Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Jessie Wu and Version 1 by Stefano Brillanti.
Hepatitis Delta Virus (HDV) is the cause of hepatitis D, a relatively rare but aggressive form of viral hepatitis developing in patients co-infected with hepatitis B virus (HBV). HDV infection is associated with HBV infection since the defective HDV needs HBV to infect and replicate in the liver. Even if not a frequent cause of chronic liver disease, HDV infection is responsible for an aggressive progression of hepatitis towards advanced liver disease.
- HDV
- hepatitis Delta
- drugs
- bulevirtide
- interferon
- cirrhosis
- chronic hepatitis
1. Introduction
Probably vastly underestimated in HBsAg carriers, the lack of standardized virological methods to diagnose and monitor the infection and effective therapy to treat the liver disease have conditioned the progress in research and clinical management. However, after almost half a century from the initial discovery of the Delta agent, recent developments in understanding and targeting the therapeutic efforts have opened new hope for patients with hepatitis D. In thiRes narrative review, we earchers try to summarize and focus on the new opportunities in the management of Delta hepatitis.
2. When All of This Started
Hepatitis Delta virus (HDV) is a defective RNA viral agent associated with HBV infection. In 1977, in Turin, Italy, Mario Rizzetto first detected by immunofluorescence a new antigen, named Delta, in the liver cell nuclei of patients with HBsAg positive chronic liver disease. Corresponding circulating antibodies were similarly found in the serum of chronic HBsAg carriers, especially those with liver damage [1]. However, it took a few years to understand that the new antigen was not secreted by HBV but represented an independent agent transmitted by superinfection or coinfection of HBsAg carriers. The new agent was characterized as a defective RNA pathogen dependent for replication and infection on helper functions provided by HBV. The virion is a 35–37 nm particle, with the Delta antigen and the RNA genome within a coat made by the HBsAg lipoprotein [2]. The prevalence of HDV infection is limited to individuals with HBV infection, as coinfection with HBV of normal subjects or superinfection of HBsAg carriers. Parenteral transmission is the route of propagating infection from one individual to another [3]. Since