Since the first case of viral pneumonia was reported from Wuhan, China in late December of 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative pathogen for the Coronavirus disease 2019 (COVID-19) pandemic, has run rampant across the world [
Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 4 by Dean Liu and Version 3 by Dean Liu.
Coronavirus disease 2019 (COVID-19), a respiratory syndrome caused by SARS-CoV-2, can be transmitted through respiratory droplets and aerosols of droplet nuclei. Aerosol-generating medical procedures (AGMP) are needed to take care of critically ill patients but place health care providers at risk of infection. With limited supplies of personal protective equipment (PPE), barrier systems were developed to help protect health care providers during tracheal intubation. The video intubating stylet shows promise to become the preferred intubation device in conjunction with plastic sheet barriers during the COVID-19 pandemic.
- COVID-19
- endotracheal intubation
- tracheal intubation
- video intubating stylet
- plastic sheet
- barrier
1. Introduction
Since the first case of viral pneumonia was reported from Wuhan, China in late December of 2019, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative pathogen for the Coronavirus disease 2019 (COVID-19) pandemic, has run rampant across the world
1]. As of 30 September 2021, there have been 232,636,622 confirmed cases and 4,762,089 COVID deaths
]. As of 30 September 2021, there have been 232,636,622 confirmed cases and 4,762,089 COVID deaths
[2]. As cases grew at an alarmingly exponential rate, it was quickly identified that COVID-19 could be transmitted through respiratory droplets and even through the aerosolization of droplet nuclei
]. As cases grew at an alarmingly exponential rate, it was quickly identified that COVID-19 could be transmitted through respiratory droplets and even through the aerosolization of droplet nuclei
[3][4]. Because of the pathology and progression of the disease towards respiratory failure, aerosol-generating medical procedures (AGMP) such as laryngoscopy, endotracheal intubation and extubation, tracheostomy, bronchoscopy and bronchoalveolar lavage, positive pressure ventilation, cardiopulmonary resuscitation with bag-valve-mask, suctioning, and nasopharyngeal aspiration and washing would be necessary to take care of patients with COVID-19 infection
]. Because of the pathology and progression of the disease towards respiratory failure, aerosol-generating medical procedures (AGMP) such as laryngoscopy, endotracheal intubation and extubation, tracheostomy, bronchoscopy and bronchoalveolar lavage, positive pressure ventilation, cardiopulmonary resuscitation with bag-valve-mask, suctioning, and nasopharyngeal aspiration and washing would be necessary to take care of patients with COVID-19 infection
[5]. Healthcare providers in the fields of anesthesiology, critical care medicine, emergency medicine, and otolaryngology, because of their roles in performing AGMPs for these patients, found themselves at risk of infection.
2. The Development of Barrier Systems
Personal protective equipment (PPE) is the primary basis for prevention of infection to healthcare workers while performing their tasks. Necessary PPE during the COVID-19 pandemic includes medical-grade masks, respirators, goggles, eye shields, face shields, gowns, gloves, shoe coverings, and head coverings [6] (Figure 1). Strict donning and doffing procedures are necessary to avoid accidental contamination of other work areas and the transmission to other patients and staff in the hospital [7]. It was quickly realized that there were not sufficient stores of PPE to safely allow healthcare providers to perform daily patient care during the pandemic [8]. Industry had a hard time ramping up production in a timely manner, and global disparities existed and have continued to exist. Without adequate PPE, coupled with other factors such as a lack of available testing, especially during the early stages of the pandemic [9], the growing number of confirmed and suspected cases, as well as an overwhelming workload, frontline medical workers endured significant anxiety performing their expected duties as they worried about becoming infected, as well as transmitting the disease to family members [10]. Currently, over 18 months into the pandemic, even with the rollout of vaccines, challenges to their widespread deployment as well as the proliferation of COVID-19 variants have prevented the world from curtailing the disease [11].

Figure 1. Examples of personal protective equipment (PPE) used by medical staff while caring for patients undergoing aerosol generating medical procedures (AGMP) during the COVID-19 pandemic.
Without adequate PPE, health care professionals quickly looked to alternative means of protection against viral transmission. One strategy was the use of a transparent physical barriers. The first reported model was designed by a Taiwanese anesthesiologist who constructed a transparent four-sided box made of plexiglass that was placed between the patient and the airway manager during tracheal intubation [12] (Figure 2A). The plans for this structure were quickly shared on social media [13], and Canneli et al. were the first to report on its use in the scientific literature [14]. Subsequently, after this idea was promoted by news and social media and the device was proliferated and distributed to some users, multiple variations of barrier devices were introduced [15][16][17][18][19][20][21]. These barriers were applied not just for endotracheal intubation and airway management (Figure 2B,C) but were utilized in various aspects of medical care, as well as applied to facilitate other forms of human interaction during the pandemic (Figure 3). On 1 May 2020, the United States Food and Drug Administration (FDA) issued an emergency use authorization (EUA) for protective barrier enclosures [22]. Over time, three general device types were identified: (1) rigid transparent box, (2) plastic sheet with frame, and (3) plastic sheet without frame (Figure 2).
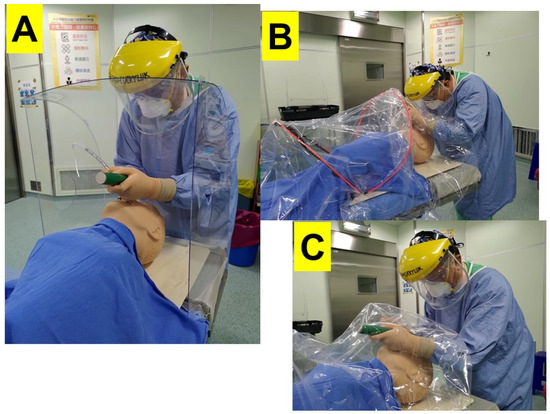
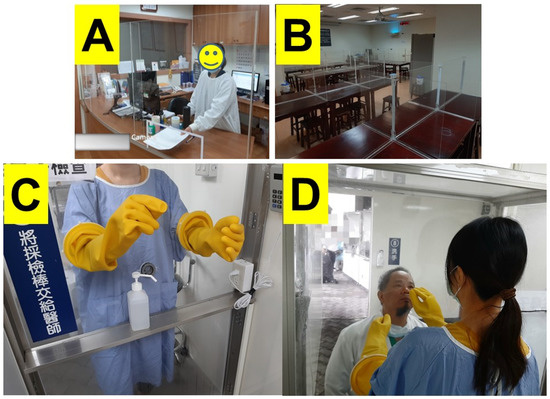
Figure 2. Various barrier systems utilized during performance of direct laryngoscopy and endotracheal intubation. (A) Rigid plastic box, (B) Plastic sheet with frame, (C) Plastic sheet without frame.
