Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 1 by Chiara Lembo and Version 3 by Camila Xu.
Erythropoietin (Epo) is a 30.4 kDa glycoprotein and pleiotropic cytokine, first described by Carnot in 1906 and isolated by Goldwasser and Kung in 1971, successfully produced for clinical use.
- neuroprotection
- preterm
- Hypoxic Ischemic Encephalopathy
- Erythropoietin
- perinatal stroke
1. Erythropoietin (Epo) Actions and Neuroprotective Effects
Erythropoietin is a 30.4 kDa glycoprotein and pleiotropic cytokine, first described by Carnot in 1906 and isolated by Goldwasser and Kung in 1971, successfully produced for clinical use [1]. During fetal life Epo is produced by the liver, while after birth the production progressively takes place in the peritubular cells of the kidney [2]. Erythropoietin is primarily known for the haematological functions. After an ischemic insult lasting at least 30 min, the transcription of the Hypoxia Inducible Transcription Factor induced by hypoxia determines an increase of Epo hormone production in the kidney [3][4]. Binding of Epo to receptors on erythroid progenitor cells causes an increase in red blood cell mass. The enhanced oxygen-carrying capacity of the blood suppress the further expression of Epo completing the feedback loop [5].
Erythropoietin is a 30.4 kDa glycoprotein and pleiotropic cytokine, first described by Carnot in 1906 and isolated by Goldwasser and Kung in 1971, successfully produced for clinical use [55]. During fetal life Epo is produced by the liver, while after birth the production progressively takes place in the peritubular cells of the kidney [56]. Erythropoietin is primarily known for the haematological functions. After an ischemic insult lasting at least 30 min, the transcription of the Hypoxia Inducible Transcription Factor induced by hypoxia determines an increase of Epo hormone production in the kidney [57,58]. Binding of Epo to receptors on erythroid progenitor cells causes an increase in red blood cell mass. The enhanced oxygen-carrying capacity of the blood suppress the further expression of Epo completing the feedback loop [59].
The endogenous levels of Epo have been reported to increase in the brain for four hours after hypoxic exposure [6]. Hypoxia induce hypoxia-inducible factor-1, which determines the expression of growth factors such as the vascular endothelial growth factor (VEGF) and Epo [7]. The immediate effect of Epo is represented by an augmented expression of haemoglobin which improves the oxygen consumption and storage in the hypoxic tissue [5]. Therefore, high serum or amniotic fluid concentrations of Epo may suggest chronic hypoxia in newborns [8]. However, the lack of brain perfusion and oxygenation which occurs in brief periods, but still severe enough to cause brain injury, may not trigger endogenous Epo production [9]. Erythropoietin exerts intracellular protective effects after the ischemia-reperfusion damage, such as decreasing apoptosis, oxidative stress and Blood Brain Barrier (BBB) injury [10]. Furthermore, Epo has been proved to be able to stimulate angiogenesis, neurogenesis and neuronal plasticity after the ischemic damage [11][12].
The endogenous levels of Epo have been reported to increase in the brain for four hours after hypoxic exposure [60]. Hypoxia induce hypoxia-inducible factor-1, which determines the expression of growth factors such as the vascular endothelial growth factor (VEGF) and Epo [61]. The immediate effect of Epo is represented by an augmented expression of haemoglobin which improves the oxygen consumption and storage in the hypoxic tissue [59]. Therefore, high serum or amniotic fluid concentrations of Epo may suggest chronic hypoxia in newborns [62]. However, the lack of brain perfusion and oxygenation which occurs in brief periods, but still severe enough to cause brain injury, may not trigger endogenous Epo production [63]. Erythropoietin exerts intracellular protective effects after the ischemia-reperfusion damage, such as decreasing apoptosis, oxidative stress and Blood Brain Barrier (BBB) injury [64]. Furthermore, Epo has been proved to be able to stimulate angiogenesis, neurogenesis and neuronal plasticity after the ischemic damage [65,66].
Pleiotropic functions of Epo concerning neuroprotection have been studied in the last few decades. The first evidence for the extra-hematopoietic properties of Epo were published between 1993 and 2000 [13][14]. Normally, only a small percentage of circulating Epo is able to pass the BBB, binding the Epo receptor (EpoR) located on the capillary vessels [15]. However, it has been demonstrated that Epo is also produced in the developing brain, where it acts as a neuroprotective agent and growing factor [16][17][18]. In particular, Epo is primarily produced by astrocytes, followed by oligodendrocytes, endothelial cells, neurons and microglia, induced by hypoxia through the Hypoxia Inducible Transcription Factor pathway [16][17][18].
Pleiotropic functions of Epo concerning neuroprotection have been studied in the last few decades. The first evidence for the extra-hematopoietic properties of Epo were published between 1993 and 2000 [67,68]. Normally, only a small percentage of circulating Epo is able to pass the BBB, binding the Epo receptor (EpoR) located on the capillary vessels [69]. However, it has been demonstrated that Epo is also produced in the developing brain, where it acts as a neuroprotective agent and growing factor [70,71,72]. In particular, Epo is primarily produced by astrocytes, followed by oligodendrocytes, endothelial cells, neurons and microglia, induced by hypoxia through the Hypoxia Inducible Transcription Factor pathway [70,71,72].
