1. AdvRheumances in Characterizing the Global Burden of tic Heart Disease and Rheumatic Heart DiseasFever: A Historical Context
1.1. Introduction
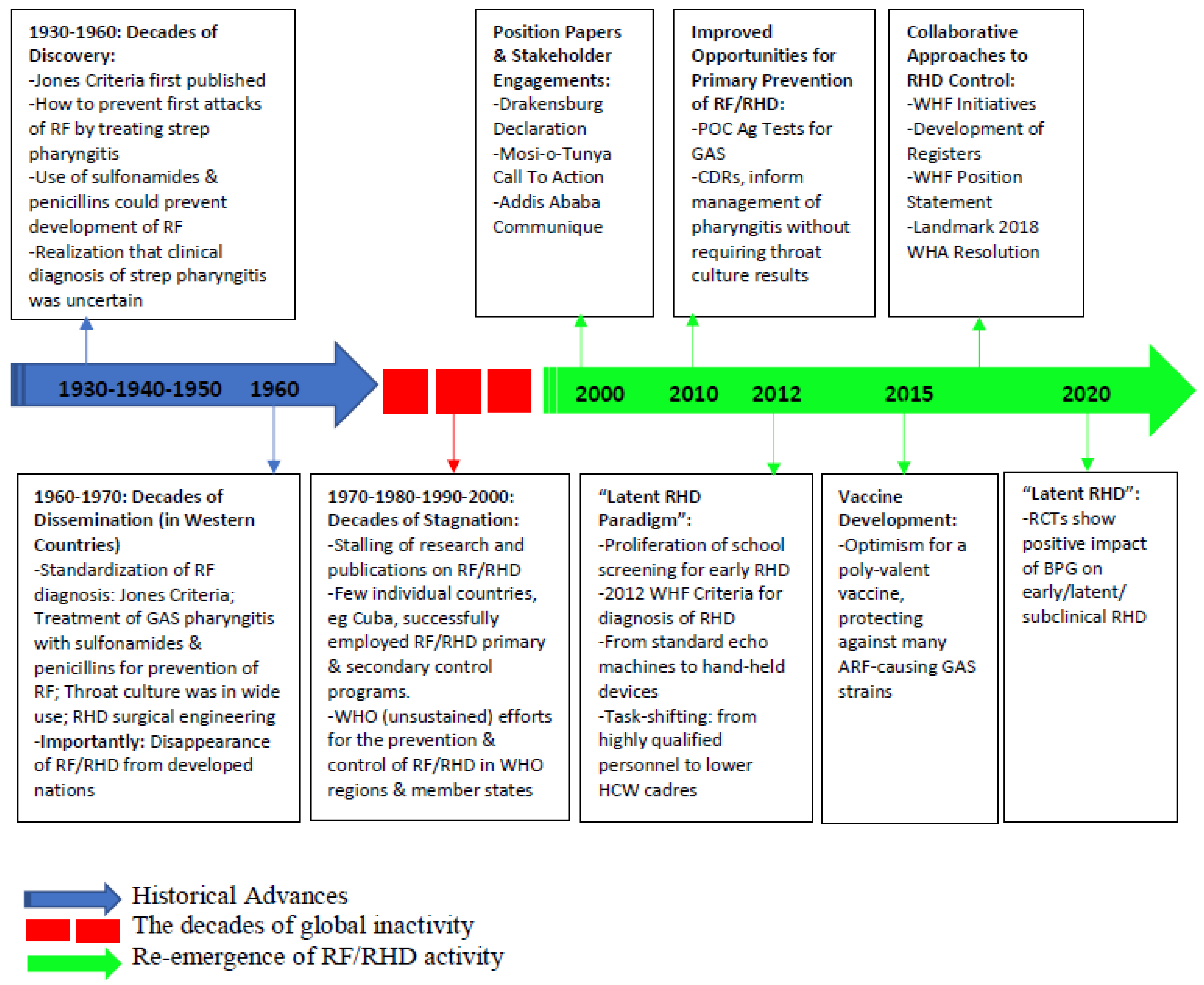
The history of rheumatic heart disease (RHD) and rheumatic fever (RF) control is a mixture of remarkable advances and frustrating gaps in scientific and public health progress. Much of what we know today about the pathogenesis, diagnosis, prevention, and treatment of this disease continuum originates from what are now considered high-income countries in the mid-20th century, where improved socioeconomic standards and access to healthcare (boosted by extensive biomedical research) resulted in a striking reduction of disease burden. Once the disorder was all but wiped out from high-income nations, however, it receded from public and academic attention, leading to a stagnation in control in low-and middle-income countries (LMICs). This period lasted for nearly a generation, but the past two decades have seen a reemergence of global RHD research and advocacy, which has largely been grassroots, conducted in low-resource settings in populations where RHD remains endemic. Figure 1 provides an overview of these sequential phases, which we discuss in greater detail in the subsequent sections.
Figure 1. Timeline of advances in global RF/RHD control. Abbreviations: GAS, group A Streptococcus; RF, rheumatic fever; ARF, acute rheumatic fever; RHD, rheumatic heart disease; POC, point of care; Ag, antigen; CDR, clinical decision rule; BPG, benzyl benzathine penicillin; HCW, health care worker; RCT, randomized clinical trial; WHA, World Health Assembly; WHF, World Heart Federation; WHO, World Health Organization.