Figure 3. Various applications of transparent plastic barriers during the COVID-19 pandemic. (A) Front desk, (B) Cafeteria, (C,D) Nasopharyngeal COVID-19 testing.
Meanwhile, some airway management experts expressed their serious concerns on such a MacGyverism-style improvised medical device (e.g., the “aerosol box”) and argued about the untested effectiveness and safety issues of this EUA device [23][24][25][26][27]. The main concerns raised against such physical barrier enclosure include the following: (1) restriction of hand movement of the intubator and assistants; (2) heavy and bulky plexiglass is difficult to carry and position or reposition in emergency situations; (3) limited for certain body habitus and positions; (4) confined space for airway maneuvering; (5) ergonomically difficult to manipulate airway equipment; (6) introducing other new risks of cross-contamination during the use, disinfection, and disposal processes; (7) increases the cognitive load of the staff and the risk of subsequent contamination; and (8) breaches in PPE due to a tear cut by the box edge. Some pointed out that such an unvalidated box design does not reduce risks (of being infected) and probably has unintended safety consequences to the airway managers, medical staff, and the patients.
3. Tracheal Intubation during the COVID-19 Pandemic
Tracheal or endotracheal intubation, the process of placing a breathing tube in the patient’s airway in order to maintain patency of the airway and provide oxygenation and ventilation, is often necessary in patients with critical respiratory illness [28]. Traditionally, the intubation process involves manipulating the head and neck to align the oral, laryngeal, and pharyngeal axes, the placement of a laryngoscope into the oropharynx to retract the tongue and soft tissues of the mouth, and the introduction of an endotracheal tube (ETT), loaded onto a stylet, past the glottic opening [29]. This procedure can be performed by a single operator, but an assistant often helps with the optimization of patient positioning such as jaw lift and lip retraction, handing the ETT-mounted stylet to the intubator, removing the stylet after the ETT has passed the vocal cords, and/or inflating the cuff of the endotracheal tube.
The intubation process places the healthcare professional at risk for COVID-19 infection as during traditional direct laryngoscopy, the anesthesia provider may need to be very close to the patient’s mouth in order to obtain a view of the glottis to advance the ETT (Figure 2 and Figure 4A). During the COVID-19 pandemic, it was subsequently recommended that videolaryngoscopy be preferentially utilized for tracheal intubation [5][30][31]. The technology behind a videolaryngoscope is that a camera is placed at the tip of the device, which is projected to a monitor, either mounted on the device itself or on an independent stand. The airway manager is able to obtain a view of the patient’s airway and guide the ETT through the patient’s glottis without placing his or her face in close proximity to the patient’s airway (Figure 4B). A recent Cochrane review had concluded that videolaryngoscopy may improve the success of tracheal intubation in adult patients, especially in difficult airways situations [32]. However, it should be noted that because of the significant increased costs of a videolaryngoscope, this device may not be available in every setting across the world.
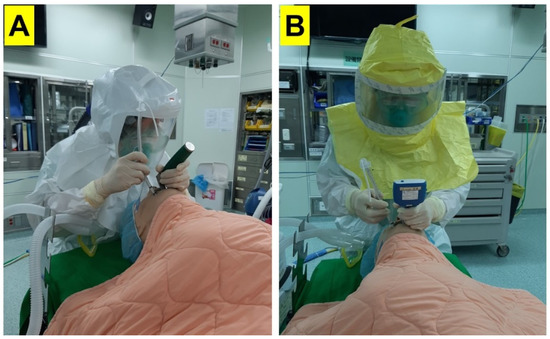
Figure 4. Proximity of the anesthesia provider to the patient’s airway during: (A) direct laryngoscopy, (B) indirect laryngoscopy using a videolaryngoscope (Courtesy photos reproduced from Cell Transplantation, SAGE Journals).
There are many videolaryngoscopes on the market today, with regional preferences in a range of designs and costs. A subset of the videolaryngoscope is the video intubating stylet. This device is a rigid or semi-rigid stylet equipped with a camera at the tip projecting to a separate monitor (Figure 5 and Figure 6). The ETT is mounted onto the video stylet in a similar fashion to a traditional stylet. The tip of the stylet may be designed to be malleable and anteflex. Because the camera resides within the stylet as opposed to on a separate videoscope, a laryngoscope is not necessary to perform endotracheal intubation (Figure 6 and Figure 7). “To see is to intubate” and “to see is to believe” are the mottos of the design of a video-assisted intubating stylet, a pioneering work that could change the face of airway management [33].
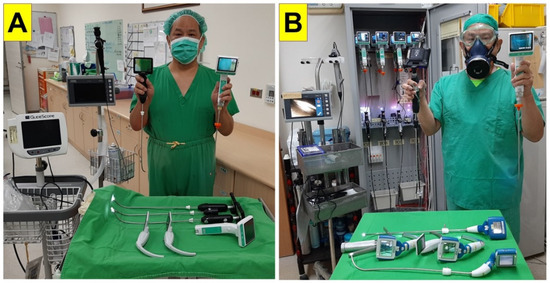
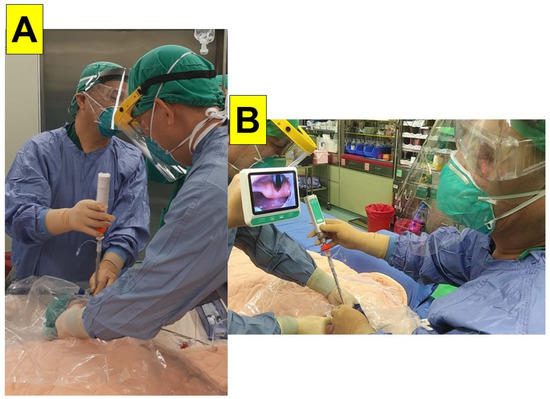
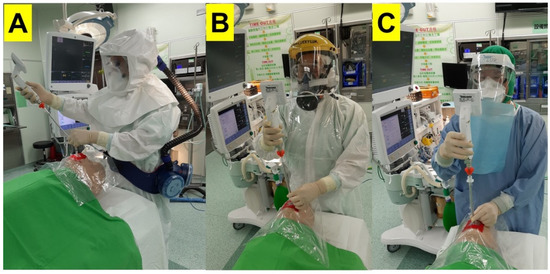
Figure 5. Prevalence of using video intubating stylet technique for tracheal intubation in Taiwan. (A) Department of Anesthesia in a 729-bed community hospital; (B) Department of Anesthesia in a 1110-bed tertiary medical Center.