Figure 1. Both in animal models and in newborns, Epo has shown anti-apoptotic [19][20][21], antioxidant [22][23][24] and anti-inflammatory properties [25][26][27][28][29]. These actions can be exerted directly or mediated by a specific receptor named EpoR, which has been isolated in glial cells, neurons and brain endothelial cells in the hippocampus, cortex internal capsule and midbrain regions [16]. Molecular mechanisms following Epo treatment are shown in
. Both in animal models and in newborns, Epo has shown anti-apoptotic [73,74,75], antioxidant [76,77,78] and anti-inflammatory properties [79,80,81,82,83]. These actions can be exerted directly or mediated by a specific receptor named EpoR, which has been isolated in glial cells, neurons and brain endothelial cells in the hippocampus, cortex internal capsule and midbrain regions [70]. Molecular mechanisms following Epo treatment are shown in
Figure 2. When not binding to its ligand, EpoR activates pathways leading to cell death. On the contrary, when Epo is bound to EpoR, cellular survival is promoted [30][31]. In addition, the role of Epo has also been described in promoting angiogenesis [20][32][33], oligodendrogenesis and neurogenesis [34][35][36][37]. In most of clinical studies, Epo is given in the form of recombinant human erythropoietin (rhEpo), which was the first purified and cloned [38]. Considering the difficulties in obtaining a sufficient quantity of Epo from the blood serum of living humans, rhEpo is produced in higher quantities from cultured mammalian hamster ovary cells and is highly purified [38][39]. At least nine isoforms of rhEpo can be identified, among which are epoetin alfa/alpha/beta, darbepoetin (Darbe) and carbamylated Epo [40]. Darbe is an analog of Epo with an additional sialic acid, able to confer a three-fold longer serum half-life compared with epoetin alfa, the most used isoform [41]. Epo and Darbe are termed as erythropoiesis-stimulating agents (ESAs) [42].
