Scholars have recently used “motor imagery” (MI) to refer to the imagination of moving particular body parts. Among the frameworks trying to explain the essence of motor imagery, there are two primary ones—motor simulation and motor emulation theory.
1. Introduction
The Motor Simulation Theory (MST) [1][2] provides a constructive explanation of the relation of imagery tasks such as motor imagery (MI task), observation, and the intention of motor tasks to motor execution (ME) tasks itself. According to MST, motor images have the same properties as analogous motor representations and thus have the same functional relationship to the perceived or represented movement and the same causal role in its development [1]. Alternatively, according to emulation theory, to simulate mechanical movement, proprioception, and kinesthesis, the “forward model” is represented by motor commands that drive body/environment emulators, which are motor and sensory representations. In such a way, coupled motor and sensory systems form a complex process of emulation that provides an adaptive motor control mechanism for ME. While performing MI, the motor system is coupled with afferent sensory systems, which provide the sensor feedback without input for MI [3].
The Motor Simulation Theory (MST) [4,5] provides a constructive explanation of the relation of imagery tasks such as motor imagery (MI task), observation, and the intention of motor tasks to motor execution (ME) tasks itself. According to MST, motor images have the same properties as analogous motor representations and thus have the same functional relationship to the perceived or represented movement and the same causal role in its development [4]. Alternatively, according to emulation theory, to simulate mechanical movement, proprioception, and kinesthesis, the “forward model” is represented by motor commands that drive body/environment emulators, which are motor and sensory representations. In such a way, coupled motor and sensory systems form a complex process of emulation that provides an adaptive motor control mechanism for ME. While performing MI, the motor system is coupled with afferent sensory systems, which provide the sensor feedback without input for MI [6].