Figure 6. Real-world demonstration of endotracheal intubation utilizing the video intubating stylet and plastic sheet. A camera on the tip of the stylet captures a view of the glottis, which is projected to a separate monitor (For a demonstration video clip, see Supplementary Material). (A) Front view; (B) Side view.
Figure 7. Mannequin demonstration of endotracheal intubation using the video intubating stylet through a piece of plastic sheet. (A) Stylet with loaded endotracheal tube introduced into patient’s mouth. (B) Stylet directed towards vocal cords under visual guidance from the monitor on the proximal end. (C) Endotracheal tube advanced off the stylet once past the vocal cords. PPE with powered air-purifying respirator, P-100, and N-95 respirators were shown in this figure. (Courtesy photos reproduced from Asian Journal of Anesthesiology, Taiwan Society of Anaesthesiologists with permission).
A potential benefit of the intubating stylet is that it may be a more economical alternative to the videolaryngoscope. In addition, many videolaryngoscopes utilize disposal laryngoscope tips/blades, which can minimize infection but are also recurring costs. Other potential benefits of the intubating stylet include a small profile, which results in less overall patient airway manipulation, such as less opening of the mouth and less lifting of the tongue. Because of its slim profile, the video stylet is more easily sanitized compared to other videolaryngoscopes. Even prior to the COVID-19 pandemic, at many institutions, the video intubating stylet had become the preferred modality for performing tracheal intubation [34][35][36][37]. Table 1 and Figure 5 show examples of high use coverage of video-assisted intubating stylets in the departments of anesthesia in Taiwan. Moreover, among 24 medical centers in Taiwan, the departments of anesthesia in 20 of them are equipped with video-assisted intubating stylets.
Table 1. Use coverage of video-assisted intubating stylet in the Hualien Tzu-Chi Medical Center, Hualien, Taiwan.
| 2016 | 2017 | 2018 | 2019 | 2020 | |
|---|---|---|---|---|---|
| Anesthesia Number | 16,077 | 17,831 | 17,998 | 19,307 | 19,721 |
| General Anesthesia Number | 15,339 | 16,893 | 17,497 | 18,481 | 19,009 |
| Laryngeal Mask Airway Number | 5544 | 5134 | 5816 | 5902 | 5863 |
| Endotracheal Tube Number | 5953 | 6504 | 6920 | 6966 | 7418 |
| Video Laryngoscope Number | 0 | 0 | 20 | 100 | 635 |
| Video Intubating Stylet Number | 5953 (100%) |
6504 (100%) |
6900 (99.7%) |
6866 (98.6%) |
6783 (91.4%) |
This hospital is a tertiary medical center in the east coast of Taiwan. There are 1110 beds, 1788 personnel, 20 operation rooms, 13 attending anesthesiologists, and 45 certified registered nurse anesthetists. The COVID-19 outbreak and pandemic started since December 2020.
4. Combining Barrier Systems with the Video Intubating Styletd
When incorporating a barrier system with the video stylet, the length of the intubating stylet precludes its use within a rigid barrier box (Figure 8), unless the box is drastically modified to accommodate the length of the intubating stylet. This may not be practical to manufacture, and the added height might also make the box difficult to handle as well as a safety concern to patients and medical staff. Additionally, the semi-rigid stylet is not long or flexible enough to be handled from outside the barrier box through the hand orifices at the head of the patient. It was quickly realized that the plastic sheet was the only barrier system that could be practically utilized with the video intubating stylet [38][39][40].
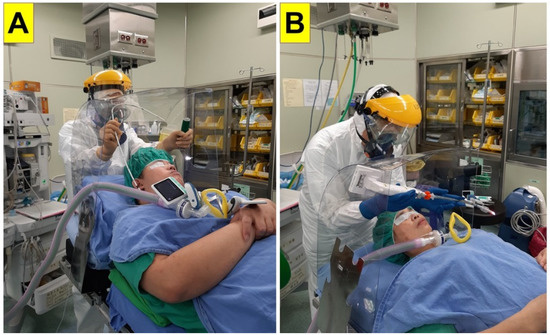
Figure 8. The plastic barrier box seriously limits the ability to perform endotracheal intubation utilizing: (A) the video-laryngoscope or conventional direct laryngoscope and bougie; a BMI-38 model in a ramp position; and (B) the video intubating stylet; a BMI-24 model in a neutral supine position. BMI: body mass index.
There are several ways that the plastic sheet can be utilized to protect the anesthesia provider. In its simplest unmodified form, the plastic sheet could be laid across the patient’s head to function as a general barrier. The health care professional subsequently reaches under to the sheet to perform tracheal intubation (Figure 2C). Because of its malleability and transparency, other maneuvers not involving the airway itself, such as an assistant providing jaw lift, can be performed over the sheet (Figure 9). If the plastic sheet hampers the ability of the anesthesia provider to successfully intubate the patient, the sheet can be easily and rapidly removed, as opposed to the bulkier and heavier plastic box. Table 2 summarized the advantages and disadvantages of plastic sheet barriers design and aerosol box design.
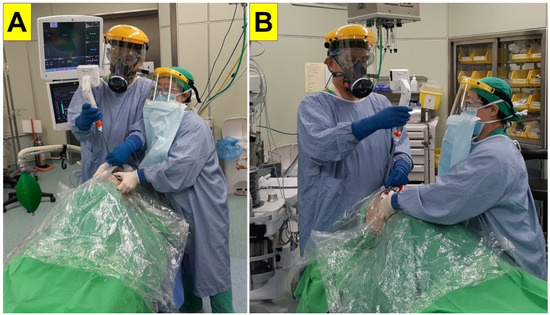
Figure 9. Endotracheal intubation utilizing a video intubating stylet with an assistant providing mouth opening and jaw lift over a plastic sheet barrier. The assistant stood either by the side of the intubator (A) or in the caudal direction (B).