. When not binding to its ligand, EpoR activates pathways leading to cell death. On the contrary, when Epo is bound to EpoR, cellular survival is promoted [84,85]. In addition, the role of Epo has also been described in promoting angiogenesis [74,86,87], oligodendrogenesis and neurogenesis [88,89,90,91]. In most of clinical studies, Epo is given in the form of recombinant human erythropoietin (rhEpo), which was the first purified and cloned [92]. Considering the difficulties in obtaining a sufficient quantity of Epo from the blood serum of living humans, rhEpo is produced in higher quantities from cultured mammalian hamster ovary cells and is highly purified [92,93]. At least nine isoforms of rhEpo can be identified, among which are epoetin alfa/alpha/beta, darbepoetin (Darbe) and carbamylated Epo [94]. Darbe is an analog of Epo with an additional sialic acid, able to confer a three-fold longer serum half-life compared with epoetin alfa, the most used isoform [95]. Epo and Darbe are termed as erythropoiesis-stimulating agents (ESAs) [96].
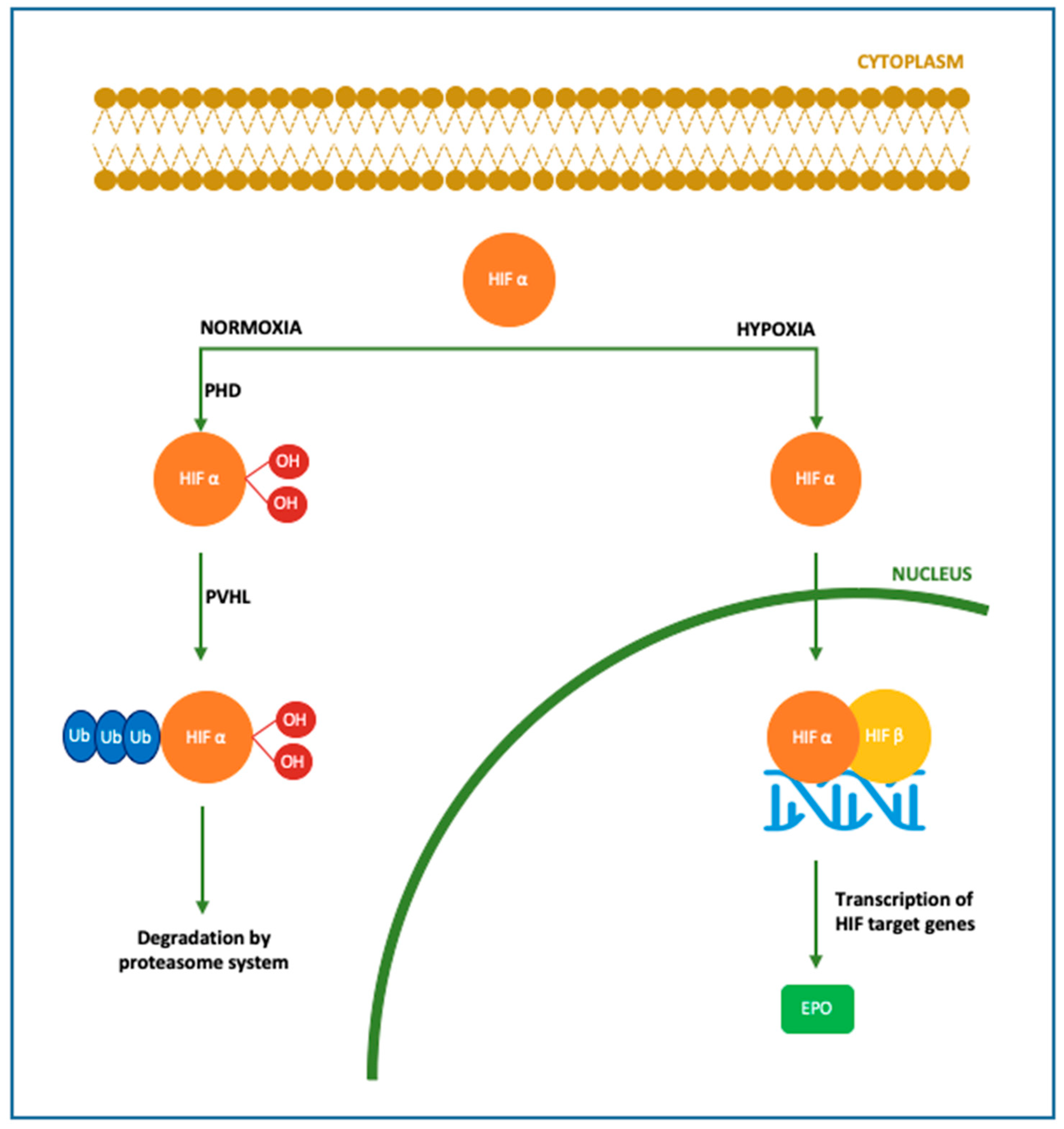
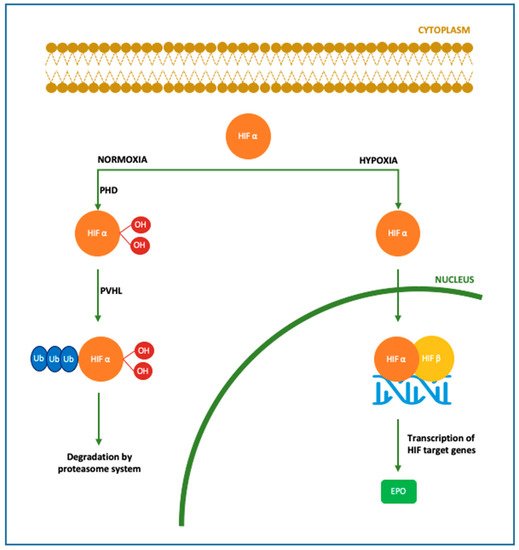
Figure 1. Molecular mechanism of Epo production. In the brain Epo production is upregulated by oxygen levels mainly in astrocytes, followed by oligodendrocytes, endothelial cells and microglia. In case of normoxia, cytoplasmic HIFα is hydroxylated and polyubiquitinated by PHD and pVHL, respectively. In this form, HIF is degraded by the proteasome system. In case of hypoxia, HIFα is dehydroxylated and deubiquinated, thus able to translocate into the nucleus and bind HIF β, inducing the transcription of its target genes among which Epo gene [16][17][18][43].
Molecular mechanism of Epo production. In the brain Epo production is upregulated by oxygen levels mainly in astrocytes, followed by oligodendrocytes, endothelial cells and microglia. In case of normoxia, cytoplasmic HIFα is hydroxylated and polyubiquitinated by PHD and pVHL, respectively. In this form, HIF is degraded by the proteasome system. In case of hypoxia, HIFα is dehydroxylated and deubiquinated, thus able to translocate into the nucleus and bind HIF β, inducing the transcription of its target genes among which Epo gene [70,71,72,97].
HIF
:
hypoxia
-
inducible factor
;
PHD
:
prolyl
-
4
-
hydroxylases
;
PVHL
:
von Hippel
–
Lindau protein.
.