1.1. Decades of Discovery: 1930s–1950s
Concurrent with the growth and advancement of the discipline of microbiology, Streptococcus [1], and shortly thereafter, Streptococcus pyogenes (group A
strep, GAS), were first iden
utified during the ‘golden age of bacteriology’ [2] in the late 19th and early 20th century. Sim
ultaneously, RF was gaining attention as the leading cause of death among individuals be
r otween 5 and 20 years, even in nations now considered to be high-income countries [3,4], with the critical link between RF and GAS established by 1889 [5]. By 1944, the diagnosis of
RF was standardized by Dr. T. Duckett Jones, (The Jones Criteria [6,7,8]), although treatment remained limited to salicylates and bedrest [4]. By the 1950s, antibiotics became even more widely available [9,10] and strong evidence emerged that proper treatment of
GAS pha
ryngitis, both with sulfonamides [4,9] and penic
illins [11], could prevent
the develo
pment of RF [4,12,13,14]. Thus, the utility of secondary antibiotic pr
ophylaxis
over the to prevent RF recurrence was established [15,16,17], with long-acting intramuscular formulations develop
ed [18], a
nd a monthly adminis
t dectration of this medication was found to effectively suppress RF recurrences [16,19,20,21,22]. Monthly injections of intra
muscular long-acting benzathine penicillin G (BPG) were subsequently shown to be superior to d
e haaily oral penicillin G in the prevention of streptococcal infections and recurrences of RF [23], establishing a key tenet of RHD management which is still accepted as dogma today. In addition to the medical management of RHD, this time period was also an era of significant pioneering in the surgical management of v
alvular RHD seque
dramaticalllae. For example, the first recorded valvotomy for aN RHD patient was performed at the House of the Good Samaritan (HGS), an RF/RHD specialty hospital, in 1923 [4].
1.2. Decades of Dissemination: 1960s–1970s
While improved living conditions in high-resource settings (less household crowding, better personal hy
giene, and improved
opublic health infrastructure) drove down the incidence of RF even before many of the scientific advances described above were realized [24,25,26], targeted advocacy, edu
cation, and awar
abileness of the diseases in the second half of the 20th century further accelerated progress toward eradication. Among the leading advocates of such measures was the American Heart Association, which had largely coalesced to fight what it dubbed ‘Childhood’s Greatest Enemy' [27]. By the 1970s, the annual i
ncidence of RF in t
yhe United States had plummeted to 0.6 per 100,000 population in those aged 5 to 19 years [28,29], Similar gains were seen during this t
o estimate thime in other high-income countries (much of Europe and Australia), and in some isolated lower income countries (such as Cuba [25] and Costa Rica [30]) which impleme
nted prevaicomprehensive RF prevention programs without the benefit of improved socio-economic conditions at that point in time.
1.3. Decades of Stagnation: 1970s–2000s
Fol
lowing
b this period of rapid advancement, RF and RHD were largely controlled in high-income countries. As such, appetite for new research (and funding for such research) in RF/RHD largely dissipated. Regrettably, this waning of interest and investigative efforts [31] only reflected the redu
ction in RF/RHD burden
of among a fraction of the world’s population. More unfortunately, those left behind represented those at highest social risk for developing--and suffering adverse outcomes from--the disese. During this period, the World Health Organization (WHO) briefly invested in a large-scale program to disseminate knowledge and best practices around the globe [32,33,34,35,36]. However, these efforts were not sustained, as the problem of R
F/RHD was progressively oversh
eumatic heart Disease adowed and ultimately dwarfed by the epidemics of malaria, tuberculosis, yellow fever, and especially—HIV/AIDS. Consequently, despite the persistent burden (and known interventions known to reduce this burden) of RF/RHD, it was steadily relegated to the status of a ‘neglected tropical disease’.
1.4. A Renewal of Attention: 2000s to Present
The last two decades, however, have seen an encouraging resurgence of interest in RF/RHD. This has, in large part, been due to both the growth of global health as a discipline as well as the development of cardiac imaging technologies suited for use in low-resource settings. In particular, echocardiography ultrasound devices have become cheaper, lighter, and more portable (
by incorporating small-form factors and rechargeable battery power supplies), resulting in their use to unmask a substantial number of children and adults living with previously-undiagnosed RHD
) in LMICs [37,38,39,40,41]. This has provided irrefutable evidence of the persistent and disparate global burden of the ongoing RHD epidemic. In response, calls to action began to emerge from research groups and professional societies [31,42,43], particularly in sub-Saharan Africa, were regional meetings were convened and produced critical position papers and guiding statements to drive the global RHD control agenda [44,45,46]. These, among other regional academic and advocacy efforts, were crowned by the 2018 World Health Assembly Resolution to end RHD [47]. In response, global research and funding opportunities have steadily increased, particularly calls for action to apply exciting modern technologies and research methodologies to build new knowledge in the RHD management cascade.
2. Advances in Characterizing the Global Burden of RHD
A number of factors over the past decade have dramatically improved our ability to estimate the prevailing burden of RHD, with estimates ranging from 15 million cases in 2005
[1][48] increasing to 40.5 million estimated cases in 2019 with refinement in epidemiologic methodology
[2][49]. More granularly, however, individual nation-level studies have shown shifting prevalences even within LMICs. Echocardiographic surveys in some settings such as in India have revealed consistent decline in the burden of RHD before and after 2000, using similar screening methods among school children. This particular decline was associated with improvement in the indicators of socioeconomic state and health-care services. Three main advances have led to the knowledge gain of the global burden of RHD, including (a) screening echocardiography; (b) RHD registries and country-wide administrative health data; and (c) big data sources, namely the Global Burden of Disease repository.