Table 2. Comparison between plastic sheet and intubation box.
| Plastic Sheet | Intubation Box | |
|---|---|---|
| Size | Small | Bulky |
| Weight | Light | Heavy |
| Texture | Soft and flexible | Hard |
| Space occupied | Small enough | Sizable |
| Need to carry, position, and reposition | Portable | Need two persons to carry and position |
| Set-up time and effort (carrying) | Quick and easy | More time and effort |
| Working location (OR, ICU, ER) | No limitation | Inconvenient at some working environment |
| Combative or claustrophobia patients obese patient | No issue | Could be a serious problem |
| Body habitus (obesity) | No added effects | Could be a serious problem |
| Safety distance (face-to-mouth) between intubator and patient | Safe | Safe |
| Kinesthetic challenges | No | Yes |
| Restriction of arms and hands movement (intubator’s and assistant’s) | Not at all | Yes |
| Maneuverability and dexterity | Not an issue | Could be hindered |
| Cause damage on PPE | Not an issue | Yes |
| Visibility and glaring | Transparent and clear | Could be affected |
| Intubation difficulties: Time to intubate/attempts/total duration/need assistance/failure | Not affected | Could be worse and risky |
| Difficulty manipulating airway tools (inserting laryngoscope, tube negotiation, confirmation, removal of stylet) | Not affected | Could be worse and risk |
| Airway visualization—Cormack Lehane score | Not affected | Could be worse |
| Timing tolerance of hypoxemia and hypotension | Acceptable | Low tolerance |
| Removal if difficult airway emergency occurred | Easy | Take time |
| Interference on airway manipulation | Not a problem | Could be affected |
| Intubating tools selection | No limits | Video laryngoscope and bougie |
| Cause more contamination during retrieval of the barrier | Insignificant | Potential problem |
| Need experience and more training | Not a problem | Needed |
| Learning curve | High | Could be a problem |
| Disposable | Yes | Not always |
| Workload on removal and discard and disinfection | Minimal | Annoying and difficult |
| Accessible and available | Yes | Not always be |
| Affordable | Yes | Not always be |
| False sense of security | Mild | Strong |
| Subjective feeling of difficulty on intubation | Insignificant | Notable |
| Mental load | Minimal | Significant |
| Effectiveness of aerosol prevention | Only for droplets prevention | Questionable for aerosol prevention |
| Safety issues on the patients | Minimal | Might cause serious problems |
Any respiratory droplets and aerosols that may have been generated during intubation will settle onto the sheet or under the sheet on the patient (Figure 10), as opposed to being dispersed into the air, and there may be less risk of contamination if the sheet is carefully folded or rolled up at the end of the procedure. Additionally, there is an option to leave the sheet over the patient’s head until time of extubation, thus protecting airway managers from co-infection at the end of surgery, when the patient may cough or buck at time of emergence from anesthesia. The sheet can be removed concurrently with the endotracheal tube, and so be used to collect the dirty ETT for disposal. In fact, one of the first suggested uses for the plastic sheet was not for tracheal intubation but for minimizing droplet spray during extubation [41].
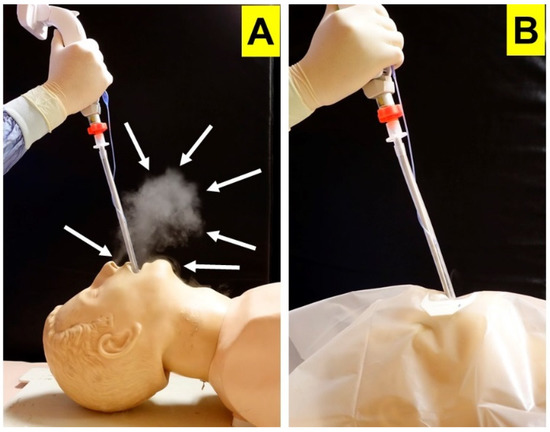
Figure 10. Mannequin demonstration of how the plastic sheet barrier prevents spread of respiratory droplets and aerosols during endotracheal intubation. (A) Endotracheal intubation using video intubating stylet without plastic sheet showing visible secretions (arrows) after a simulated cough. (B) When a plastic sheet barrier is used, secretions are contained under the sheet after a simulated cough. (Courtesy photos reproduced from Cell Transplantation [39]).
A negative aspect of simply reaching under the sheet to perform airway maneuvers is the contamination of the healthcare professional’s hands and arms during the procedure. In addition, the visualization of the indirect monitor may be difficult if the screen is mounted on the videoscope itself [42]. Subsequently, plastic sheets were modified by making openings in the plastic sheet, allowing for the airway device and ETT to be passed from above the sheet or for the provider’s hands to reach through [17][20] (Figure 9 and Figure 11). Even if the monitor was affixed to the videoscope, the operator would still have an unobstructed view if the screen remained above the barrier. In order to use a videolaryngoscope with this modified plastic sheet method, either a single large opening would be made to accommodate both laryngoscope and endotracheal tube, or two smaller openings could be made in close proximity to one another. However, the larger the opening that was created into the sheet, the larger the risk for environmental contamination, defeating the purpose of using a barrier system.

Figure 11. Modification of plastic sheet barrier with (A) small incisions marked by colored tape to (B) allow passage of intubation device from above the sheet.
The advantage of using the video intubating stylet with the plastic sheet is that because of its slim profile, only a single small opening would need to be made to allow the intubating stylet and mounted ETT to pass through (Figure 11 and Figure 12). A single institution’s protocol has been previously described in the literature, in which two small crosscuts were made into the plastic sheet with a surgical blade [38][39][40], (Figure 11). The purpose of the second incision was to have the ability to quickly perform mask ventilation or oral suctioning if the need arose during the intubation attempt (Figure 13). Both crosscuts were covered with transparent adhesive film, and a large bore needle was used to pierce a hole in the transparent film, minimizing the size of the defect while still making it easy to introduce the airway apparatus. As the video stylet passed through the hole, the transparent film would enlarge to accept the stylet but would also adhere to the endotracheal tube, minimizing the defect in the plastic sheet and the subsequent risk of environmental contamination.