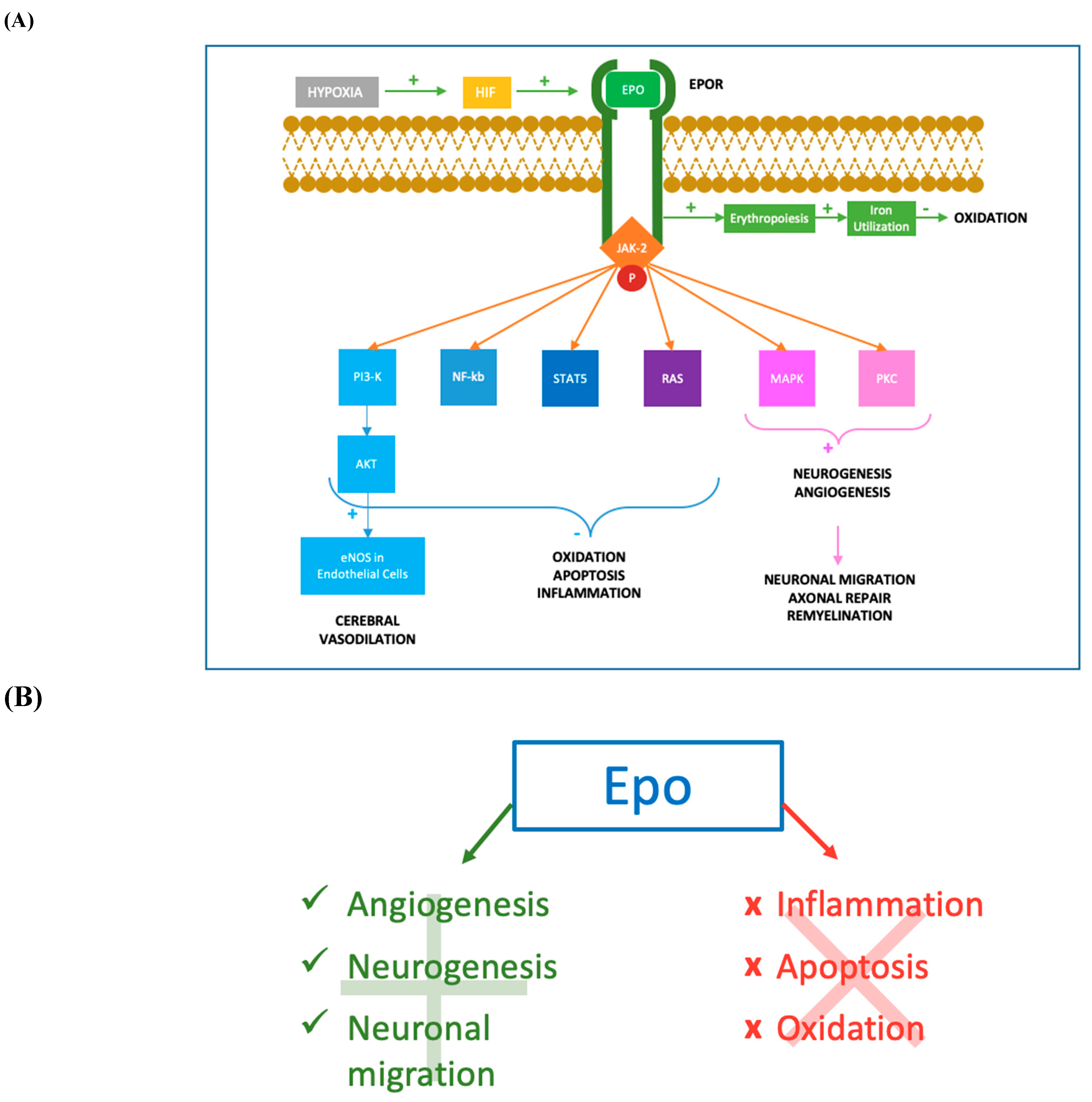
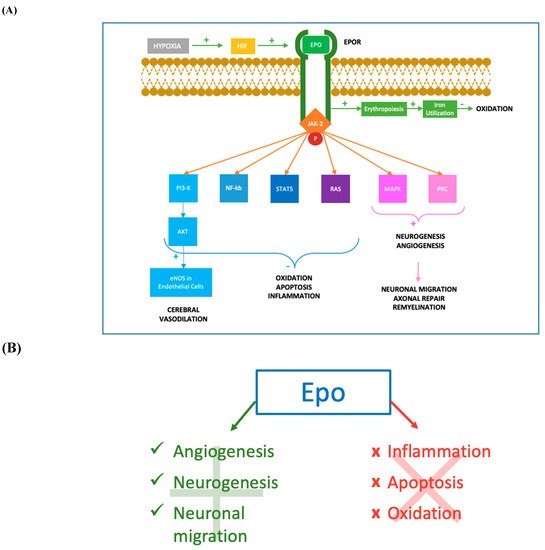
Figure 2.