1.1. Advances in Screening Echocardiography
2.1. Advances in Screening Echocardiography
RHD remains largely clinically silent until patients become symptomatic with the advanced form of disease. Echocardiographic (echo) screening
[3][37], which has been one of the chief advancements in our understanding of the global burden of RHD, has resulted from school, community, and clinical echo screening to define the epidemiological burden of the disease. In particular, echo screening is responsible for the birth of the ‘latent RHD’ paradigm (namely the identification of subclinical echo-detected disease)—rallied as an opportunity for early intervention to prevent disease progression. Active case finding through echo screening has gained further traction in the past decade particularly following the publication of standardized diagnostic criteria by the World Heart Federation (WHF) in 2012
[4][50]. The value of echo screening in the control of RHD has been a subject of debate
[5][51] in recent years
[6][52]. Nevertheless, robust data from a landmark randomized-controlled trial strongly suggest that secondary antibiotic prophylaxis prevents the progression of latent RHD to moderate or severe stages of disease, thus supporting the clinical need for screening, even among asymptomatic individuals
[7][53].
Key developments toward pragmatic echocardiographic screening capacity in LMICs have included: (a) development of handheld echo devices which are less expensive, generate smaller and shareable file sizes, and have a smaller profile without reliance on wired electricity
[5][51]; (b) task-shifting of echo image acquisition from highly trained cardiologists and licensed sonographers to other healthcare workers such as nurses, allowing for expansion of screening capabilities; (c) supportive cloud-based telemedicine programs for remote echo image interpretation; and finally, (d) expanding technological advances
[8][9][54,55], with several companies now offering artificial intelligence guidance technology built into hand-held devices, thus empowering novice operators to perform screening echoes even after only minimal training, and promising deep learning approaches for automated flagging of abnormalities in the near future
[10][56]. There is also an ongoing effort to improve and simplify the WHF criteria for the diagnosis of latent RHD
[11][57], with additional development of risk scores to predict outcomes in both borderline and definite latent RHD
[11][57].
1.2. Establishment of RHD Registries and Big Data Resources
2.2. Establishment of RHD Registries and Big Data Resources
With the increasing interest in meeting the RHD challenge in endemic countries, a number of large disease-specific registries have been established in LMICs. These have illuminated the dire epidemiologic situation of clinical RHD in these settings
[2][12][13][49,58,59]. The hospital-based sub-Saharan Africa Survey of Heart Failure (THESUS-HF) registry study showed that RHD was the second major cause of acute heart failure hospitalizations, with an inpatient mortality rate of 4.2% and a 180-day mortality rate of 17.8%
[14][60]. The VALVAFRIC
[15][61], REMEDY
[16][62], and certain national
[17][18][63,64] registry studies provide the most recent descriptions of chronic RHD complications in patients residing in low- and middle-income countries. In general, they have established that clinical RHD in LMICs is characterized by late presentation with substantial established complications
[17][18][63,64]. The clinical course is thus punctuated by recurrent hospitalizations and unacceptably early mortality (mean age at death of 29.4 years), with most of these deaths occurring within the first three months following diagnosis.
On the global scale, contemporary surveys continue to reveal worldwide RHD disparities, with low-income countries bearing a disproportionate burden of the disease. RHD currently affects 40.5 million people across the globe and accounts for 306,000 deaths annually—representing 1.6% of all mortality from cardiovascular disease, the leading cause of death worldwide
[2][49]. The increased prevalence of RHD detected in recent studies, when compared to historical surveys, is most likely related to improved case detection attributable to the increased availability of echocardiography, better survival of affected individuals, and the chronic nature of the disease
[2][49]. Sub-Saharan Africa retains the highest prevalence of clinically-apparent RHD
[19][65], and there is some evidence that the true burden of RHD in some African countries may be much higher than previous estimates
[20][66]. Today, the highest age-standardized disability-adjusted life year (DALY) rates attributable to RHD are in the regions of Oceania (627.4 per 100,000) and South Asia (348.5 per 100,000). In Australia and New Zealand, the highest rates of RF and RHD are found among indigenous populations
[21][22][67,68]. Unfortunately, epidemiological data on RHD prevalence is least robust from the most affected regions
[23][69]. National, regional and global RHD registries continue to report female predominance, however no gender-based differences in complications such as heart failure, atrial fibrillation, stroke and pulmonary hypertension have been noted.
2
3. Advances in Elucidating the Pathogenesis of RF/RHD
The general academic consensus remains that an immune-mediated pathologic process is the hallmark of RHD. Nevertheless, the exact mechanisms underlying this complex process have yet to be completely unveiled. Traditional dogma has held that GAS pharyngitis is responsible for triggering the immune reaction that leads to RHD pathology
[24][70]. However, more recently, other superficial streptococcal infections, such as impetigo and pyoderma, have been found to be associated with RHD
[25][26][71,72]. There is also emerging evidence potentially implicating group C and group G streptococcus in contributing to the pathogenesis of RHD
[27][28][29][30][31][73,74,75,76,77].