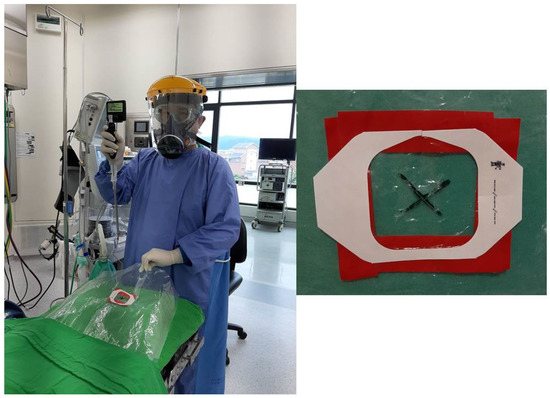
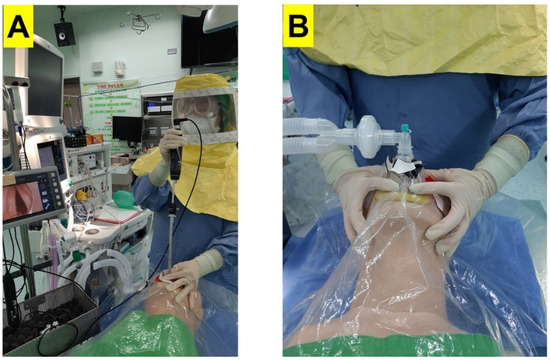
Figure 12. Only a small crosscut in the plastic sheet is needed (marked by X) to allow advancement of the video-assisted intubating stylet.
Figure 13. Two crosscuts are made into the plastic barrier sheet to allow (A) endotracheal intubation using a video-assisted intubating stylet, while (B) the second crosscut in the plastic barrier allows timely resumption of mask ventilation if the need arises during the intubation attempt. (Courtesy photo reproduced from Asian Journal of Anesthesiology [40] with permission).
Prefabricated plastic sheets have been produced with seam lines to allow easy removal of the plastic sheet after successful tracheal intubation (Figure 14), however, even without prefabricated sheets, a homemade sheet can be precut to facilitate its easy removal. While the plastic sheet is disposable as a medical waste, the intubating stylet is either disposable (costed from USD 50 to 100) or to be disinfected according to infection control policies and standard operating procedures adhered to local health regulations (for more detailed description, please see the reference [40]). As previously described, because the plastic sheet can also serve as protection against contamination during the extubation process, the sheet may be left over the patient’s head until surgery has concluded and the ETT has been removed [17][18][41].

Figure 14. Prefabricated plastic sheet with areas marked by circles to guide creation of incisions for introduction of laryngoscope/suction catheter and video stylet/endotracheal tube, as well as seam lines to allow easy removal of the plastic sheet after intubation.
5. Criticisms of Barrier Methods
A recent review of the literature screened 4509 unique articles describing barrier systems and airway management, but only 123 full-text articles met the inclusion criteria [21]. Of these papers, 42% utilized a box, while 54% used a plastic sheet, further subdivided into sheets with support (32%) and without support (22%). Unfortunately, the majority of papers written on this subject have been short letters or commentaries. To date, there is not strong evidence to support the use of barrier systems, although these systems seem to have logical benefit.
Based on what has been observed and reported in the literature, a large criticism of rigid box systems has been a delay in time to intubation, with potential worsening of airway views especially in difficult intubation situations [43][44][45]. The rigid plastic structure limits the maneuvers an airway manager might perform to optimize the glottic view (Figure 2A and Figure 8), and it might also hinder other staff from providing assistance during the intubation attempts. Other criticisms of the rigid box design have been environmental contamination at the open caudal end, as well as from secondary aerosolization at the time of box removal, difficulty with sanitation, and even harm to medical staff during its use [46]. Some studies concluded that plastic sheet systems do better than rigid box systems in terms of environmental exposure [47], operator ergonomics, and ease of allowing another provider to provide assistance [18]. Subsequently, on 20 August 2020, the FDA revoked the umbrella EUA for barrier devices and now recommends the concurrent use of negative pressure with these systems [48].
The use of the intubating stylet, although theoretically simpler and easier to use, has not been validated in humans. A few mannequin studies concluded that the intubating stylet was easier to use, had quicker intubation times with higher success rates compared to the traditional laryngoscope in simulated difficult airways [49][50], and a small randomized trial of patients being intubated in the lateral decubitus position suggested that the time to intubation using a video stylet was shorter compared to using a fiberoptic bronchoscope, although a greater hemodynamic response and higher incidence of sore throat was observed with the intubating stylet [51]. To date, there are sparse studies comparing the use of a video intubating stylet with a videolaryngoscope, which is currently commonly accepted as the preferred difficult airway device in the majority of the world [32].
Obesity is often associated with increased neck circumference, both of which are risk factors for difficult intubation [52], and obesity has been shown to be associated with a more severe COVID-19 course, including ICU admission and increased mortality [53][54]. COVID-19 patients in critical respiratory illness have poor respiratory reserves, and time to oxygen desaturation is rapid. A concern with using the intubating stylet in the obese patient is that it may be difficult to obtain a view of the glottis if there is significant soft tissue collapse after the induction of anesthesia. In extreme situations, jaw lift may not improve visualization of the airway. A laryngoscope, which has a wide blade to retract collapsed soft tissue structures and can facilitate maneuvering of the ETT towards the glottic opening, is typically used with the intubating stylet technique.
6. Future Directions and Conclusions
It is worthy to mention that videolaryngoscopy became a new paradigm for tracheal intubation (e.g., unanticipated and expected difficult airway management) since decades ago [32][55]. Such critical roles and increasing prevalence of videolaryngoscopy have been emerged in many clinical environments, such as emergency rooms, operating theaters, intensive care units, and wards [56][57][58]. Among all the intubating tools, it is interesting to note that optical (lighted and video-assisted) stylets are still not prevalent in many countries so far [59]. Such kinds of optical stylets, originally designed by Shikani [33] and later modified by Levitan [60], have been evaluated in several different clinical scenarios [61][62][63][64][65][66]. The advantages of such an airway management modality are as follows: obtaining better patient glottic view with high first-pass success rates, no need to contact any airway soft tissues and therefore causing less stimulation or tissue damages, maintaining a safe distance between the intubator from patient’s mouth, high learning curve, etc.
During COVID-19 pandemic, not surprisingly, the beneficial role of videolaryngoscopy has been repeatedly advocated in several guidelines [30][31]. Meanwhile, together with videolaryngoscopy, a gum elastic bougie (GEB, also named an endotracheal tube introducer) is an effective adjunct to difficult airway management [67][68][69][70][71]. Therefore, both essential tools have reasonably been proposed to be included in the COVID-19 emergency tracheal intubation kit dump and tray [30][31]. However, in the real world, videolaryngoscopes and video-assisted intubating stylets might not be available in some countries and regions. In that case, the airway managers should have adequate PPE while using conventional direct laryngoscope for tracheal intubation during COVID-19 pandemic.
