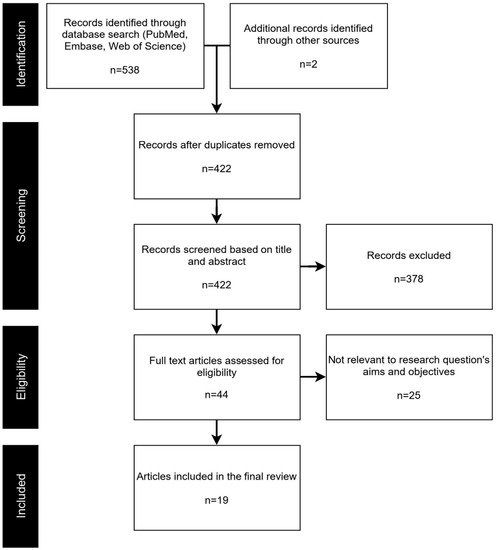
PRISMA study selection flowchart.
Table S1 outlines the main characteristics of the systems detailed in each study. For studies in which the surveillance strategy was multifaceted and had many branches of surveillance activities (and in different subsystems), only the core components of the system were detailed. For example, for Super Bowl XLIX in 2016, multiple systems were outlined as part of the overall surveillance strategy, including hospital and urgent care surveillance, emergency room syndromic surveillance, and real-time onsite syndromic surveillance [20].
The scope and number of syndromic indicators or syndrome classifications ranged widely among the studies. Some studies limited the syndromes included in surveillance to a specific geographic region. For example, researchers conducted a system and disease risk assessment including a literature review of the disease patterns, assessment of disease databases, assessment of the public health and surveillance teams, and interviews and focus groups with key stakeholders within the Solomon Islands, where the mass gathering event was going to happen
[10][37]. In another case, a system included a case definition for acute diarrhea as a response to a local outbreak of rotavirus that was occurring in South Tarawa at the time of the 2013 Kiribati Independence Celebrations
[11][32]. Some of the systems (n = 5) used event-related tags to establish a clear connection between a patient visit and the mass gathering event. For the 2015 Special Olympics, proactive patient tagging was used to flag attendees of the event in ED clinical notes, which allowed subsequent algorithms to easily identify those patients and potential health concerns related to the event
[12][21]. For surveillance activities surrounding the 2017 solar eclipse viewing events in Kentucky, US, “eclipse” was included as a unique syndromic classification
[13][26]. “Inauguration-related” was included as a syndrome definition for surveillance activities oriented around the 2017 US presidential inauguration
[14][25].
In this
scoping re
searchview, syndromic surveillance was examined as a potential strategy for providing support to and maintaining the robustness of public health infrastructure surrounding mass gathering scenarios. Nineteen studies were identified for data extraction and key information was collected about the mass gathering events and related syndromic surveillance activities. The systems described were implemented in a wide range of geographic and socio-economic settings, indicating a diverse potential for syndromic surveillance to meet the needs of different environments.
As identified in the present
re
ntryview, a core component of a reliable syndromic surveillance system or infrastructure, with regard to implementation during a mass gathering scenario, is ample preparation. In all studies examined, syndromic surveillance activities were preceded to some degree by a preparation phase. Since event-oriented surveillance is dependent on the integration of data from multiple sources as well as different mediums (e.g., hospitals and first aid stations), it is necessary that sufficient time be given to organize and facilitate collaborations among several entities. For the 2015 Super Bowl, communication was described among a large number of health agencies, healthcare providers, and businesses, including the Maricopa Department of Health, Maricopa County hospitals, local hotels, Arizona Department of Health Services and the U.S. Centers for Disease Control and Prevention, as well as other agencies and services. A vital component of the preparation phase prior to syndromic surveillance is training key staff members and physicians. This was especially important in scenarios where surveillance activities stemmed from event-based care sites, such as first aid stations and mobile clinics. There is a clear benefit to assessing disease profiles of regions proximal to the mass gathering event. In one circumstance, a literature review was conducted to identify disease trends within the area of operation as well as an assessment of pre-existing public health and lab surveillance infrastructure. This
researchstudy also describes a risk assessment examining the characteristics of the mass gathering scenario
[10][37].
Previous research has examined the potential for syndromic surveillance to detect disease outbreaks earlier than other forms of public health surveillance
[15][16][7,38]. In the present re
svie
archw, the evidence to support these claims is limited with regard to a mass gathering scenario. While most of the studies indicated that the purported systems functioned reliably under the strain of increased clinical visits, none of the studies indicated that any significant outbreaks of disease were detected. In one case, a system was modified to meet the needs of an outbreak spurred by a mass gathering event
[11][32]. Additionally, very few studies outlined any attempts at contemporaneously investigating or validating the data collected and analyzed by the system. In some cases, syndromes with low prevalence were suspected to not generate a sufficiently strong signal in the detection measures implemented by a system. However, without cross-validation with other data sources independent of the described system, it is difficult to establish whether the signals generated should warrant a potentially costly public health response.
3. Conclusions
Further research is necessary to conclude whether syndromic surveillance has a verifiable impact on the health of the populations under surveillance during mass gathering scenarios. The goal of the present re
svie
archw was to outline the process of preparing for and implementing this surveillance strategy at mass gathering events; however, further analysis of health and disease profiles at these events is necessary.