2. Generalization of Brain Regions Involved in MI and ME
Studying and systematizing collected data to compare MI and ME emerged results represented in
Table 1
and
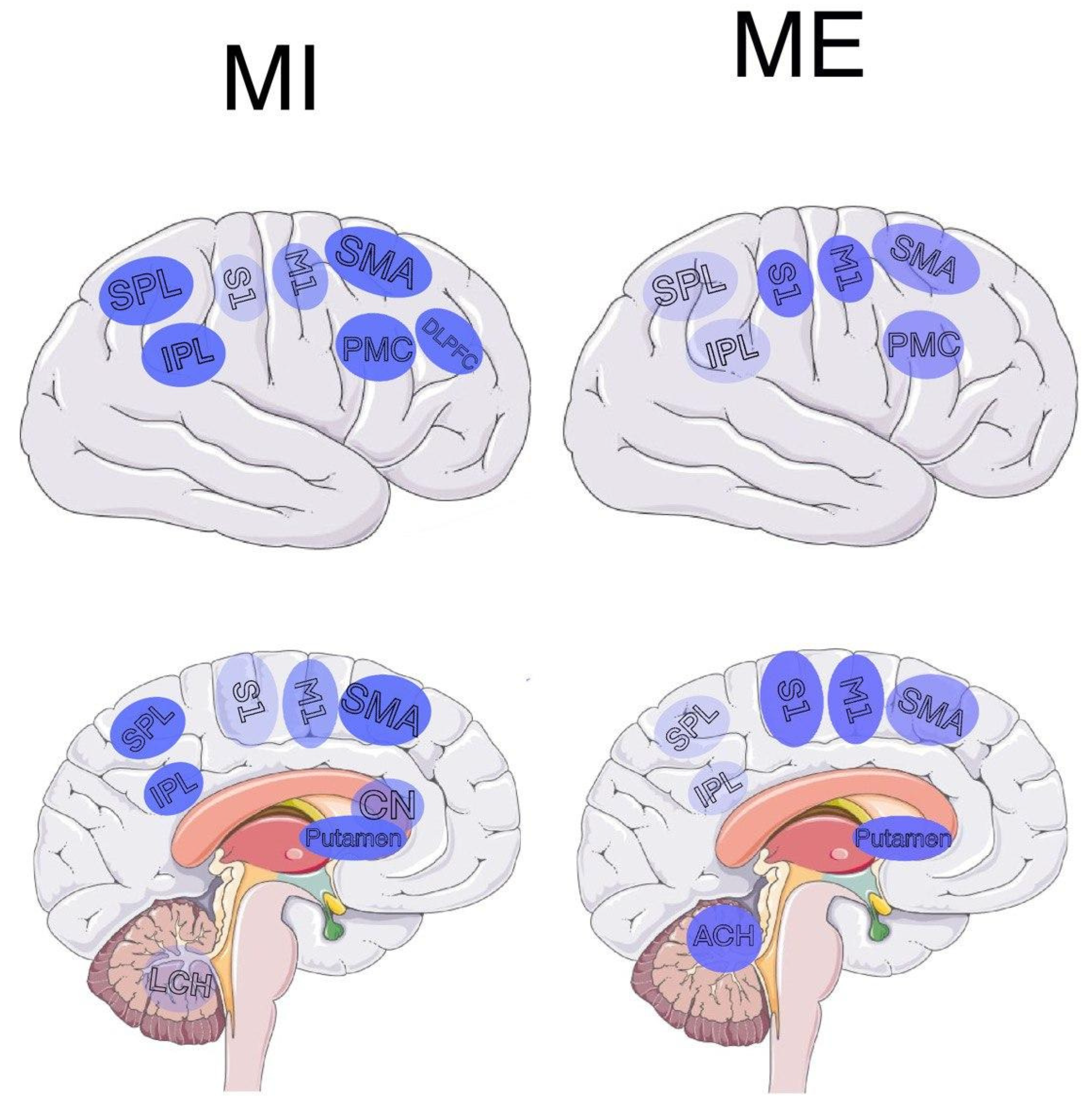
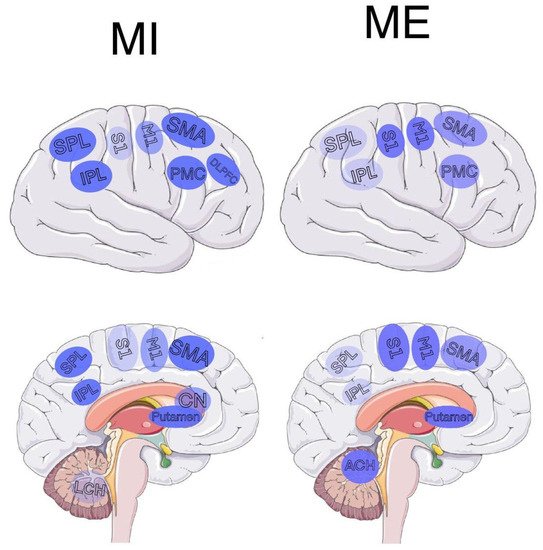
Figure 1. There is a significant overlap of the brain regions responsible for MI and ME. This similarity in brain activation for MI and ME could be explained by belonging to the same motor representation system [4]. Nevertheless, even though most research in this field is focused on activation sites overlap, a more comprehensive observation indicated significant differences between motor imagery and physical execution. . There is a significant overlap of the brain regions responsible for MI and ME. This similarity in brain activation for MI and ME could be explained by belonging to the same motor representation system [23]. Nevertheless, even though most research in this field is focused on activation sites overlap, a more comprehensive observation indicated significant differences between motor imagery and physical execution.
Figure 1.
Activation maps of brain regions during MI and ME. (Left) Brain activation map for MI; (right) brain activation map of ME. Abbreviations: PMC—premotor cortex, M1—primary motor cortex, S1, S2—primary and secondary somatosensory cortices, SMA—supplementary motor area, CN—caudate nucleus, LCH—lateral cerebellar hemisphere, ACH—anterior cerebellar hemisphere, SPL—superior parietal lobe, IPL—inferior parietal lobe, DLPFC—left dorsolateral prefrontal cortex. The intensity of color depicts the strength of activity in the corresponding region.
Table 1. Brain areas activated during MI and ME, aggregated papers.