Although the use of a video intubating stylet in conjunction with a plastic barrier sheet may be the most efficacious method to prevent environmental contamination from droplet and aerosol exposure during AGMPs, based upon the small size of the incision in the sheet that is necessary to pass the ETT, more research is needed in this area. Plastic sheets need to be shown that they do indeed mitigate the risk of environmental exposure and health care provider co-infection during tracheal intubation and extubation. Consensus on plastic sheet modifications can help reproducibility and improve efficacy across different clinical settings and hospital situations. More randomized trials with adequate patient enrollment is necessary to investigate the following scenarios: (1) the comparison of videolaryngoscopes to video stylets in difficult airway situations, especially in morbidly obese patients; (2) the effectiveness and safety of utilizing plastic sheet barriers during airway manipulation using a variety of intubating devices; and more specifically, (3) the comparison of videolaryngoscope to the video intubating stylet in conjunction with plastic sheet barrier systems.
Nonetheless, the video intubating stylet continues to gain acceptance as an indirect video intubating device in particular regions of the world given its ease of use, short training duration, relative cost, and straightforward re-sanitation process. Plastic barrier devices have shown promise to reduce environmental contamination and hospital personnel co-infection during AGMPs such as tracheal intubation. Because of its slim profile and minimal effect to disrupt the integrity of the plastic sheet, the video intubating stylet in conjunction with the plastic sheet may indeed prove to be the preferential intubating method during the COVID-19 pandemic and beyond.
]. Healthcare providers in the fields of anesthesiology, critical care medicine, emergency medicine, and otolaryngology, because of their roles in performing AGMPs for these patients, found themselves at risk of infection
References
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506.
- Data: WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 30 September 2021).
- Yuki, K.; Fujiogi, M.; Koutsogiannaki, S. COVID-19 pathophysiology: A review. Clin. Immunol. 2020, 215, 108427.
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154.
- Wax, R.S.; Christian, M.D. Practical recommendations for critical care and anesthesiology teams caring for novel coronavirus (2019-nCoV) patients. Can. J. Anaesth. 2020, 67, 568–576.
- Ruskin, K.J.; Ruskin, A.C.; Musselman, B.T.; Harvey, J.R.; Nesthus, T.E.; O’Connor, M. COVID-19, personal protective equipment, and human performance. Anesthesiology 2021, 134, 518–525.
- Verbeek, J.H.; Rajamaki, B.; Ijaz, S.; Sauni, R.; Toomey, E.; Blackwood, B.; Tikka, C.; Ruotsalainen, J.H.; Kilinc Balci, F.S. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst. Rev. 2020, 5, CD011621.
- Burki, T. Global shortage of personal protective equipment. Lancet Infect. Dis. 2020, 20, 785–786.
- Arnaout, R. Cooperation under pressure: Lessons from the COVID-19 swab crisis. J. Clin. Microbiol. 2021, 59, JCM0123921.
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976.
- Tregoning, J.S.; Flight, K.E.; Higham, S.L.; Wang, Z.; Pierce, B.F. Progress of the COVID-19 vaccine effort: Viruses, vaccines and variants versus efficacy, effectiveness and escape. Nat. Rev. Immunol. 2021, 21, 626–636.
- Everington, K. Taiwanese Doctor Invents Device to Protect US Doctors against Coronavirus. 23 March 2020. Available online: https://www.taiwannews.com.tw/en/news/3902435 (accessed on 20 August 2021).
- Lai, H.Y. Aerosol Box Protects Healthcare Providers during Endotracheal Intubation. Available online: https://sites.google.com/view/aerosolbox/home?authuser=0 (accessed on 20 August 2021).
- Canelli, R.; Connor, C.W.; Gonzalez, M.; Nozari, A.; Ortega, R. Barrier enclosure during endotracheal intubation. N. Engl. J. Med. 2020, 382, 1957–1958.
- Fidler, R.L.; Niedek, C.R.; Teng, J.J.; Sturgeon, M.E.; Zhang, Q.; Robinowitz, D.L.; Hirsch, J. Aerosol retention characteristics of barrier devices. Anesthesiology 2021, 134, 61–71.
- Fried, E.A.; Zhou, G.; Shah, R.; Shin, D.W.; Shah, A.; Katz, D.; Burnett, G.W. Barrier devices, intubation, and aerosol mitigation strategies: Personal protective equipment in the time of Coronavirus Disease 2019. Anesth. Analg. 2021, 132, 38–45.
- Babazade, R.; Khan, E.S.; Ibrahim, M.; Simon, M.; Vadhera, R.B. Additional barrier to protect health care workers during intubation. Anesth. Analg. 2020, 131, e47–e48.
- Brown, H.; Preston, D.; Bhoja, R. Thinking outside the box: A low-cost and pragmatic alternative to aerosol boxes for endotracheal intubation of COVID-19 patients. Anesthesiology 2020, 133, 683–684.
- Brown, S.; Patrao, F.; Verma, S.; Lean, A.; Flack, S.; Polaner, D. Barrier system for airway management of COVID-19 patients. Anesth. Analg. 2020, 131, e34–e35.
- Emami, N.; Tanner, T.; Ogundipe, F.; Hawn, V.S.; Rubin, R.; Skae, C.C.; Shiloh, A.L.; Keene, A.B. Drape to prevent disease transmission during endotracheal intubation. Am. J. Infect. Control 2021, 49, 387–388.
- Price, C.; Ben-Yakov, M.; Choi, J.; Orchanian-Cheff, A.; Tawadrous, D. Barrier enclosure use during aerosol-generating medical procedures: A scoping review. Am. J. Emerg. Med. 2021, 41, 209–218.
- U.S. Food & Drug Administration. Emergency Use Authorization for Protective Barrier Enclosures in Response to the Evolving Coronavirus Disease 2019 (COVID-19) Pandemic. 1 May 2020. Available online: https://www.fda.gov/media/141415/download (accessed on 19 August 2020).
- Rosenblatt, W.H.; Sherman, J.D. More on barrier enclosure during endotracheal intubation. N. Engl. J. Med. 2020, 382, e69.
- Kovatsis, P.G.; Matava, C.T.; Payton, J.M. More on barrier enclosure during endotracheal intubation. N. Engl. J. Med. 2020, 382, e69.
- Duggan, L.V.; Marshall, S.D.; Scott, J.; Brindley, P.G.; Grocott, H.P. The MacGyver bias and attraction of homemade devices in healthcare. Can. J. Anaesth. 2019, 66, 757–761.
- Brewster, D.J.; Begley, J.L.; Marshall, S.D. Rise and fall of the aerosol box; and what we must learn from the adoption of untested equipment. Emerg. Med. J. 2021, 38, 109–110.
