Painful Legs and Moving Toes syndrome (PLMT) is a rare neurological movement disorder characterized by involuntary and irregular movements of one or more toes, often together, with moderate to severe diffuse pain at the foot and leg. It can appear on one or both sides and in the upper limbs as well as lower limbs. The etiology of PLMT is still unclear; therefore, the main symptoms of PLMT, including pain in limbs as well as involuntary movements of toes, can be treated only symptomatically, and the outcomes are often unsatisfactory. Central or peripheral nerve injuries have been assumed to be the possible causes of irregular involuntary movements, often accompanied by chronic pain; however, its etiology is unknown in most cases. The management of PLMT is very difficult because of its rare prevalence and obscure pathogenesis, and there have been no clear guidelines for the treatment of PLMT. Oral medications (e.g., GABAergic agents, benzodiazepines, antiepileptics, antidepressants, atypical antipsychotics, beta-blockers, corticosteroids, cannabis, calcitonin, and analgesics) and several therapeutic interventions (e.g., local botulinum neurotoxin-A injection, spinal cord stimulation, anesthetic, and surgical interventions) have been recommended, based on individual experiences from several cases. Its etiology, pathogenesis, and effective treatments should be further discussed.
- painful legs
- moving toes
- PLMT
- pain
- movement disorder
- involuntary
- botulinum
- pregabalin
- spinal stimulation
1. History
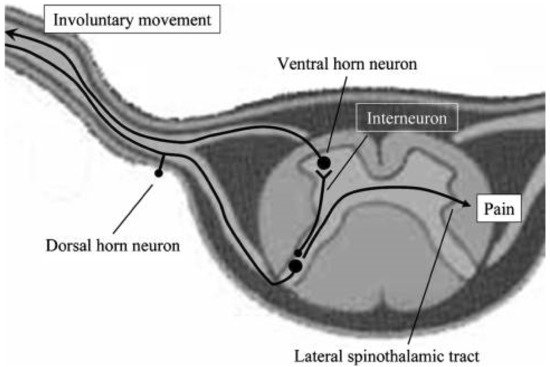
Painful Legs and Moving Toes syndrome (PLMT), one of the spinal-generated movement disorders
, is a rare movement disorder with involuntary irregular flexion/extension of one or more toes, which is often accompanied with pain felt deeply in the foot and leg. It therefore reduces the quality of life as well as activities in social community and the workplace
. PLMT was firstly reported as a pain syndrome in the feet or lower limbs with spontaneous movements of the toes by Spillane and colleagues in 1971
; since then, PLMT has been described in case or cases series reports rarely
. Until now, about 130 cases with PLMT have been reported, according to our literature search on PubMed and other public open-access databases (screening on 31 October 2021) and patients’ ages ranged from 11 to 86
. The definition of PLMT has expanded to the upper limbs (painful hands and moving fingers)
. It has been also called “painful limbs and moving extremities” involving more than toes or fingers, e.g., feet or hands and limbs
. The affected locations have extended from toes or fingers proximally to ipsilateral foot or hands and limbs, as well as contralateral limbs in some cases, and possibly from the lower limb to the upper
. Several atypical cases with painful movement disorder have been reported
. One case with PLMT extended to the tongue, called “painful moving tongue”, but detailed information was not available
2. Etiology of PLMT
Radiculopathy
Plexus injury
Focal neuropathy (e.g., tarsal tunnel syndrome)
Polyneuropathy (large fiber, small fiber)
Herpes zoster myelitis
Spinal cord compression
Traumatic spinal cord injury
Postsurgical complication
Hashimoto’s Encephalopathy
Morbus Wilson
Morbus Parkinson
Stroke
Neuroleptics
Endocrinologic condition, e.g., Hashimoto thyroiditis and Hypophysenadenome
Local trauma without neurologic injury (at least not found)
Dupuytren’s contracture
3. Diagnostics of PLMT
3.1. Medical History of Possible Pathological Conditions of PLMT
3.2. Clinical and Neurophysiological Diagnostics
3.3. Neurophysiological Examination
- -
-
the first type with short duration (10–80 ms) and a higher frequency of 4–6 Hz
- -
-
the second type with longer duration (160–500 ms) and lower frequency of 1.5–3 Hz.