| Brain Area |
Common for MI and ME |
MI |
ME |
| Inferior parietal lobe |
[5][6][24,25] |
[5][6][7][24,25,26] |
[5][6][24,25] |
| Superior parietal lobe |
[6][8][9][25,27,28] |
[6][7][8][9][25,26,27,28] |
[6][8][9][25,27,28] |
| Posterior parietal lobe |
[10][29] |
[10][11][12][29,30,31] |
[10][29] |
| Frontal parietal lobe |
[4][13][11,23] |
[4][10][13][11,23,29] |
[4][13][11,23] |
| Prefrontal cortex |
[14][10] |
[14][10] |
[13][14][10,11] |
| Subcortical |
[13][11] |
[6][13][11,25] |
[13][11] |
| Rostral premotor |
- |
[12][13][11,31] |
- |
| Striatum |
[5][13][11,24] |
[5][7][13][15][16][11,24,26,32,33] |
[5][13][11,24] |
| Cerebellar areas |
[4][6][10][13][14][17][10,11,23,25,29,34] |
[4][6][10][13][11,23,25,29] |
[4][5][6][7][[108,11,23],24[9,25][10,26][13,27][14,28][16,29][17,33],34] |
| M1 |
[6][9][17][25[,2818,34],35] |
[6][9][17][18][19][20][25,28,34,35,36,37] |
[4][5][6][9][10],28[14],29[16],33[17],34[18],35[20][10,23,24,25,37] |
| S1 |
[9][17][28,34] |
[9][17][28,34] |
[9][10]28[14],29[17],34[20][10,,37] |
| S2 |
[21][38] |
[21][38] |
[21][38] |
| SMA |
[8][9][14][17][10,27,28,34] |
[6][8][9][10][14][17][10,25,27,28,29,34] |
[4][5][8][9][14][17][10,23,24,27,28,34] |
| PMC |
[9][17][28,34] |
[9][17][28,34] |
[7][9][17][26,28,34] |
| Central sulcus |
- |
[13][11] |
- |
| Precentral gyri |
- |
- |
[18][35] |
| Frontal gyri |
- |
[10][29] |
- |
| Left DLPFC |
- |
[22][39] |
- |
3. Motor Imagery Assessment
Imagination is a complex phenomenon in which vividness, intensity, and representation are not the same in every person [23][24]. Studies show that some people cannot even use various types of imagination, including motor imagination [24]. The difference from person to person in terms of forms of imagination makes the research process in this field complex. Therefore, assessing imagery ability prior to conducting an imagery experiment or participating in an imagery training program is essential. Imagination is a complex phenomenon in which vividness, intensity, and representation are not the same in every person [40,41]. Studies show that some people cannot even use various types of imagination, including motor imagination [41]. The difference from person to person in terms of forms of imagination makes the research process in this field complex. Therefore, assessing imagery ability prior to conducting an imagery experiment or participating in an imagery training program is essential.
For creating a successful method for assessing MI, it is crucial to understand its properties and aspects that could be expressed numerically and evaluated for a subject. According to Jeannerod [25], motor representations are involved in both conscious and unconscious cognitive activities. Examples involving conscious motor representation are imagining a limb movement in the first person and dreams, so-called explicit motor imagery. In contrast, examples that involve unconscious motor representations are prospective action judgments and motorically driven perceptual decisions (e.g., defining hand laterality in different depicted positions), so-called implicit motor imagery. Jeannerod also distinguished motor imagery from dynamic visual imagery and movement imagery from an external viewpoint, referring them to a visual type of imagery. The essential part of motor imagery that distinguishes this type of imagery from a visual one is a kinaesthetic sensation that allows the subject to experience the feeling of performing movements. Nevertheless, the phenomenon of motor imagery could not be reduced to the kinesthetic sense only as it develops in a body-centered and visuospatial context. So, motor imagery includes kinesthetic, visual, and spatial aspects of movement executed by an imager [26]. Therefore, all of the above aspects as characteristics of the experiencing of imaginative movement must be considered when assessing motor imagination. For creating a successful method for assessing MI, it is crucial to understand its properties and aspects that could be expressed numerically and evaluated for a subject. According to Jeannerod [42], motor representations are involved in both conscious and unconscious cognitive activities. Examples involving conscious motor representation are imagining a limb movement in the first person and dreams, so-called explicit motor imagery. In contrast, examples that involve unconscious motor representations are prospective action judgments and motorically driven perceptual decisions (e.g., defining hand laterality in different depicted positions), so-called implicit motor imagery. Jeannerod also distinguished motor imagery from dynamic visual imagery and movement imagery from an external viewpoint, referring them to a visual type of imagery. The essential part of motor imagery that distinguishes this type of imagery from a visual one is a kinaesthetic sensation that allows the subject to experience the feeling of performing movements. Nevertheless, the phenomenon of motor imagery could not be reduced to the kinesthetic sense only as it develops in a body-centered and visuospatial context. So, motor imagery includes kinesthetic, visual, and spatial aspects of movement executed by an imager [43]. Therefore, all of the above aspects as characteristics of the experiencing of imaginative movement must be considered when assessing motor imagination.