Molecular mechanisms of Epo action. (
A
) After hypoxia, the production of HIF determines an augmented synthesis of Epo which binds to its transmembrane receptor EpoR. The cytoplasmic tail of the Epo-EpoR complex phosphorylates JAK2, which activates a complex cascade of signalling pathways. The activation of PI3K/AKT pathway leads to the increase of eNOS activity in endothelial cells, determining augmented levels of NO and cerebral vasodilation. PI3K/AKT, together with NF-kb, STAT-5 and RAS pathways, reduces inflammation, oxidation and apoptosis acting both at nuclear and intramitochondrial levels. Moreover, MAPK and PKC mediated mechanisms promote neurogenesis and angiogenesis in damaged tissues. Neurogenesis, especially oligodendrogenesis, facilitates the process of remyelination and axonal repair, while angiogenesis permits flow restoration and migration of neuronal progenitors in the ischemic areas. The erythropoietic effect of Epo-EpoR binding is an additional antioxidant mechanism, increasing iron utilization resulting in a lower iron oxidant potential. JAK-2: Janus-tyrosine-kinase-2; PI3K: phosphoinositide 3-kinase; AKT: v-akt murine thymoma viral oncogene homolog; eNOS: endothelial nitric oxide synthase; NO: nitric oxide; NF-kb: nuclear factor kappa-light-chain-enhancer of activated B cells; STAT-5: signal transducer and activator of transcription 5; RAS: rat sarcoma; MAPK: mitogen-activated protein kinase; PKC: protein kinase C. (
B) Mechanisms promoted and inhibited following Epo treatment. Epo has shown anti-apoptotic [19][20][21], antioxidant [22][23][24] and anti-inflammatory properties [25][26][27][28][29]. Epo promotes angiogenesis [20][32][33], oligodendrogenesis, neuronal progenitors migration in the ischemic areas (Wang et al., 2004; Ohab et al., 2006; Li et al., 2007) and neurogenesis [34][35][36][37].
2. Erythropoietin in Preterm Infants
Erythropoietin has been administered to preterm infants since 1990 for haematological purposes. In fact, Epo has been extensively used for the prevention of anemia of prematurity, but the discovery of the potential role as a neuroprotective agent suggested new purposes for its administration [44][45][46]. In the last few decades the survival of preterm infants has dramatically grown, yet this population is still exposed to a great incidence of neurodevelopmental impairment [47][48]. Trials conducted in animal models have shown neuroprotective effects of Epo, thus clinical studies investigating Epo’s new potential benefits in premature babies have followed [49][50][51][52][53]. In particular, it has been described that Epo administration in preterm is able to protect neurons and oligodendrocytes from apoptosis, prevent inflammation and promote neurogenesis and angiogenesis [54][55]. Preterm infants benefit by a prolonged treatment during the period of oligodendrocyte maturation, between 24 and 32 weeks [49][56][57], in which Epo exerts a neuroprotective function. Evidence in newborns and animal models suggest neuroprotective effects at doses >200 U/kg [58]. Cumulative doses have been associated with more beneficial effects compared to a single-dose administration [59]. The dosage of EPO ranged from 250 to 3000 UI/kg in all studies. Darbe alfa was administered at 10 mcg/Kg sc [60][61][62]. The population target was represented of extremely and very preterm babies (gestational age below 32 weeks or BW < 1500 gr). Only three clinical trials focused on the role of Epo in extremely preterm infants (gestational age below 28 weeks or 1000 gr) [63][64][65]. Erythropoietin administration was proved to be safe in all preterm infants, not affecting mortality rate and major adverse effects occurrence in the short and long term [64][65][66]. These data confirmed previous analyses on animal models [59][67][68]. Out of 16, 10 trials performed clinical neurodevelopmental outcome evaluated mainly in the first years of life. No uniform results were reported. In addition, neurodevelopmental outcomes were not assessed in all trials in which neuroimaging was performed. It has been well recognized that a correlation between white matter injuries and neurodevelopmental outcome, in terms of increased incidence of cerebral palsy, motor and cognitive delay exists [69][70][71][72]. In addition, values of fractional anisotropy of the corpus callosum assessed using TBSS have been reported to directly correlate with motor and cognitive outcomes [73]. Thus, neuroimaging alterations have been related with poorer neurodevelopmental outcomes [41][60][61][74][75]. Studies on Epo treated very preterm newborns highlighted an improved white matter development and a weak but widespread effect in the overall structural connectivity network after Epo treatment [76][77]. Yet, no difference for any brain metabolite has been reported in very preterm treated group [61].3. Erythropoietin in HIE
After several years of studies conducted in animal models, in 2009 the first trial of Epo administration as adjuvant therapy with TH in newborns affected by HIE was published. The research underlined Epo favourable effects, paving the way to further studies [78]. Since then Epo showed beneficial effects during the secondary energy failure and the tertiary phases of HIE [79]. The therapeutic scheme is influenced by the type of damage [56]. In HIE term newborns high Epo doses are more effective when the injury has not been established yet [49][56][57]. Evidence from animal models have shown that Epo should be administered at high doses within 6 h after the onset of brain injury to reach a substantial neuroprotective effect [80]. In this context, Epo may influence the mechanisms of cerebral flow restoration, neovascularization and neuroregeneration, limiting the ischemic damage [81]. The analysis revealed that Epo administration was safe and well tolerated [78], confirming previous findings in animal models [51][59][68]. The passage through the BBB is an essential issue to be considered for any neuroprotective drug given systemically. Erythropoietin presents a molecular weight too high to be carried across the BBB through the lipid mediated transport [78]. Transport of Epo through the BBB is mediated by a specific receptor-facilitated process [15] as well as a time, dose and peak serum concentration-dependent mechanism [82][83]. Furthermore, the alteration of BBB permeability caused by asphyxia determines in patient with HIE an easier passage from serum to cerebrospinal fluid [84]. In the studies analysed, Epo administration is followed by a higher concentration of Epo