3.4. Differential Diagnoses
- -
-
Restless leg syndrome with pain and movement of feet and legs;
- -
-
Painful radiculopathy or plexopathy;
- -
-
Complex regional pain syndrome;
- -
-
Akathisia with leg movements;
- -
-
Cramps with unilateral involuntary muscle hardening, usually calf muscle;
- -
-
Spinal segmental myoclonus with leg movement;
- -
-
EPC with continuous toes/foot or leg movement;
- -
-
Focal or polyneuropathy with feet numbness, tingling, and/or pain;
- -
-
Dystonia with sustained involuntary movements of feet and legs;
- -
-
Periodic-limb-movement disorder (PLMD);
- -
-
Parkinson with tremor;
- -
-
Chorea;
- -
-
Pseudoathetosis;
- -
-
Epilepsia partialis continua with toes/foot movements; and
- -
-
Psychogenic movement disorder.
4. Management of PLMT
Spinal cord stimulation
Botulinum neurotoxin injection
Local vibration
Sympathetic blockade
Epidural blockade
Transcutaneous electrical nerve stimulation
Massage
Local cold, warm, or tactile stimulation
Sympathectomy
Surgical decompression
Other surgical treatments according to possible causes of PLMT
4.1. Pharmacological Therapy
4.1.1. Oral Medication
4.1.2. Interventions
4.2. Nonpharmacological Therapeutic Interventions
4.3. Other Surgical Treatments
5. Conclusions and Prospects
.
References
- Termsarasab, P.; Thammongkolchai, T.; Frucht, S.J. Spinal-generated movement disorders: A clinical review. J. Clin. Mov. Disord. 2015, 2, 18.
- Spillane, J.D.; Nathan, P.W.; Kelly, R.E.; Marsden, C.D. Painful legs and moving toes. Brain 1971, 94, 541–556.
- Rossi, F.H.; Liu, W.; Geigel, E.; Castaneda, S.; Rossi, E.M.; Schnacky, K. Painful legs and moving toes syndrome responsive to pregabalin. J. Postgrad. Med. 2015, 61, 116–119.
- Okamoto, S.; Takegami, T.; Mano, T. Peculiar involuntary movement of the toes associated with discomfort of the foot, a case of so-called “painful legs and moving toes”. Rinsho Shinkeigaku 1974, 14, 829–834. (In Japanese)
- Nathan, P.W. Painful legs and moving toes: Evidence on the site of the lesion. J. Neurol. Neurosurg. Psychiatry 1978, 41, 934–939.
- Schott, G.D. Painful legs and moving toes: The role of trauma. J. Neurol. Neurosurg. Psychiatry 1981, 44, 344–346.
- Verhagen, W.I.; Horstink, M.W.; Notermans, S.L. Painful arm and moving fingers. J. Neurol. Neurosurg. Psychiatry 1985, 48, 384–385.
- Funakawa, I.; Mano, Y.; Takayanagi, T. Painful hand and moving fingers. A case report. J. Neurol. 1987, 234, 342–343.
- Walters, A.S.; Hening, W.A.; Shah, S.K.; Chokroverty, S. Painless legs and moving toes: A syndrome related to painful legs and moving toes? Mov. Disord. 1993, 8, 377–379.
- Dressler, D.; Thompson, P.D.; Gledhill, R.F.; Marsden, C.D. The syndrome of painful legs and moving toes. Mov. Disord. 1994, 9, 13–21.
- Supiot, F.; Gazagnes, M.D.; Blecic, S.A.; Zegers de Beyl, D. Painful arm and moving fingers: Clinical features of four new cases. Mov. Disord. 2002, 17, 616–618.
- Papapetropoulos, S.; Singer, C. Painless legs moving toes in a patient with Wilson’s disease. Mov. Disord. 2006, 21, 579–580.
- Hassan, A.; Mateen, F.J.; Coon, E.A.; Ahlskog, J.E. Painful legs and moving toes syndrome: A 76-patient case series. Arch. Neurol. 2012, 69, 1032–1038.
- Fan, Y.Y.; Xu, Y.; Gao, X.G. Spontaneous aching pain and peculiar involuntary movements: A case report of painful legs and moving toes and review of the literature. Case Rep. Med. 2014, 2014, 581402.