4. Transcranial Magnetic Stimulation in MI Research
Transcranial magnetic stimulation (TMS) is widely accepted as a powerful noninvasive tool for analyzing the central and peripheral nervous systems of people. Magnetic stimulation has a similar activation mechanism to electrical stimulation for activating peripheral nerves. TMS excites the pyramidal neurons transsynaptically resulting in the rise of I (indirect) waves. In contrast, transcranial electrical stimulation excites the pyramidal tract axons directly, either at the beginning segment of the neuron or at proximal internodes in the subcortical white matter, resulting in D (direct) waves [27]. Transcranial magnetic stimulation (TMS) is widely accepted as a powerful noninvasive tool for analyzing the central and peripheral nervous systems of people. Magnetic stimulation has a similar activation mechanism to electrical stimulation for activating peripheral nerves. TMS excites the pyramidal neurons transsynaptically resulting in the rise of I (indirect) waves. In contrast, transcranial electrical stimulation excites the pyramidal tract axons directly, either at the beginning segment of the neuron or at proximal internodes in the subcortical white matter, resulting in D (direct) waves [61].
The significant and well-studied feature of TMS is its application in motor and motor imagery studies. Figure 2 demonstrates the most commonly used TMS protocols in MI research. TMS applied to the motor cortex induces an excitatory effect on corticospinal neurons, which can be assessed with electromyography as motor evoked potentials (MEPs) and/or [27]. Moreover, cortical stimulation with TMS can induce not only excitatory effects but inhibitory too. This characteristic may be utilized to analyze functions of the brain regions other than the motor cortex. It results in the capability of TMS to map brain regions and investigate functional connectivity among distinct cortical regions [27]. Another crucial feature of TMS is its long-term effect on brain function. Even after stopping the stimulation, the corresponding stimulating effect lasts for a long time (starting from several hours to several months in the case of medical applications [28][29][30]). All these features make TMS a powerful tool for motor imagery studies. demonstrates the most commonly used TMS protocols in MI research. TMS applied to the motor cortex induces an excitatory effect on corticospinal neurons, which can be assessed with electromyography as motor evoked potentials (MEPs) and/or [61]. Moreover, cortical stimulation with TMS can induce not only excitatory effects but inhibitory too. This characteristic may be utilized to analyze functions of the brain regions other than the motor cortex. It results in the capability of TMS to map brain regions and investigate functional connectivity among distinct cortical regions [61]. Another crucial feature of TMS is its long-term effect on brain function. Even after stopping the stimulation, the corresponding stimulating effect lasts for a long time (starting from several hours to several months in the case of medical applications [62,63,64]). All these features make TMS a powerful tool for motor imagery studies.
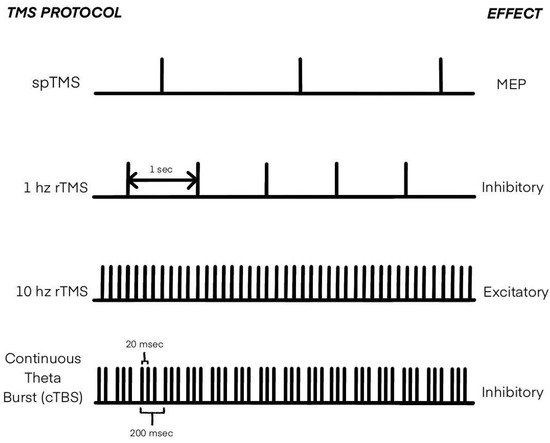
Figure 2. Types of transcranial magnetic stimulation (TMS) applied in MI research.
