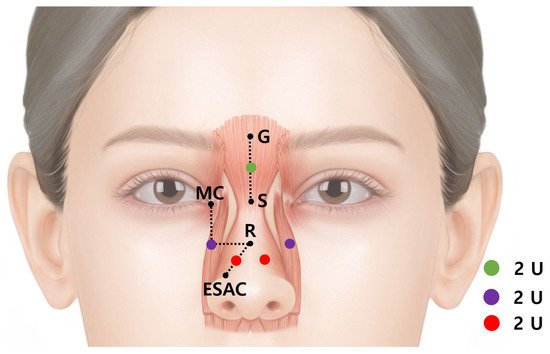
Figure 5. The injection point for the horizontal radix line (green dot) is in middle of the glabella (G) and sellion (S); for the nasal side crunch scrunch wrinkles (red dots), it is in the middle of the rhinion (R) and the medial end of the supra-alar crease (ESAC); and for the bunny lines (purple dots) it is at the crossing point of the horizontal line at the level of the rhinion and the vertical line at the level of the medial canthus; 2 Units of botulinum neurotoxins should be injected per point.
3.3. Bunny Line (Oblique Nose Furrows)
The bunny lines are oblique wrinkles on both sides of the nose dorsum at a 45° angle. The lines are caused primarily by the levator labii superioris alaeque nasi muscle and secondarily by the medial muscular band of the orbicularis oculi muscle. A dose of 2 U should be injected into the upper part of the levator labii superioris alaeque nasi muscle on each side. The injection should be conducted at the crossing point of the horizontal line at the level of the rhinion and the vertical line at the level of the medial canthus (Figure 5).References
- Dessy, L.A.; Mazzocchi, M.; Rubino, C.; Mazzarello, V.; Spissu, N.; Scuderi, N. An Objective Assessment of Botulinum Toxin A Effect on Superficial Skin Texture. Ann. Plast. Surg. 2007, 58, 469–473.
- Childers, M.K. Targeting the Neuromuscular Junction in Skeletal Muscles. Am. J. Phys. Med. Rehabil. 2004, 83, S38–S44.
- Wutthiphan, S.; Kowal, L.; O’Day, J.; Jones, S.; Price, J. Diplopia following subcutaneous injections of botulinum A toxin for facial spasms. J. Pediatr. Ophthalmol. Strabismus 1997, 34, 229–234.
- Chen, C.S.; Miller, N.R. Botulinum toxin injection causing lateral rectus palsy. Br. J. Ophthalmol. 2007, 91, 843.
- Aristodemou, P.; Watt, L.; Baldwin, C.; Hugkulstone, C. Diplopia Associated with the Cosmetic Use of Botulinum Toxin A for Facial Rejuvenation. Ophthalmic Plast. Reconstr. Surg. 2006, 22, 134–136.
- Hsu, T.S.J.; Dover, J.S.; Arndt, K.A. Effect of Volume and Concentration on the Diffusion of Botulinum Exotoxin A. Arch. Dermatol. 2004, 140, 1351–1354.
- Kinnett, D. Botulinum toxin A injections in children: Technique and dosing issues. Am. J. Phys. Med. Rehabil. 2004, 83, S59–S64.
- Lepage, D.; Parratte, B.; Tatu, L.; Vuiller, F.; Monnier, G. Extra- and intramuscular nerve supply of the muscles of the anterior antebrachial compartment: Applications for selective neurotomy and for botulinum toxin injection. Surg. Radiol. Anat. 2005, 27, 420–430.
- Pingel, J.; Nielsen, M.S.; Lauridsen, T.; Rix, K.R.; Bech, M.; Alkjær, T.; Andersen, I.T.; Nielsen, J.B.; Feidenhansl, R. Injection of high dose botulinum-toxin A leads to impaired skeletal muscle function and damage of the fibrilar and non-fibrilar structures. Sci. Rep. 2017, 7, 14746.
- Bellows, S.; Jankovic, J. Immunogenicity Associated with Botulinum Toxin Treatment. Toxins 2019, 11, 491.
- Campanati, A.; Giuliodori, K.; Martina, E.; Giuliano, A.; Ganzetti, G.; Offidani, A. Onabotulinumtoxin type A (Botox((R))) versus Incobotulinumtoxin type A (Xeomin((R))) in the treatment of focal idiopathic palmar hyperhidrosis: Results of a com-parative double-blind clinical trial. J. Neural. Transm. 2014, 121, 21–26.
- Yi, K.-H.; Cong, L.; Bae, J.-H.; Park, E.-S.; Rha, D.-W.; Kim, H.-J. Neuromuscular structure of the tibialis anterior muscle for functional electrical stimulation. Surg. Radiol. Anat. 2017, 39, 77–83.