in the cerebrospinal fluid compared to HIE controls, thus confirming the increased levels are due to the contribution of Epo exogenous administration [78]. Administration of Epo has shown some advantages compared to TH treatment. Treatment with Epo implies easier technical performance, with less side effects [78][85]. Moreover, Epo treatment is effective if administered within 48 h of life, differently from TH which must be initiated within the first 6 h of life [78]. Thus, Epo treatment has been proposed as both an alternative therapy or combined treatment with TH [78][85]. In all the protocols comparing Epo vs. placebo or Epo associated with TH vs. supportive therapy, Epo treatment determined a lower death rate and improved neurologic outcomes [85][86][87][88][89][90]. Valera et al. treated 15 HIE neonates with EPO for two weeks, starting within three hours from birth along with TH. At 18 months, there was 80% survival with no neurodevelopmental disability. Unfortunately, there was no control group for comparison [91]. Rogers et al. recruited 24 newborns with HIE and administered Epo 24 h after HIE combined with standard TH. The researchers found that significant neurodevelopmental disability occurred in only 12.5% of infants with moderate to severe MRI changes who received Epo plus TH, compared to 70–80% significant disability or death in infants treated with TH alone. However, these results were not statistically significant as the number of infants was too small [92]. The Phase II clinical trial on newborns with HIE reported better 12-months motor outcomes for treatment with Epo plus TH compared to TH alone [90]. A randomized case-control study by Wu et al. [89] evaluating 24 newborns treated with Epo and TH for moderate/severe HIE, showed a significantly reduced brain injury on MRI at 5 days-of-age and better 12-months motor outcomes compared to the 26 infants who received TH as a standard routine measure for HIE. The Epo treatment was also associated with an antioxidant effect and an increase of neuroprotective factors [85][86]. The study by Wang et al. clearly demonstrated the protection from the damage resulting from asphyxia through inhibiting apoptosis, reducing oxygen free radicals and enhancing antioxidant capacity. In this research trial, 34 newborns received Epo and Vitamin C plus TH compared to 34 newborns receiving conventional treatment plus ascorbic acid. There were lower oxidative stress index levels and higher antioxidant enzymes in both groups after treatment, with better results in the group treated with Epo. Moreover, lower pro-apoptotic molecules and higher anti-apoptotic molecules were found in both groups after treatment, with better results again in the group treated with Epo [93]. In addition, MRI analysis confirmed the beneficial effect of Epo in the reduction of brain injury, both if administered alone [87] or combined with TH [90]. Despite all these data, the optimal dosage and administration regimens for the treatment of HIE in newborns still needs to be defined [78][85][92].4. Erythropoietin in Neonatal Stroke
At the diagnosis of neonatal stroke, the damage has already been established and the reparation mechanisms are not fully known, thus nowadays acute therapies for perinatal strokes are still not available [94]. Currently the management of the disease is mainly supportive, based on the treatment of complications, such as antiepileptic therapy, and on the improvement of neurologic chronic sequelae through rehabilitation [95]. Erythropoietin has become one of the most remarkable neuroprotective strategy since Sakanaka et al. reported for the first time the role of Epo as a neuroprotective agent in the ischemic brain damage [96]. Recent researches are focused on new approaches including the administration of adjuvant neuroprotective therapies, with the aim to enhance endogenous mechanisms of repair and angiogenesis [97][98]. The safety profile of Epo administration was also confirmed in the studies on neonatal stroke. This is consistent with previous data available from animal models and preterm and HIE-suffering newborns, which showed a good tolerance of treatment with Epo in those populations [45][80][99][100]. The brain MRI evaluation in both studies didn’t find a beneficial effect of Epo treatment on stroke volume [101][102]. Furthermore, Epo treatment was not associated with an overall difference in neurodevelopmental outcome, at 3 months and one year follow up respectively with Griffiths’ scale and BSID-III [101][102]. These data are in contrast with most of the newborn stroke animal models in which several neuroprotective effects and reduction of stroke volume induced by Epo are described [7][49][103][104]. Recently, a delayed Epo therapy administered to mice model with middle brain artery occlusion stroke reported to uphold brain volume and to improve behavioural and sensorimotor functions, compared with placebo-treated animals [7]. The discrepancy between the experimental animal model and clinical trials may be due to the small neonatal study population, as the trials are both phase I and II studies. Furthermore, Andropoulos and colleagues found that six enrolled newborns presented microdeletions at the chromosome 22q11.2 region, a condition known to be linked to a variable degree on neurodevelopmental impairment in a syndromic condition [105]. Another limiting factor is the therapeutic window, as the beneficial effect is limited to specific time after injury [106]. One interventional study used Epo after stroke diagnosis, which is usually done 24–48 h after cerebral vascular accident. The use of specific biomarkers that will increase within the first hours of life in hypoxic-ischemic injury may help in the early diagnosis of stroke, allowing a prompt identification of neonates who may qualify for neuroprotection. Finally, the variability in period and tests used to assess the neurodevelopmental outcome may represent a weakness and suggests that scores should be interpreted with caution. Since the determinants of cognitive outcomes at school age are multifactorial, the predictive value of tests administered at age < 24 months might never approach 100%.) Mechanisms promoted and inhibited following Epo treatment. Epo has shown anti-apoptotic [73,74,75], antioxidant [76,77,78] and anti-inflammatory properties [79,80,81,82,83]. Epo promotes angiogenesis [74,86,87], oligodendrogenesis, neuronal progenitors migration in the ischemic areas (Wang et al., 2004; Ohab et al., 2006; Li et al., 2007) and neurogenesis [88,89,90,91].