- Turner, M.C.; Duggan, L.V.; Glezerson, B.A.; Marshall, S.D. Thinking outside the (acrylic) box: A framework for the local use of custom-made medical devices. Anaesthesia 2020, 75, 1566–1569.
- Berry, J.M. Conventional (laryngoscopic) orotracheal and nasotracheal intubation (single lumen tube). In Benumof’s Airway Management: Principles and Practice, 2nd ed.; Benumof, J.L., Ed.; Mosby-Elsevier: Philadelphia, PA, USA, 2007; Chapter 16; pp. 379–392.
- Kabrhel, C.; Thomsen, T.W.; Setnik, G.S.; Walls, R.M. Videos in clinical medicine. Orotracheal intubation. N. Engl. J. Med. 2007, 356, e15.
- Cook, T.M.; El-Boghdadly, K.; McGuire, B.; McNarry, A.F.; Patel, A.; Higgs, A. Consensus guidelines for managing the airway in patients with COVID-19: Guidelines from the Difficult Airway Society, the Association of Anaesthetists, the Intensive Care Society, the Faculty of Intensive Care Medicine and the Royal College of Anaesthetists. Anaesthesia 2020, 75, 785–799.
- Brewster, D.J.; Chrimes, N.; Do, T.B.; Fraser, K.; Groombridge, C.J.; Higgs, A.; Humar, M.J.; Leeuwenburg, T.J.; McGloughlin, S.; Newman, F.G.; et al. Consensus statement: Safe Airway Society principles of airway management and tracheal intubation specific to the COVID-19 adult patient group. Med. J. Aust. 2020, 212, 472–481.
- Lewis, S.R.; Butler, A.R.; Parker, J.; Cook, T.M.; Smith, A.F. Videolaryngoscopy versus direct laryngoscopy for adult patients requiring tracheal intubation. Cochrane Database Syst. Rev. 2016, 11, CD011136.
- Shikani, A.H. New “seeing” stylet-scope and method for the management of the difficult airway. Otolaryngol. Head Neck Surg. 1999, 120, 113–116.
- Lee, M.C.; Tseng, K.Y.; Shen, Y.C. Nasotracheal intubation in patients with limited mouth opening: A comparison between fibreoptic intubation and the Trachway®. Anaesthesia 2016, 71, 31–38.
- Yang, M.; Kim, J.A.; Ahn, H.J.; Choi, J.W.; Kim, D.K.; Cho, E.A. Double-lumen tube tracheal intubation using a rigid video-stylet: A randomized controlled comparison with the Macintosh laryngoscope. Br. J. Anaesth. 2013, 111, 990–995.
- Yoon, H.K.; Lee, H.C.; Park, J.B.; Oh, H.; Hee-Pyoung Park, H.P. McGrath MAC videolaryngoscope versus Optiscope video stylet for tracheal intubation in patients with manual inline cervical stabilization: A randomized trial. Anesth. Analg. 2020, 130, 870–878.
- Kim, J.K.; Kim, J.A.; Kim, C.S.; Ahn, H.J.; Yang, M.K.; Choi, S.J. Comparison of tracheal intubation with the Airway Scope or Clarus Video System in patients with cervical collars. Anaesthesia 2011, 66, 694–698.
- Yang, Y.L.; Huang, C.H.; Luk, H.N.; Tsai, P.B. Adaptation to the plastic barrier sheet to facilitate intubation during the COVID-19 pandemic. Anesth. Analg. 2020, 131, e97–e99.
- Luk, H.N.; Yang, Y.L.; Tsai, P.B. Application of plastic sheet barrier and video intubating stylet to protect tracheal intubators during coronavirus disease 2019 pandemic: A Taiwan experience. Cell Transplant. 2021, 30.
- Tsai, P.B.; Luk, H.N. Plastic sheet and video intubating stylet: A technical note. Asian J. Anesthesiol. 2021, 1–5.
- Matava, C.T.; Yu, J.; Denning, S. Clear plastic drapes may be effective at limiting aerosolization and droplet spray during extubation: Implications for COVID-19. Can J Anaesth. 2020, 67, 902–904.
- Rose, P.; Veall, J.; Chima, N.; Vowels, E.; Chitnis, S.; Flexman, A.; Tang, R. A comparison of droplet and contact contamination using 3 simulated barrier techniques for COVID-19 intubation: A quality assurance study. CMAJ Open 2020, 8, E554–E559.
- Begley, J.L.; Lavery, K.E.; Nickson, C.P.; Brewster, D.J. The aerosol box for intubation in coronavirus disease 2019 patients: An in-situ simulation crossover study. Anaesthesia 2020, 75, 1014–1021.
- Jen, T.T.H.; Gusti, V.; Badh, C.; Mehta, S.; Denomme, J.; Lockhart, S.; Shams, B.; Klaibert, B.; Chau, A. The impact of a barrier enclosure on time to tracheal intubation: A randomized controlled trial. Can. J. Anaesth. 2021, 68, 1358–1367.
- Lim, Z.J.; Ponnapa Reddy, M.; Karalapillai, D.; Shekar, K.; Subramaniam, A. Impact of an aerosol box on time to tracheal intubation: Systematic review and meta-analysis. Br. J. Anaesth. 2021, 126, e122–e125.
- Sorbello, M.; Rosenblatt, W.; Hofmeyr, R.; Greif, R.; Urdaneta, F. Aerosol boxes and barrier enclosures for airway management in COVID-19 patients: A scoping review and narrative synthesis. Br. J. Anaesth. 2020, 125, 880–894.
- Simpson, J.P.; Wong, D.N.; Verco, L.; Carter, R.; Dzidowski, M.; Chan, P.Y. Measurement of airborne particle exposure during simulated tracheal intubation using various proposed aerosol containment devices during the COVID-19 pandemic. Anaesthesia 2020, 75, 1587–1595.
- U.S. Food & Drug Administration. Protective Barrier Enclosures without Negative Pressure Used during the COVID-19 Pandemic May Increase Risk to Patients and Health Care Providers—Letter to Health Care Providers. 20 August 2020. Available online: https://www.fda.gov/medical-devices/letters-health-care-providers/protective-barrier-enclosures-without-negative-pressure-used-during-covid-19-pandemic-may-increase (accessed on 20 August 2021).
- Ong, J.; Lee, C.L.; Huang, S.J.; Shyr, M.H. Comparison between the Trachway video intubating stylet and Macintosh laryngoscope in four simulated difficult tracheal intubations: A manikin study. Tzu Chi Med. J. 2016, 28, 109–112.