- Yi, K.-H.; Rha, D.-W.; Lee, S.C.; Cong, L.; Lee, H.-J.; Lee, Y.-W.; Kim, H.-J.; Hu, K.-S. Intramuscular nerve distribution pattern of ankle invertor muscles in human cadaver using Sihler stain. Muscle Nerve 2016, 53, 742–747.
- Rha, D.-W.; Yi, K.-H.; Park, E.S.; Park, C.; Kim, H.-J. Intramuscular nerve distribution of the hamstring muscles: Application to treating spasticity. Clin. Anat. 2016, 29, 746–751.
- Yi, K.; Choi, Y.; Cong, L.; Lee, K.; Hu, K.; Kim, H. Effective botulinum toxin injection guide for treatment of cervical dystonia. Clin. Anat. 2020, 33, 192–198.
- Yi, K.; Lee, H.; Lee, J.; Lee, K.; Kim, H. Effective botulinum neurotoxin injection in treating iliopsoas spasticity. Clin. Anat. 2021, 34, 431–436.
- Yi, K.; Lee, H.; Choi, Y.; Lee, K.; Lee, J.; Kim, H. Anatomical guide for botulinum neurotoxin injection: Application to cosmetic shoulder contouring, pain syndromes, and cervical dystonia. Clin. Anat. 2021, 34, 822–828.
- Yi, K.; Lee, K.; Lee, J.; Hu, H.; Lee, K.; Seo, K.K.; Kim, H. Guidelines for botulinum neurotoxin injections in piriformis syndrome. Clin. Anat. 2021, 34, 1028–1034.
- Yi, K.-H.; Lee, H.-J.; Lee, J.-H.; Seo, K.; Kim, H.-J. Application of Botulinum Neurotoxin Injections in TRAM Flap for Breast Reconstruction: Intramuscular Neural Arborization of the Rectus Abdominis Muscle. Toxins 2021, 13, 269.
- Yi, K.-H.; Lee, J.-H.; Lee, D.K.; Hu, H.-W.; Seo, K.K.; Kim, H.-J. Anatomical locations of the motor endplates of sartorius muscle for botulinum toxin injections in treatment of muscle spasticity. Surg. Radiol. Anat. 2021, 43, 2025–2030.
- Yi, K.H.; Lee, J.H.; Kim, H.J. Intramuscular Neural Distribution of the Serratus Anterior Muscle: Regarding Botulinum Neu-rotoxin Injection for Treating Myofascial Pain Syndrome. Toxins 2022, 14, 271.
- Yi, K.-H.; Lee, J.-H.; Hu, H.-W.; Kim, H.-J. Anatomical Proposal for Botulinum Neurotoxin Injection for Glabellar Frown Lines. Toxins 2022, 14, 268.
- Yi, K.-H.; Lee, H.-J.; Seo, K.K.; Kim, H.-J. Intramuscular Neural Arborization of the Latissimus Dorsi Muscle: Application of Botulinum Neurotoxin Injection in Flap Reconstruction. Toxins 2022, 14, 107.
- Jeong, J.; Terence, G.; Kim, J. Understanding the Anatomy of the Transverse Nasalis Aponeurotic Fibers and Its Importance in Asian Rhinoplasty. Ann. Plast. Surg. 2018, 81, 516–522.
- Hur, M.-S.; Hu, K.-S.; Youn, K.-H.; Song, W.-C.; Abe, S.; Kim, H.-J. New anatomical profile of the nasal musculature: Dilator naris vestibularis, dilator naris anterior, and alar part of the nasalis. Clin. Anat. 2011, 24, 162–167.
- Starkman, S.J.; Sherris, D.A. Association of Corrugator Supercilii and Procerus Myectomy With Endoscopic Browlift Outcomes. JAMA Fac. Plast. Surg. 2019, 21, 375–380.
- Hwang, K.; Jin, S.; Park, J.H.; Chung, I.H. Innervation of the Procerus Muscle. J. Craniofacial Surg. 2006, 17, 484–486.
- Hur, M.S.; Hu, K.S.; Park, J.T.; Youn, K.H.; Kim, H.J. New anatomical insight of the levator labii superioris alaeque nasi and the transverse part of the nasalis. Surg. Radiol. Anat. 2010, 32, 753–756.
- Hur, M.-S. Anatomical relationships of the procerus with the nasal ala and the nasal muscles: Transverse part of the nasalis and levator labii superioris alaeque nasi. Surg. Radiol. Anat. 2017, 39, 865–869.
- Katina, S.; McNeil, K.; Ayoub, A.; Guilfoyle, B.; Khambay, B.; Siebert, P.; Sukno, F.; Rojas, M.; Vittert, L.; Waddington, J.; et al. The definitions of three-dimensional landmarks on the human face: An interdisciplinary view. J. Anat. 2016, 228, 355–365.
- Kothari, M.; Shukri, N.; Quayyum, A. Transient superior oblique paresis after injection of Botulinum Toxin A for facial reju-venation. Indian J. Ophthalmol. 2012, 60, 77–78.
More