2. Erythropoietin in Preterm Infants
Erythropoietin has been administered to preterm infants since 1990 for haematological purposes. In fact, Epo has been extensively used for the prevention of anemia of prematurity, but the discovery of the potential role as a neuroprotective agent suggested new purposes for its administration [127,128,129].
In the last few decades the survival of preterm infants has dramatically grown, yet this population is still exposed to a great incidence of neurodevelopmental impairment [7,8]. Trials conducted in animal models have shown neuroprotective effects of Epo, thus clinical studies investigating Epo’s new potential benefits in premature babies have followed [130,131,132,133,134]. In particular, it has been described that Epo administration in preterm is able to protect neurons and oligodendrocytes from apoptosis, prevent inflammation and promote neurogenesis and angiogenesis [135,136]. Preterm infants benefit by a prolonged treatment during the period of oligodendrocyte maturation, between 24 and 32 weeks [2,130,137], in which Epo exerts a neuroprotective function. Evidence in newborns and animal models suggest neuroprotective effects at doses >200 U/kg [138]. Cumulative doses have been associated with more beneficial effects compared to a single-dose administration [139].
The dosage of EPO ranged from 250 to 3000 UI/kg in all studies. Darbe alfa was administered at 10 mcg/Kg sc [98,99,104].
The population target was represented of extremely and very preterm babies (gestational age below 32 weeks or BW < 1500 gr). Only three clinical trials focused on the role of Epo in extremely preterm infants (gestational age below 28 weeks or 1000 gr) [102,103,112].
Erythropoietin administration was proved to be safe in all preterm infants, not affecting mortality rate and major adverse effects occurrence in the short and long term [103,108,112]. These data confirmed previous analyses on animal models [139,140,141].
Out of 16, 10 trials performed clinical neurodevelopmental outcome evaluated mainly in the first years of life. No uniform results were reported.
In addition, neurodevelopmental outcomes were not assessed in all trials in which neuroimaging was performed. It has been well recognized that a correlation between white matter injuries and neurodevelopmental outcome, in terms of increased incidence of cerebral palsy, motor and cognitive delay exists [15,16,142,143]. In addition, values of fractional anisotropy of the corpus callosum assessed using TBSS have been reported to directly correlate with motor and cognitive outcomes [144]. Thus, neuroimaging alterations have been related with poorer neurodevelopmental outcomes [95,98,99,106,145]. Studies on Epo treated very preterm newborns highlighted an improved white matter development and a weak but widespread effect in the overall structural connectivity network after Epo treatment [110,111]. Yet, no difference for any brain metabolite has been reported in very preterm treated group [99].
3. Erythropoietin in HIE
After several years of studies conducted in animal models, in 2009 the first trial of Epo administration as adjuvant therapy with TH in newborns affected by HIE was published. The study underlined Epo favourable effects, paving the way to further studies [116]. Since then Epo showed beneficial effects during the secondary energy failure and the tertiary phases of HIE [146].
The therapeutic scheme is influenced by the type of damage [2]. In HIE term newborns high Epo doses are more effective when the injury has not been established yet [2,130,137]. Evidence from animal models have shown that Epo should be administered at high doses within 6 h after the onset of brain injury to reach a substantial neuroprotective effect [147]. In this context, Epo may influence the mechanisms of cerebral flow restoration, neovascularization and neuroregeneration, limiting the ischemic damage [148].
Our analysis revealed that Epo administration was safe and well tolerated [116], confirming previous findings in animal models [132,139,141].
The passage through the BBB is an essential issue to be considered for any neuroprotective drug given systemically. Erythropoietin presents a molecular weight too high to be carried across the BBB through the lipid mediated transport [116]. Transport of Epo through the BBB is mediated by a specific receptor-facilitated process [69] as well as a time, dose and peak serum concentration-dependent mechanism [149,150]. Furthermore, the alteration of BBB permeability caused by asphyxia determines in patient with HIE an easier passage from serum to cerebrospinal fluid [151]. In the studies analysed, Epo administration is followed by a higher concentration of Epo in the cerebrospinal fluid compared to HIE controls, thus confirming the increased levels are due to the contribution of Epo exogenous administration [116].