- Reich, S.G. Painful legs and moving toes. Handb. Clin. Neurol. 2011, 100, 375–383.
- Ebersbach, G.; Schelosky, L.; Schenkel, A.; Scholz, U.; Poewe, W. Unilateral painful legs and moving toes syndrome with moving fingers--evidence for distinct oscillators. Mov. Disord. 1998, 13, 965–968.
- Mosek, A.; Rabey, J.M.; Kushnir, M.; Korczyn, A.D. Painful calf, moving foot. Mov. Disord. 1996, 11, 339–340.
- Dziewas, R.; Kuhlenbäumer, G.; Okegwo, A.; Lüdemann, P. Painless legs and moving toes in a mother and her daughter. Mov. Disord. 2003, 18, 718–722.
- Singer, C.; Papapetropoulos, S. A case of painless arms/moving fingers responsive to botulinum toxin a injections. Parkinsonism Relat. Disord. 2007, 13, 55–56.
- Alrawashdeh, O. Painless legs and moving toes syndrome associated with a sacral Tarlov cyst: A case report. J. Med. Case Rep. 2016, 10, 52.
- Bermejo, P.E.; Zabala, J.A. Painless legs and moving toes” syndrome due to spinal cord compression. Eur. Spine J. 2008, 17 (Suppl. S2), S294–S295.
- Schwingenschuh, P.; Bhatia, K.P. Painful moving tongue in a patient with the painful legs moving toes syndrome. Mov. Disord. 2008, 23, 1324–1325.
- Guimarães, J.; Santos, L.; Bugalho, P. Painful legs and moving toes syndrome associated with Hashimoto’s disease. Eur. J. Neurol. 2007, 14, 343–345.
- Renard, D.; Taieb, G.; Castelnovo, G.; Labauge, P. Teaching Video NeuroImages: Painful legs, moving toes associated with partial transverse myelitis. Neurology 2010, 75, e74.
- Ikeda, K.; Deguchi, K.; Touge, T.; Sasaki, I.; Tsukaguchi, M.; Shimamura, M.; Komatsu, E.; Takeuchi, H.; Kuriyama, S. Painful legs and moving toes syndrome associated with herpes zoster myelitis. J. Neurol. Sci. 2004, 219, 147–150.
- Guieu, R.; Sampiéri, F.; Pouget, J.; Guy, B.; Rochat, H. Adenosine in painful legs and moving toes syndrome. Clin. Neuropharmacol. 1994, 17, 460–469.
- Zinnuroglu, M.; Ozkayran, T. Painful legs and moving toes following a traumatic medial plantar nerve injury. Mov. Disord. 2010, 25, 133–135.
- Mitsumoto, H.; Levin, K.H.; Wilbourn, A.J.; Chou, S.M. Hypertrophic mononeuritis clinically presenting with painful legs and moving toes. Muscle Nerve 1990, 13, 215–221.
- Pla, M.E.; Dillingham, T.R.; Spellman, N.T.; Colon, E.; Jabbari, B. Painful legs and moving toes associates with tarsal tunnel syndrome and accessory soleus muscle. Mov. Disord. 1996, 11, 82–86.
- Montagna, P.; Cirignotta, F.; Sacquegna, T.; Martinelli, P.; Ambrosetto, G.; Lugaresi, E. “Painful legs and moving toes” associated with polyneuropathy. J. Neurol. Neurosurg. Psychiatry 1983, 46, 399–403.
- Touge, T.; Ishibashi, T.; Kamoda, M.; Tsukaguchi, M.; Takeuchi, H. Painful legs and moving toes” and muscle cramps spreading to the bilateral legs in a patient with alcoholic polyneuropathy. Rinsho Shinkeigaku 1998, 38, 762–766. (In Japanese)
- Pitágoras de Mattos, J.; Oliveira, M.; André, C. Painful legs and moving toes associated with neuropathy in HIV-infected patients. Mov. Disord. 1999, 14, 1053–1054.
- Di Fabio, R.; Casali, C.; Pierelli, F. Quetiapine: An alternative treatment in painless legs and moving toes. Mov. Disord. 2008, 23, 1326–1328.
- Pandey, S.; Soni, G. Painful leg and moving toes syndrome in secondary tethered cord syndrome. J. Spinal Cord Med. 2016, 39, 363–365.