5. Applications, MI for Diagnostics
The applications of MI for BCI operation, in rehabilitation systems in sports, have become conventional. There is a bulk of papers and reviews on these issues [31][32][33][34][35][36]. Another exciting and promising trend in MI applications is researching and diagnosing various neurodegenerative diseases and psychoses, especially schizophrenia [37][38][39][40][41]. For example, based on the analysis of the difficulties in MI, the researchers of the review [42] conclude that schizophrenia involves, as well, impairments of the posterior parietal cortex. Moreover, they present a novel hypothesis that suggests differential impairments of the left and right parietal cortices in schizophrenia, which may help explain many of the first-rank symptoms of the disorder. The study [43] revealed that patients with schizophrenia performed motor imagery of gait slower than healthy controls. This deficit could be in part explained by impaired executive function and specifically by a disturbance in the sensitivity to interference. The paper [44] showed that schizophrenia patients, similarly to nonclinical participants, overestimated tool-related benefits and underestimated tool-related effort in terms of time when they mentally simulated a task requiring the use of a tool. These results open new perspectives on the issue of effort in schizophrenia. The applications of MI for BCI operation, in rehabilitation systems in sports, have become conventional. There is a bulk of papers and reviews on these issues [12,13,14,15,21,22]. Another exciting and promising trend in MI applications is researching and diagnosing various neurodegenerative diseases and psychoses, especially schizophrenia [16,17,18,19,104]. For example, based on the analysis of the difficulties in MI, the authors of the review [20] conclude that schizophrenia involves, as well, impairments of the posterior parietal cortex. Moreover, they present a novel hypothesis that suggests differential impairments of the left and right parietal cortices in schizophrenia, which may help explain many of the first-rank symptoms of the disorder. The study [105] revealed that patients with schizophrenia performed motor imagery of gait slower than healthy controls. This deficit could be in part explained by impaired executive function and specifically by a disturbance in the sensitivity to interference. The paper [106] showed that schizophrenia patients, similarly to nonclinical participants, overestimated tool-related benefits and underestimated tool-related effort in terms of time when they mentally simulated a task requiring the use of a tool. These results open new perspectives on the issue of effort in schizophrenia.
The work [45] investigated motor retardation in bipolar depression. FMRI showed that, during motor imagery, the patients activated the posterior medial parietal cortex, the posterior cingulate cortex, the premotor cortex, the prefrontal cortex, and the frontal poles more than the healthy controls did. In addition, limbic and prefrontal regions associated with self-reference and the default mode network were altered during motor imagery in bipolar depression with motor retardation. The study [46] investigated the influence of unipolar depression on MI ability using a pointing task. Compared to controls, depressed patients showed marked motor slowing on actual and imagined movements. More significant temporal discrepancies between actual and mental movements were observed in depressed patients than in healthy controls. Furthermore, depressed patients modulated, to some extent, mental movement durations according to the difficulty of the task, but this modulation was not as strong as that of healthy subjects. These results suggest that unipolar depression significantly affects the higher stages of action planning and points out a selective decline of motor prediction. The work [107] investigated motor retardation in bipolar depression. FMRI showed that, during motor imagery, the patients activated the posterior medial parietal cortex, the posterior cingulate cortex, the premotor cortex, the prefrontal cortex, and the frontal poles more than the healthy controls did. In addition, limbic and prefrontal regions associated with self-reference and the default mode network were altered during motor imagery in bipolar depression with motor retardation. The study [108] investigated the influence of unipolar depression on MI ability using a pointing task. Compared to controls, depressed patients showed marked motor slowing on actual and imagined movements. More significant temporal discrepancies between actual and mental movements were observed in depressed patients than in healthy controls. Furthermore, depressed patients modulated, to some extent, mental movement durations according to the difficulty of the task, but this modulation was not as strong as that of healthy subjects. These results suggest that unipolar depression significantly affects the higher stages of action planning and points out a selective decline of motor prediction.
Reference [47] addressed action simulation processes in adolescents with Asperger syndrome (AS) using the following MI tasks: the classical hand laterality task and the mental rotation of letters. The authors demonstrated a specific alteration of motor imagery skills in AS—they found the biomechanical effect (the advantage for judging hand pictures showing physically comfortable versus physically awkward positions) in typically-developing participants but not in participants with AS. Reference [109] addressed action simulation processes in adolescents with Asperger syndrome (AS) using the following MI tasks: the classical hand laterality task and the mental rotation of letters. The authors demonstrated a specific alteration of motor imagery skills in AS—they found the biomechanical effect (the advantage for judging hand pictures showing physically comfortable versus physically awkward positions) in typically-developing participants but not in participants with AS.
Thus, motor imagery is a powerful and promising tool for research and diagnostics of various neurodegenerative disorders and psychoses, whose potential has not yet been fully realized.