Administration of Epo has shown some advantages compared to TH treatment. Treatment with Epo implies easier technical performance, with less side effects [116,121]. Moreover, Epo treatment is effective if administered within 48 h of life, differently from TH which must be initiated within the first 6 h of life [116]. Thus, Epo treatment has been proposed as both an alternative therapy or combined treatment with TH [116,121].
In all the protocols comparing Epo vs. placebo or Epo associated with TH vs. supportive therapy, Epo treatment determined a lower death rate and improved neurologic outcomes [117,119,120,121,122,123]. Valera et al. treated 15 HIE neonates with EPO for two weeks, starting within three hours from birth along with TH. At 18 months, there was 80% survival with no neurodevelopmental disability. Unfortunately, there was no control group for comparison [152].
Rogers et al. recruited 24 newborns with HIE and administered Epo 24 h after HIE combined with standard TH. The authors found that significant neurodevelopmental disability occurred in only 12.5% of infants with moderate to severe MRI changes who received Epo plus TH, compared to 70–80% significant disability or death in infants treated with TH alone. However, these results were not statistically significant as the number of infants was too small [118]. The Phase II clinical trial on newborns with HIE reported better 12-months motor outcomes for treatment with Epo plus TH compared to TH alone [123]. A randomized case-control study by Wu et al. [122] evaluating 24 newborns treated with Epo and TH for moderate/severe HIE, showed a significantly reduced brain injury on MRI at 5 days-of-age and better 12-months motor outcomes compared to the 26 infants who received TH as a standard routine measure for HIE. The Epo treatment was also associated with an antioxidant effect and an increase of neuroprotective factors [117,121]. The study by Wang et al. clearly demonstrated the protection from the damage resulting from asphyxia through inhibiting apoptosis, reducing oxygen free radicals and enhancing antioxidant capacity. In this research trial, 34 newborns received Epo and Vitamin C plus TH compared to 34 newborns receiving conventional treatment plus ascorbic acid. There were lower oxidative stress index levels and higher antioxidant enzymes in both groups after treatment, with better results in the group treated with Epo. Moreover, lower pro-apoptotic molecules and higher anti-apoptotic molecules were found in both groups after treatment, with better results again in the group treated with Epo [153].
In addition, MRI analysis confirmed the beneficial effect of Epo in the reduction of brain injury, both if administered alone [119] or combined with TH [123]. Despite all these data, the optimal dosage and administration regimens for the treatment of HIE in newborns still needs to be defined [116,118,121].
4. Erythropoietin in Neonatal Stroke
At the diagnosis of neonatal stroke, the damage has already been established and the reparation mechanisms are not fully known, thus nowadays acute therapies for perinatal strokes are still not available [154]. Currently the management of the disease is mainly supportive, based on the treatment of complications, such as antiepileptic therapy, and on the improvement of neurologic chronic sequelae through rehabilitation [155]. Erythropoietin has become one of the most remarkable neuroprotective strategy since Sakanaka et al. reported for the first time the role of Epo as a neuroprotective agent in the ischemic brain damage [156]. Recent researches are focused on new approaches including the administration of adjuvant neuroprotective therapies, with the aim to enhance endogenous mechanisms of repair and angiogenesis [157,158].
The safety profile of Epo administration was also confirmed in the studies on neonatal stroke. This is consistent with previous data available from animal models and preterm and HIE-suffering newborns, which showed a good tolerance of treatment with Epo in those populations [128,147,159,160].
The brain MRI evaluation in both studies didn’t find a beneficial effect of Epo treatment on stroke volume [125,126]. Furthermore, Epo treatment was not associated with an overall difference in neurodevelopmental outcome, at 3 months and one year follow up respectively with Griffiths’ scale and BSID-III [125,126].
These data are in contrast with most of the newborn stroke animal models in which several neuroprotective effects and reduction of stroke volume induced by Epo are described [61,130,161,162]. Recently, a delayed Epo therapy administered to mice model with middle brain artery occlusion stroke reported to uphold brain volume and to improve behavioural and sensorimotor functions, compared with placebo-treated animals [61].
The discrepancy between the experimental animal model and clinical trials may be due to the small neonatal study population, as the trials are both phase I and II studies. Furthermore, Andropoulos and colleagues found that six enrolled newborns presented microdeletions at the chromosome 22q11.2 region, a condition known to be linked to a variable degree on neurodevelopmental impairment in a syndromic condition [163].
Another limiting factor is the therapeutic window, as the beneficial effect is limited to specific time after injury [164]. One interventional study used Epo after stroke diagnosis, which is usually done 24–48 h after cerebral vascular accident. The use of specific biomarkers that will increase within the first hours of life in hypoxic-ischemic injury may help in the early diagnosis of stroke, allowing a prompt identification of neonates who may qualify for neuroprotection.
Finally, the variability in period and tests used to assess the neurodevelopmental outcome may represent a weakness and suggests that scores should be interpreted with caution. Since the determinants of cognitive outcomes at school age are multifactorial, the predictive value of tests administered at age < 24 months might never approach 100%.