the 1980s, it was clear that HDV infection had high pathogenic potential, inducing hepatitis in all infected subjects. Hepatitis may be acute or chronic, the former more frequently associated with coinfection, and the latter mainly occurring after superinfection. The HBsAg carrier state represents the ideal background for infection and replication of HDV, and the subsequent chronic hepatitis is generally active and severe, progressing to more advanced liver disease within a few years [4]. All of this has been known for decades, and wresearchers are still waiting for significant progress in the clinical management of Delta hepatitis.3. New Drugs for Delta Hepatitis
Different approaches have been investigated to interfere and suppress HDV replication during the last years. As a result, three significant therapeutic mechanisms have been identified: (1) inhibition of HDV prenylation, (2) inhibition of HBsAg release and (3) inhibition of cell entry [12][5] (Figure 1).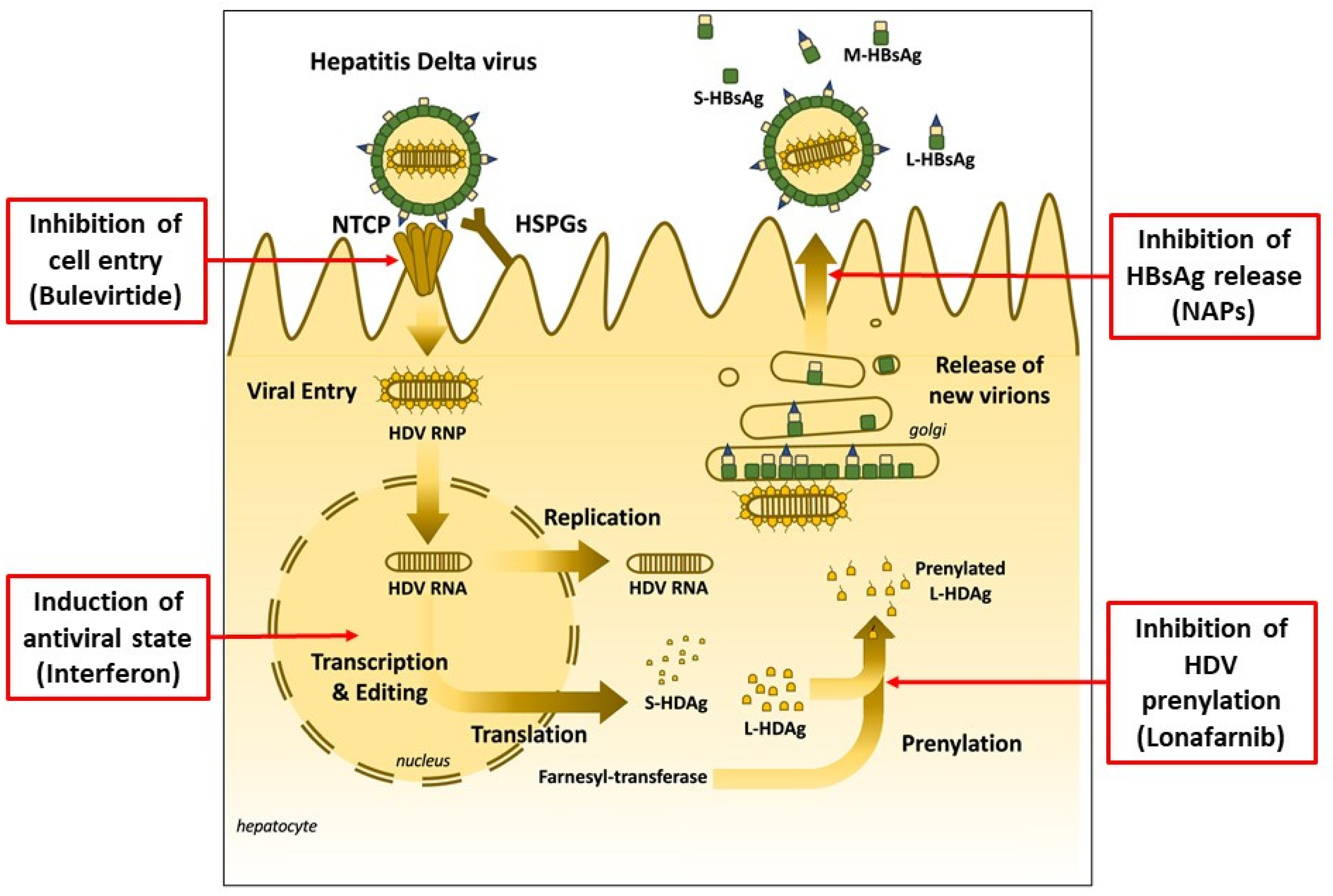
Figure 1. Hepatitis Delta Virus infection and therapeutic targets of currently available and experimental new drugs (adapted from Liver Int. 2021, 41 (Suppl. 1), 30–37, used with permission).
References
- Rizzetto, M.; Canese, M.G.; Arico, S.; Crivelli, O.; Trepo, C.; Bonino, F.; Verme, G. Immunofluorescence detection of new antigen-antibody system (δ/anti-δ) associated to hepatitis B virus in liver and in serum of HBsAg carriers. Gut 1977, 18, 997–1003.
- Rizzetto, M.; Verme, G. Delta hepatitis—Present status. J. Hepatol. 1985, 1, 187–193.
- Urban, S.; Neumann-Haefelin, C.; Lampertico, P. Hepatitis D virus in 2021: Virology, immunology and new treatment approaches for a difficult-to-treat disease. Gut 2021, 70, 1782–1794.
- Romeo, R.; Del Ninno, E.; Rumi, M.; Russo, A.G.; Sangiovanni, A.; de Franchis, R.; Ronchi, G.; Colombo, M. A 28-Year Study of the Course of Hepatitis Δ Infection: A Risk Factor for Cirrhosis and Hepatocellular Carcinoma. Gastroenterology 2009, 136, 1629–1638. Available online: https://doi.org/10.1053/J.GASTRO.2009.01.052/ATTACHMENT/2037C2FD-79EA-457B-86B0-10DDE1C33CC5/MMC1.MP4 (accessed on 5 February 2022).
- Loureiro, D.; Castelnau, C.; Tout, I.; Boyer, N.; Narguet, S.; Menasria Benazzouz, S.; Louis, Z.; Pons-Kerjean, N.; Giuly, N.; Marcellin, P.; et al. New therapies for hepatitis delta virus infection. Liver Int. 2021, 41 (Suppl. 1), 30–37.