The most widely accepted hypothesis in the pathogenesis of RF/RHD
[32][33][78,79] is that molecular mimicry is responsible for the autoimmune phenomena of the disease, but more recent data suggests a more complex cascade of events, such as collagen-associated neo-antigens
[34][35][80,81] epitope spreading
[36][82], and T-cell receptor (TCR) degeneracy
[37][38][39][83,84,85] may participate in the resultant pathology. Additionally, specific CD4+ T cells, as well as NK cells and CD4-CD8- T cells, might be important players in cardiac tissue destruction seen in RHD
[40][86]. Recent efforts have been developed to take advantage of the intense GAS antigen-associated immune response for the creation of RF/RHD vaccines, but these have remained elusive largely due to lack of academic and financial investment
[41][87]. Dissecting the immunopathogenic responses using state-of-the-art methods such as single cell RNA sequencing combined with TCR CDR3 region usage may open new insights to advance this field.
Furth
4. Advances in Understanding the Genetic Predisposition to RF/RHD
De
rmore, despite the widespread socioeconomic risk factors for RHD development present in LMICs, only a minority (roughly 3–6%) of GAS-endemic populations develop RF
[24][70]. Furthermore, RHD is largely believed to have a complex genetic risk profile
[42][88]. Historical RHD studies in twins have supported this postulation
[43][44][89,90], and more recent modern genetic interrogation studies have she new light on RHD pathogenesis and predisposition.
Genetic associations in RHD have been explored through numerous candidate gene studies—for example, those reviewed by Martin et al.
[45][91] and Muhamed et al.
[46][92] elicited genetic associations in RHD through candidate gene studies. These have yielded conflicting and heterogeneous results, implicating a variety of genes with several listed study limitations
[43][45][46][89,91,92] including those that have reported the association of human leukocyte antigen (HLA) molecules, encoded by genes on chromosome 6, and susceptibility to developing RF/RHD
[43][47][48][49][50][51][89,93,94,95,96,97]. Within HLA genes, class II genes have been widely reported, with the majority linking HLA-DR7
[43][50][89,96] and HLA-DR4
[45][49][52][91,95,98] to the development of RHD.
There has also been interest in evaluating genetic polymorphisms coding for inflammatory mediators in RHD and their phenotypic expression. Polymorphisms in IL-2, IL-4, IL-6 and IL-10 genes have been associated with clinical disease, and the discriminative value of IL-4 to differentiate latent versus clinical RHD has been demonstrated
[53][99]. Additionally, interleukins IL-4, IL-8 and IL-1RA seem to predict progression from latent to clinical RHD, while in individuals with advanced RHD, co-regulated expression of IL-6 and TNF-α are associated with severe valvular dysfunction, with higher IL-10 and IL-4 levels predicting adverse clinical outcomes
[54][100].
The biggest advance in the field of RHD genetics has been genome-wide association studies (GWAS), of which four major studies have been published to date (
Table 1)
[47][55][56][57][93,101,102,103]. GWAS are considered more suitable studies for complex diseases in which large numbers of variants can be tested by comparing single-nucleotide polymorphism (SNP) distributions in patients with the disease against selected controls
[58][104].
cell wall, have not shown expressive results yet
[60][110].
These GWAS studies have generated support for the presence of significant heritability in RHD, which is likely to be polygenic. The RhEumatiC Heart diseAse Genetics (RECHARGE) study is ongoing in Rwanda, using next-generation genetic sequencing on a sample of approximately 1000 participants (ClinicalTrials.gov Identifier: NCT02118818). It is expected to be completed in 2024. The importance of investing resources in the genetic association of RHD lies not just in the potential to substantially contribute towards understanding disease pathogenesis and etiology, but also the prospect of identifying novel or repurposed therapeutics and vaccine development
[46][92].
3
5. Advances in Management of Esthe ablished Disease in the RF/RHD Continuum
3.1. Progress Towards a Group A Streptococcus Vaccine
Even though RHD is, in theory, preventable, advances in prevention of RHD in low-resource settings has been slow. Nevertheless, the past decade has seen a revived dedication and commitment to further developing best clinical practices at the primordial, primary, secondary and tertiary levels of prevention. The search for a safe and effective GAS vaccine continues, and this will likely form the monumental advance that will deal the final blow to RF/RHD in all regions of the world, regardless of prevailing socioeconomic and health system determinants.
5.1. Advances in Primordial Prevention
Recent studies have aimed to provide a better description of the influence of socioeconomic determinants, healthcare system factors, and transmission dynamics of GAS responsible for actionable interventions for RHD prevention. Household crowding has been shown to have the strongest evidence of association with GAS infection and ARF/ RHD, increasing the risk by 1.7- to 2.8-fold. Dwelling characteristics such as construction type, house condition, dampness, and ventilation are also associated with an increased risk of GAS infection that ranges from 1.8 to 3.6-fold [105]. The greater risk of having RHD among first-degree relatives of individuals with clinical RHD may be secondary to the shared socioeconomic conditions [106,107]. Approaches targeting these primordial determinants have been designed and are being implemented via a community approach in Australia [108].
Group A Streptococcus Vaccines
Efforts to create a vaccine to prevent GAS infections have been ongoing since 1923. However, the first vaccines were ineffective and highly reactogenic, raising concerns, though likely unfounded or overblown, about the potential for vaccines to increase ARF predisposition; this resulted in the US Food and Drug Administration (FDA) stopping GAS vaccine trials in the 1970s for over 30 years
[59][60][109,110]. In the past two decades, studies on vaccine development have improved with advances in genomics, proteomics, and immunomics; still, most vaccines are in pre-clinical testing, and few have reached Phase I and II trials. Currently, there are no licensed vaccines of GAS available in any settings
[60][110].