- Wu, M.Y.; Yiang, G.T.; Ke, J.Y.; Chen, C.S.; Lin, P.C.; Chen, Y.L. Role of Trachway versus conventional modes of intubation in difficult airway management in COVID-19 setups. Emerg. Med. Int. 2021, 25, 6614523.
- Wahdan, A.S.; El-Refai, N.A.R.; Omar, S.H.; Abdel Moneem, S.A.; Mohamed, M.M.; Hussien, M.M. Endotracheal intubation in patients undergoing open abdominal surgery in the lateral position: A comparison between the intubating video stylet and fiberoptic intubating bronchoscopy. Korean J. Anesthesiol. 2021, 74, 234–241.
- Lundstrøm, L.H.; Møller, A.M.; Rosenstock, C.; Astrup, G.; Wetterslev, J. High body mass index is a weak predictor for difficult and failed tracheal intubation: A cohort study of 91,332 consecutive patients scheduled for direct laryngoscopy registered in the Danish Anesthesia Database. Anesthesiology 2009, 110, 266–274.
- Popkin, B.M.; Du, S.; Green, W.D.; Beck, M.A.; Algaith, T.; Herbst, C.H.; Alsukait, R.F.; Alluhidan, M.; Alazemi, N.; Shekar, M. Individuals with obesity and COVID-19: A global perspective on the epidemiology and biological relationships. Obes. Rev. 2020, 21, e13128.
- Drucker, D.J. Diabetes, obesity, metabolism, and SARS-CoV-2 infection: The end of the beginning. Cell Metab. 2021, 33, 479–498.
- Cook, T.M.; Kelly, F.E. A national survey of videolaryngoscopy in the United Kingdom. Br. J. Anaesth. 2017, 118, 593–600.
- Swaminathan, A.K.; Rachel Berkowitz, R.; Baker, A.; Spyres, M. Do emergency medicine residents receive appropriate video laryngoscopy training? A survey to compare the utilization of video laryngoscopy devices in emergency medicine residency programs and community emergency departments. J. Emerg. Med. 2015, 48, 613–619.
- Monette, D.L.; Brown III, C.A.; Benoit, J.L.; McMullan, J.T.; Carleton, S.C.; Steuerwald, M.T.; Eyre, A.; Pallin, D.J.; NEAR III Investigators. The impact of video laryngoscopy on the clinical learning environment of emergency medicine residents: A report of 14,313 intubations. AEM. Educ. Train. 2019, 3, 156–162.
- Ono, Y.; Tanigawa, K.; Shinohara, K.; Yano, T.; Sorimachi, K.; Inokuchi, R.; Shimada, J. Human and equipment resources for difficult airway management, airway education programs, and capnometry use in Japanese emergency departments: A nationwide cross-sectional study. Int. J. Emerg. Med. 2017, 10, 28.
- Liu, H.H.; Wang, Y.; Zhong, M.; Li, Y.H.; Gao, H.; Zhang, J.F.; Ma, W.H. Managing the difficult airway: A survey of doctors with different seniority in China. Medicine 2021, 100, e27181.
- Levitan, R.M. Design rationale and intended use of a short optical stylet for routine fiberoptic augmentation of emergency laryngoscopy. Am. J. Emerg. Med. 2006, 24, 490–495.
- Biro, P.; Bättig, U.; Henderson, J.; Seifert, B. First clinical experience of tracheal intubation with the SensaScope, a novel steerable semirigid video stylet. Br. J. Anaesth. 2006, 97, 255–261.
- Phua, D.S.; Mah, C.L.; Wang, C.F. The Shikani optical stylet as an alternative to the GlideScope® videolaryngoscope in simulated difficult intubations—A randomised controlled trial. Anaesthesia 2012, 67, 402–406.
- Cooney, D.R.; Cooney, N.L.; Wallus, H.; Wojcik, S. Performance of emergency physicians utilizing a video-assisted semi-rigid fiberoptic stylet for intubation of a difficult airway in a high-fidelity simulated patient: A pilot study. Int. J. Emerg. Med. 2012, 5, 24.
- Kok, T.; George, R.B.; McKeen, D.; Vakharia, N.; Pink, A. Effectiveness and safety of the Levitan FPS Scope™ for tracheal intubation under general anesthesia with a simulated difficult airway. Can. J. Anaesth. 2012, 59, 743–750.
- Gaszynski, T.; Pietrzyk, M.; Szewczyk, T.; Gaszynska, E. A comparison of performance of endotracheal intubation using the Levitan FPS optical stylet or Lary-Flex videolaryngoscope in morbidly obese patients. Sci. World J. 2014, 207591.
- Xu, M.; Li, X.X.; Guo, X.Y.; Wang, J. Shikani optical stylet versus Macintosh laryngoscope for intubation in patients undergoing surgery for cervical spondylosis: A randomized controlled trial. Chin. Med. J. 2017, 130, 297–302.
- Evans, A.; Morris, S.; Petterson, J.; Hall, J.E. A comparison of the Seeing Optical Stylet and the gum elastic bougie in simulated difficult tracheal intubation: A manikin study. Anaesthesia 2006, 61, 478–481.
- Driver, B.; Dodd, K.; Klein, L.R.; Buckley, R.; Robinson, A.; McGill, J.W.; Reardon, R.F.; Prekker, M.E. The bougie and first-pass success in the emergency department. Ann. Emerg. Med. 2017, 70, 473–478.
- Ono, Y.; Shinohara, K.; Shimada, J.; Inoue, S.; Kotani, J. Lower maximum forces on oral structures when using gum-elastic bougie than when using endotracheal tube and stylet during both direct and indirect laryngoscopy by novices: A crossover study using a high-fidelity simulator. BMC Emerg. Med. 2020, 20, 34.
- Driver, B.E.; Prekker, M.E.; Klein, L.R.; Reardon, R.F.; Miner, J.R.; Fagerstrom, E.T.; Cleghorn, M.R.; McGill, J.W.; Cole, J.B. Effect of use of a bougie vs endotracheal tube and stylet on first-attempt intubation success among patients with difficult airways undergoing emergency intubation: A randomized clinical trial. JAMA 2018, 319, 2179–2189.
- Combes, X.; Jabre, P.; Margenet, A.; Merle, J.C.; Leroux, B.; Dru, M.; Lecarpentier, E.; Dhonneur, G. Unanticipated difficult airway management in the prehospital emergency setting: Prospective validation of an algorithm. Anesthesiology 2011, 114, 105–110.
More