- Koh, C.; Canini, L.; Dahari, H.; Zhao, X.; Uprichard, S.L.; Haynes-Williams, V.; Winters, M.A.; Subramanya, G.; Cooper, S.L.; Pinto, P.; et al. Oral prenylation inhibition with lonafarnib in chronic hepatitis D infection: A proof-of-concept randomized, double-blind, placebo-controlled phase 2A trial. Lancet Infect. Dis. 2015, 15, 1167–1174.
- Yurdaydin, C.; Keskin, O.; Kalkan, C.; Karakaya, F.; Çalişkan, A.; Karatayli, E.; Karatayli, S.; Bozdayi, A.M.; Koh, C.; Heller, T.; et al. Optimizing lonafarnib treatment for the management of chronic delta hepatitis: The LOWR HDV-1 study. Hepatology 2018, 67, 1224–1236.
- Bazinet, M.; Pântea, V.; Cebotarescu, V.; Cojuhari, L.; Jimbei, P.; Albrecht, J.; Schmid, P.; Le Gal, F.; Gordien, E.; Krawczyk, A.; et al. Safety and efficacy of REP 2139 and pegylated interferon alfa-2a for treatment-naive patients with chronic hepatitis B virus and hepatitis D virus coinfection (REP 301 and REP 301-LTF): A non-randomized, open-label, phase 2 trial. Lancet Gastroenterol. Hepatol. 2017, 2, 877–889.
- Bogomolov, P.; Alexandrov, A.; Voronkova, N.; Macievich, M.; Kokina, K.; Petrachenkova, M.; Lehr, T.; Lempp, F.A.; Wedemeyer, H.; Haag, M.; et al. Treatment of chronic hepatitis D with the entry inhibitor myrcludex B: First results of a phase Ib/IIa study. J. Hepatol. 2016, 65, 490–498.
- Asselah, T.; Arama, S.S.; Bogomolov, P.; Bourliere, M.; Fontaine, H.; Gherlan, S.G.; Gorodin, V.; Hilleret, M.-N.; Lazar, S.; Mamonova, N.; et al. Safety and efficacy of bulevirtide monotherapy and in combination with Peginterferon alfa-2a in patients with chronic hepatitis delta: 24 weeks interim data of MYR204 Phase 2b study. J. Hepatol. 2021, 75, S205–S293. Available online: https://www.journal-of-hepatology.eu/article/S0168-8278(21)01842-0/pdf; https://linkinghub.elsevier.com/retrieve/pii/S0168827821018420 (accessed on 5 February 2022).
- Wedemeyer, H.; Aleman, S.; Andreone, P.; Blank, A.; Brunetto, M.; Bogomolov, P.; Chulanov, V.; Hilgard, G.; Merle, U.; Zotov, S.; et al. Bulevirtide monotherapy at low and high dose in patients with chronic hepatitis delta: 24 weeks interim data of the phase 3 MYR301 study. J. Hepatol. 2021, 75, S294–S803. Available online: https://www.journal-of-hepatology.eu/article/S0168-8278(21)01843-2/pdf (accessed on 5 February 2022).
- De Ledinghen, V.; Guyader, D.; Metivier, S.; Hilleret, M.-N.; Fontaine, H.; Roche, B.; Ganne-Carrie, N.; d’Alteroche, L.; Loustaud-Ratti, V.; Gervais, A.; et al. Safety and efficacy of 2mg bulevirtide in patients with chronic HBV/HDV coinfection. First real-world results (French Early Access Program). Hepatology 2021, 74 (Suppl. 1), 16A–17A.
- Loglio, A.; Ferenci, P.; Renteria, S.C.U.; Tham, C.Y.; Scholtes, C.; Holzmann, H.; van Bömmel, F.; Borghi, M.; Perbellini, R.; Rimondi, A.; et al. Safety and effectiveness of up to 3 years’ bulevirtide monotherapy in patients with HDV-related cirrhosis. J. Hepatol. 2022, 76, 464–469.
- Wang, W.; Lempp, F.A.; Schlund, F.; Walter, L.; Decker, C.C.; Zhang, Z.; Ni, Y.; Urban, S. Assembly and infection efficacy of hepatitis B virus surface protein exchanges in 8 hepatitis D virus genotype isolates. J. Hepatol. 2021, 75, 311–323.
More