Vaccine candidates, however, include multivalent M protein-based vaccines, M protein vaccines containing conserved C-repeat epitopes, cell wall carbohydrate vaccines, and non-M protein multi-component vaccines. Table 12 provides a summary of vaccines that are in the development pipeline. Vaccines based on group A carbohydrate (GAC), a polysaccharide present in Streptococcus pyogenes
Prevailing challenges in vaccine development are multifactorial, ranging from incomplete understanding of the basic science of GAS/RF/RHD to lack of commercial stakeholder interest. Specific challenges for GAS vaccine development include: (a) extensive genomic heterogenicity of Strep A and subsequent protein sequence variations, limiting the effectiveness of the vaccine over different populations
[60][110]; (b) complexity of global GAS epidemiology; (c) incomplete understanding of ARF pathogenesis; (d) risk of serious autoimmune reactions to vaccines
[59][109]; (e) dependence on controlled human infection models for vaccine development as GAS is strictly a human pathogen, thus precluding the use of animal models
[66][111]; (f) lack of consensus on clinical endpoints for establishment of proof of concept, (g) limited market in high-income countries; and h) lack of commercial interest
[60][110].
In order to overcome the myriad challenges in GAS vaccine development, in 2018 the World Health Assembly (WHA) launched a Global Resolution calling for improved control and prevention of GAS infections and RHD
[67][112]. In 2019, the Strep A Vaccine Consortium (SAVAC) was formed to work along the World Health Organization (WHO)
[60][110]. Furthermore, through the Coalition to Advance Vaccines Against Group A Streptococcus (CANVAS), the Australian and New Zealand governments have designated significant funding to support the development of a vaccine against GAS pharyngitis
[68][113].
3.2. Advances in Primary Prevention
5.2. Advances in Primary Prevention
5.2.1. Diagnosis of Group A Strep Pharyngitis
Microbiological culture of a throat swab remains the gold standard for diagnosing GAS pharyngitis, despite the prohibitive cost of this modality at a population level, the long turn-around time precluding confirmed diagnosis in a single clinic visit, and lack of readily available culture-able laboratories in LMICs. Recognizing these limitations, alternative diagnostic tests which are less resource-intensive have been developed and continue to evolve.
Clinical decision rules can obviate the need for expensive bacteriological diagnostic tools since they do not require specialized equipment and are easy for providers to implement
[69][70][71][119,120,121]. There has been a proliferation of Clinical Decision Rules (CDRs) for diagnosis of GAS pharyngitis in recent years
[69][70][72][73][74][75][76][77][119,120,122,123,124,125,126,127]. Recent developments relevant to RHD endemic regions include: (a) validation studies of existing CDRs in RHD endemic regions
[78][128] that have concluded that diagnostic performance varies considerably in different regions of the world, thus highlighting the importance of evaluating and validating CDRs in local settings before they are rolled out as the standard of care; and, (b) development of CDRs in RHD endemic regions such as the Cape Town Clinical Decision Rule
[69][119] in South Africa. The Cape Town Clinical Decision Rule is likely a more relevant application to similar settings in sub-Saharan Africa. Tailoring decision rules to a specific population is a critical research area for population specific investment in LMICs.
Rapid Antigen Detection Tests (RADTs) have been in clinical use for four decades, with attractive features such as a quick turn-around time (<10 min), low cost, and ease of use. Recently,
we have learned that some external performance factors
were learned, such as inadequate staff training, substantially reduce the accuracy of these tests
[79][129]. There is also greater understanding of factors that potentially increase heterogeneity of testing results that have similar sensitivity and specificity
[80][130] such as differences in throat culture sample collection
[80][81][130,131], experience of the person performing the RADT, absence of a universally accepted blood agar plate culture method to serve as a reference standard
[82][132], patient-level characteristics such as clinical presentation and inoculum size
[83][133], and spectrum bias
[84][134]. However, despite multiple advantages, RADTs remain vastly unavailable and are considered expensive for many low-resource settings. There is an overarching need to make existing RADTs available and affordable for use in such settings.
More recent progress in point-of-care tests for GAS pharyngitis include Nucleic Acid Amplification Tests (NAATs), which have much better sensitivity and specificity than RADTs
[85][135]. For example, the sensitivity and specificity of the Illumigene assay are estimated to be in excess of 99%
[85][86][87][135,136,137]. This high performance, coupled with speed of results, makes NAATs ideal candidates for point-of-care use in the clinical environment. Several NAATs have received approval over the past six years
[88][138], but their high cost has precluded widespread use. Despite the prevailing cost, NAATs are being increasingly investigated as low-cost, integrated tools for use in low resource settings
[89][90][139,140]. Research should strive towards the development of molecular diagnostic tests using a “pharyngitis panel” of targets.
Electrochemical detection methods, which use DNA, have been proposed as an affordable, effective method for diagnosing GAS; results are available in 30 minutes with 100% specificity, have been reported
[91][92][141,142].
Machine learning and artificial intelligence techniques are also in development to aid in the diagnosis of strep throat through throat image processing
[93][143] and automated examination of throat cultures to identify GAS
[94][144]. Neural networks have also been suggested to assist in diagnosis, with reported correct diagnosis of pharyngitis in 95.4% of test cases in one study
[95][145]. The Strepic
® device, a qualitative point-of-care clinical prototype, has been designed specifically as a viable, low-cost, commercially realizable autofluorescence-based diagnostic test (ClinicalTrials.gov Identifier: NCT03777098).
5.2.2. Treatment of Group A Strep Pharyngitis
Penicillin remains the first line recommendation for the treatment of GAS pharyngitis, with two Cochrane reviews supporting this recommendation
[96][97][146,147]. Monthly intramuscular injections of benzathine benzyl penicillin (BPG) remain the gold standard for secondary antibiotic prophylaxis for the prevention of RHD
[98][99][148,149]. Recent strategies to diminish pain
[100][150] associated with BPG administration include the addition of lidocaine to BPG solution
[101][102][151,152] and the use of pain distraction methods (buzzy R)
[102][103][104][105][152,153,154,155]. There is also work underway in developing implantable and longer acting BPG delivery devices
[106][107][108][156,157,158]. The WHO added BPG to the essential medicines list for member states as a way to increase access, however, disruptions in global and local BPG supply chains are not uncommon
[109][110][159,160]. Regrettably, a recent report described geographically widespread reduced in-vitro susceptibility of
Streptococcus pyogenes to beta-lactam antibiotics associated with mutations in the pbp2× gene
[111][161], warranting enhanced surveillance and further epidemiological and molecular genetic study of this potential emergent antimicrobial threat.
Community and provider knowledge and awareness of the RHD-GAS relationship remain a pillar of primary prevention strategies. While previous awareness campaigns heavily utilized print and mass media
[112][113][114][36,162,163], increasing availability of sophisticated personal technologies such as mobile devices and internet access (particularly in low-resource settings), have resulted in the employment of new electronic avenues of patient, public, and stakeholder education about RHD
[115][164].
Additionally, it has been noted that streptococcal carriage rates often vary between communities and by season, especially in endemic countries
[116][117][165,166]. It has thus been postulated that the GAS carrier state is not implicated in the pathogenesis of RF/RHD, and that transmission of GAS is almost limited exclusively to individuals with acute GAS infection
[118][119][167,168]. Therefore, antibiotic treatment for eradication of GAS has been recommended only for individuals with acute GAS infection. However, this traditional benign dogma of the carrier state is being challenged and revisited, with additional investigation necessary to determine if this paradigm holds true in endemic regions of the globe.
3.3. Advances in Secondary Prevention
5.3. Advances in Secondary Prevention
The Jones criteria for the diagnosis for ARF were first established in 1944
[120][169]. Since their inception, the criteria have undergone multiple revisions and updates, most recently in 2015
[121][7]. This most recent revision addressed two significant features: it (a) distinguished criteria between low-risk and moderate-to-high risk populations based on ARF incidence or RHD prevalence; and (b) recommended echocardiography of all suspected cases of ARF and incorporated subclinical carditis as evidenced by echocardiography as a major criteria. Differentiating criteria for low-risk and moderate-to-high risk populations aimed to increase sensitivity in endemic regions while retaining specificity in low-risk areas, thus making the criteria more globally relevant. However, ARF still remains a clinical diagnosis with no single confirmatory test, and there is ongoing work attempting to identify a unique immune signature that could be used to reliably diagnose ARF
[122][170]. For example, in routine clinical practice it is often not feasible to obtain both acute and convalescent sera and therefore, the absolute quantitative measure of anti-streptolysin (ASO) titers is used more for diagnostic value
[123][171]. However, there is wide geographic variability of the 80th percentile upper limit of normal (ULN) cutoffs for ASO titers
[124][125][172,173]. It is therefore important to establish ULN ranges of ASO titers for various age groups in different geographic locations. Accordingly, there have been recent studies in some RHD endemic regions describing their population-specific streptococcal antibody titers
[126][174].
This is particularly relevant, because, as previously mentioned, there is recent evidence for the benefit of secondary penicillin prophylaxis for prevention of progressive cardiac disease in latent RHD
[7][53]. The recent GOAL trial demonstrated that among children and adolescents 5 to 17 years of age with latent RHD, secondary antibiotic prophylaxis reduced the risk of RHD progression at two years followup time
[7][53]. This new evidence provides added justification for echocardiographic screening and active case detection of RHD as a key step in the control of RHD sequelae in susceptible populations.
5.4. Procedural and Medical Advances in Tertiary Care
5.4.1. Surgical Management -- Valve Replacement vs. Valve Repair
3.4. Procedural and Medical Advances in Tertiary Care
Mitral valve (MV) repair, rather than replacement, is currently the preferred surgical management for patients with mitral regurgitation (MR) as evidence suggests better short and long-term outcomes [175,176,177,178], including shorter hospital stays and fewer infections [179]. However, MV repair requires refined surgical skills with an associated learning curve, adequate surgical environment, and echocardiographic guidance by an expert, in addition to relatively favorable valve anatomy. For these reasons, in low-income areas where RHD is prevalent, surgical teams often have more expertise in performing MV replacement, making it the first choice for surgical intervention in these settings [178].
Procedural Advances in RHD-Associated Valvular Disease
5.4.2. Operative Management -- From Surgical Valvotomy to Percutaneous Balloon Mitral Valvuloplasty (PBMV)
There is a growing body of evidence to support the use of PBMV for RHD-associated mitral stenosis, and the indications have considerably expanded in the past decade to include challenging and unfavorable MV involvement. Furthermore, additional prognostic parameters have been investigated—such as asymmetrical commissural fusion and atrioventricular compliance—and the Wilkins score has been updated with parameters derived from international RHD cohorts
[127][180]. Meanwhile, percutaneous valve interventions continue to evolve worldwide, with transcatheter aortic valve implantation for the treatment of aortic stenosis (more below) being a prime example of such advances
[128][181]. With its successful implementation, percutaneous valve intervention is gaining attention as a feasible treatment for both mitral and aortic valve disease, as well as an option for second valvular interventions after the failure of the primary valve surgery—common in RHD—with additional outcome information to be established in the upcoming decades
[129][130][182,183].
5.4.3. Transcatheter Management Innovations -- Transcatheter Aortic Valve Replacement (TAVR) for Rheumatic Aortic Stenosis
TAVR is an established minimally invasive alternative to surgical aortic valve replacement (SAVR) in patients with severe aortic stenosis (AS) and calcific aortic valve disease
[131][132][184,185]. In RHD with aortic involvement, SAVR is still the first choice of intervention due to the lower degree of valve calcification seen in rheumatic valves in most cases
[132][133][185,186], younger age of patients, and limited scientific evidence of TAVR for RHD-associated AS
[133][186]. Until recently, knowledge surrounding the application of TAVR for RHD patients was limited to case series and reports
[132][134][135][136][185,187,188,189]. However, there is contemporary evidence for non-inferiority of TAVR to SAVR in rheumatic AS, safety of TAVR, and short and intermediate term outcomes of TAVR
[132][135][185,188]. These novel data have changed the perspective of TAVR for RHD, suggesting it as a feasible approach for RHD patients with predominant aortic valve involvement. However, wider spectrum studies with larger subject numbers and long-term outcomes reports in RHD-specific patient populations are warranted in order to achieve generalization of such findings.
5.4.4. Advances in the Medical Management of Clinical RHD
Given the limitation of surgical treatment options for many patients with symptomatic RHD in low-income regions, medical management remains a critical cornerstone of therapy for those awaiting or unable to obtain operative management of advanced valvular RHD. Unfortunately, medical therapy to date has yet to demonstrate slowed progression of the disease. As such, pharmacologic treatment has targeted symptom relief by addressing underlying left ventricular dysfunction and heart failure or by addressing the end-stage complications of RHD
[137][178].
Atrial fibrillation (AF) is a major cause of morbidity and mortality in patients with RHD
[16][137][138][62,178,190]. Anticoagulation is recommended to reduce the risk of cardioembolic events in patients with AF, often associated with advancing valvular pathologies
[16][138][139][62,190,191]. Oral Vitamin K antagonists are the recommended drugs of choice for this purpose
[137][178], but they are associated with challenges both for health care providers and patients in monitoring and maintaining their effectiveness
[138][139][190,191]. New evidence may revolutionize anticoagulation in rheumatic atrial fibrillation, as novel oral anticoagulants (NOACs)—not yet formally recommended for AF in the presence of RHD—have proven to be non-inferior to warfarin in a Brazilian trial which allowed the inclusion of RHD patients with atrial fibrillation and bioprosthetic mitral valves
[140][192]. The multicenter INVICTUS trial
[141][193] examining warfarin versus rivaroxaban in rheumatic AF is nearing completion and may bring more definite conclusions in the near future. However, even if NOACs become a standard for anticoagulation in RHD, access and cost-effectiveness will require careful discussion for their use in LMICs, given the higher present market price of these drugs
[142][194].
Another chief clinical concern among advanced RHD patients remains that of infective endocarditis in both prosthetic valves and diseased native heart valves. Given the lack of scientific evidence in reducing infective endocarditis (IE) burden in the absence of prosthetic valves or previous history of IE, antibiotic prophylaxis for dental procedures has been relegated to a limited role in recent professional society guidelines
[143][195]. Currently, recommendations for such chemical prophylaxis is limited to high-risk patients—noticeably those following valve replacement or those with a previous IE episode—undergoing high-risk procedures with potential bacterial translocation
[144][196]. Good dental hygiene and regular dental cleanings, however, still play an important role in IE prevention and should be emphasized
[195].
6. Rheumatic Heart Disease in Pregnancy
Preexisting cardiac disease is a major contributor to maternal mortality worldwide, especially in LMICs [197]. Recognition of RHD in pregnancy is extremely important, especially given the higher prevalence of RHD [143]in women, particularly young women of reproductive age in LMICs [190], and the significant risk posed by RHD during pregnancy. Recent echocardiographic screening studies in sub-populations of pregnant women in RHD endemic regions have provided epidemiologic descriptions of the burden and outcomes of RHD in pregnancy [197,198], reinforcing the need for programs dedicated to early diagnosis and prioritization of cardiovascular care during family planning and pregnancy in RHD-endemic regions. Family planning with adequate preconception counseling should be provided to known RHD patients. However, that is often not the reality. For example, only 5% of women with prosthetic valves and 2% of women with severe mitral stenosis in the aforementioned REMEDY registry study reported being on a form of reproductive contraception [178]. Additionally, for pregnant women with primary indications for anticoagulation, particularly mechanical valves, management remains complex and challenging [178,190]. The ideal choice of bioprosthetic valves in women of childbearing potential to circumvent the need for anticoagulation is still not feasible in many RHD endemic regions because of the inevitable need for re-operation from expected usual degradation of bioprosthetic valves within one to two decades.
7. Other Recent Advances
7.1. Understanding of RHD-HIV Co-Infection
The regions of the world with the highest RF and RHD prevalence are also those with the greatest human immunodeficiency virus (HIV) prevalence, but there has been little investigation into the epidemiology of the dual burden of these diseases [58,199]. Previous small cross-sectional surveys in Uganda have reported conflicting results regarding the association between HIV and RHD [200,201,202]. A recent description of the epidemiologic profile and longitudinal outcomes of an HIV-RHD comorbid population, however, revealed that the prevalence of HIV in this cohort was not significantly higher than that of the general Ugandan population, with rates of 3.6%, compared to a national range of 2.1% in children and 6.2% in people over 15 years of age [203]. Furthermore, comorbid individuals did not appear to suffer higher mortality rates than those with RHD alone. However, HIV-RHD comorbid subjects had nearly threefold higher odds of having suffered a stroke or transient ischemic attack compared to those without HIV [203,204]. Overall, these data imply that aside from elevated cerebrovascular accident risk, RHD defines the short-term clinical outcomes of this group of people more than HIV does [205]. As major innovations in HIV treatment have significantly improved the long-term survival of people living with HIV, comorbid noncommunicable diseases have begun to dominate their morbidity and mortality [206]. This presents an opportunity for RHD care networks to leverage and adopt tools and innovations developed for the HIV public health effort, such as the Cascade of Care, to benefit not just HIV-RHD comorbid patients, but also individuals residing in LMICs affected by RHD in general [207,208].
4. RHD Policy Advances
4.1. Understanding of RHD-Associated Costs in Endemic Regions
7.2. Understanding of RHD-Associated Costs in Endemic Regions
RHD costing data from endemic countries and regions has historically been quite sparse. However, cost-effectiveness analyses comparing primary, secondary, and tertiary prevention of RHD in the African setting have recently been conducted
[145][209]. Such findings have revealed that scaling up primary prevention would be a cost-saving approach, with a negative incremental cost-effectiveness ratio (ICER) of -$2539 USD per DALY averted, whilst putting efforts into secondary prevention programs would be cost-effective (USD $752 per DALY averted)
[145][209]. The investments required for local surgical capacity development were high with limited impact (ICER of USD $23,827 per DALY averted for constructing a local surgical center)
[145][209]. Several other analyses have separately explored optimal cost-effective strategies for primary prevention
[146][210], secondary prevention
[147][148][149][150][211,212,213,214], and a combination of both
[150][151][152][214,215,216]. A recent modeling study for the prevention and management of RHD in the African Union concluded that, “In the short term, costs of secondary prevention and secondary and tertiary care for RHD are lower than for primary prevention, and benefits accrue earlier
[153][217]”. Most analyses make use of Markov models, and similar challenges relating to lack of precise transition probabilities on which to base the calculations have been reported
[145][148][151][209,212,215].
Additionally, recent studies regarding the cost of illness have described the substantial economic impact of RHD at the household, health system, and national level in endemic countries such as Uganda
[154][218], South Africa
[155][156][219,220], India
[157][158][221,222], and others
[159][223].
4.2. Global Efforts, Advocacy, and Stakeholder Engagement in the Fight against RHD
7.3. Global Efforts, Advocacy, and Stakeholder Engagement in the Fight against RHD
The growing research and healthcare/awareness projects in RHD worldwide, combined with a considerable increase in research interest over the past two decades, has raised multisectoral attention regarding this neglected disease. This has resulted in international coordination of efforts which have been multifaceted, with ambitious aims (Table 23).
Table 23. Summarized aims of global efforts in the fight against RHD, and key charges from the 2018 WHA resolution to member states. Abbreviations: RHD, rheumatic heart disease; WHO, World Health Organization; WHF, World Heart Federation; WHA, World Health Assembly.
As an example of practical outcomes of this international coordination, in 2011 the United Nations set key targets to reach by 2025, including a reduction in the risk of premature noncommunicable disease death–markedly cardiovascular disease–by 25% by 2025; with RHD notably included in this agenda
[163][45]. Consequently, multiple authoritative individuals
[164][165][42,43], societies, task forces, unions and federations, at regional, continental and international levels have published position statements
[163][166][167][168][169][44,45,46,226,227], serving as a basis for guiding research and healthcare initiatives, helping define “next steps” and priorities for the global scientific agenda. The WHF has played a particularly pivotal role in such initiatives, with its first broad position statement on RHD released in 2013 reinforcing key aims and actions in a similar direction of preceding African statements
[169][227]. More recently, there was a re-dedication of the American Heart Association (AHA) on the RHD agenda
[170][228] with resumption of its intensive work on the development of guidelines and statements
[121][137][7,178], research funding through its councils, and a working group dedicated to RF and RHD control.
These aforementioned position publications and statements from different organizations and regions, combined with the intensive collaborative multisectoral efforts worldwide, were recognized by the 2018 World Health Assembly Global Resolution to end RHD
[160][161][162][47,224,225]. The key charges that this resolution brought to member states are listed in
Table 23. In light of this unprecedented collaborative resolution, health systems should move towards enacting its actionable recommendations, increasing investment in primary care and general health infrastructure, sanitation and housing, medical supply and building capacity for RHD prevention and management
.
8. Conclusions
We now find ourselves in a period in history that could again be marked by rapid progress towards elimination of RHD, this time on the global, rather than high-income regional, stage. Application of modern scientific techniques for improving RHD prevention, diagnosis and treatment have the potential to revolutionize our approach to RHD control and are urgently needed. Progress is being made in basic science, clinical, translational, and population-based research. However, to sustain and accelerate this trajectory, substantial multisector investment, including research funding, capacity building, and resources for education and awareness are urgently needed. The solutions are within our grasp and with adequate investment, we may substantially reduce the global burden of RHD in our lifetime.