- Kwon, S.J.; Kim, J.M.; Jeon, B.S. A case report of painless moving toes syndrome. J. Clin. Neurol. 2008, 4, 33–35.
- Wulff, C.H. Painful legs and moving toes. A report of 3 cases with neurophysiological studies. Acta Neurol. Scand. 1982, 66, 283–287.
- El Otmani, H.; Moutaouakil, F.; Fadel, H.; Slassi, I. Syndrome de jambe douloureuse et orteils instables associé à une radiculopathie lombaire . Rev. Neurol. 2009, 165, 980–983.
- Sahashi, K.; Tsuchiya, I.; Iwase, S.; Ibi, T.; Mano, T. Clinical analyses on moving toes in “painful legs and moving toes”. Rinsho Shinkeigaku 1989, 29, 849–853. (In Japanese)
- Okuda, Y.; Suzuki, K.; Kitajima, T.; Masuda, R.; Asai, T. Lumbar epidural block for ‘painful legs and moving toes’ syndrome: A report of three cases. Pain 1998, 78, 145–147.
- Miyakawa, T.; Yoshimoto, M.; Takebayashi, T.; Yamashita, T. Case reports: Painful limbs/moving extremities: Report of two cases. Clin. Orthop. Relat. Res. 2010, 468, 3419–3425.
- Uchihara, T.; Ichikawa, T.; Furukawa, T.; Tsukagoshi, H. Myoclonus with burning sensation in legs that remits with sympathetic blockade. J. Neurol. Sci. 1990, 100, 161–164.
- Seipelt, M.; Zerr, I.; Nau, R.; Mollenhauer, B.; Kropp, S.; Steinhoff, B.J.; Wilhelm-Gössling, C.; Bamberg, C.; Janzen, R.W.; Berlit, P.; et al. Hashimoto’s encephalitis as a differential diagnosis of Creutzfeldt-Jakob disease. J. Neurol. Neurosurg. Psychiatry 1999, 66, 172–176.
- Takahashi, H.; Saitoh, C.; Iwata, O.; Nanbu, T.; Takada, S.; Morita, S. Epidural spinal cord stimulation for the treatment of painful legs and moving toes syndrome. Pain 2002, 96, 343–345.
- Shime, N.; Sugimoto, E. Lumbar sympathetic ganglion block in a patient with painful legs and moving toes syndrome. Anesth. Analg. 1998, 86, 1056–1057.
- Drummond, P.D.; Finch, P.M. Sympathetic nervous system involvement in the syndrome of painful legs and moving toes. Clin. J. Pain 2004, 20, 370–374.
- Tanaka, M.; Török, N.; Tóth, F.; Szabó, Á.; Vécsei, L. Co-Players in Chronic Pain: Neuroinflammation and the Tryptophan-Kynurenine Metabolic Pathway. Biomedicines 2021, 9, 897.
- Guieu, R.; Tardy-Gervet, M.F.; Blin, O.; Pouget, J. Pain relief achieved by transcutaneous electrical nerve stimulation and/or vibratory stimulation in a case of painful legs and moving toes. Pain 1990, 42, 43–48.
- Alvarez, M.V.; Driver-Dunckley, E.E.; Caviness, J.N.; Adler, C.H.; Evidente, V.G. Case series of painful legs and moving toes: Clinical and electrophysiologic observations. Mov. Disord. 2008, 23, 2062–2066.
- Nishioka, K.; Suzuki, M.; Nakajima, M.; Hara, T.; Iseki, M.; Hattori, N. Painful legs and moving toes syndrome evaluated through brain single photon emission computed tomography: A case series. J. Neurol. 2019, 266, 717–725.
- Diaz, N.L.; Hanspal, E.K.; Mazzoni, P. Painless legs and moving toes: Symptom reduction during pregnancy. Mov. Disord. 2012, 27, 328–329.
- Thiriez, C.; Gurruchaga, J.M.; Goujon, C.; Fénelon, G.; Palfi, S. Spinal stimulation for movement disorders. Neurotherapeutics 2014, 11, 543–552.
- Sanders, P.; Waddy, H.M.; Thompson, P.D. An ‘annoying’ foot: Unilateral painful legs and moving toes syndrome. Pain 1999, 82, 103–104.
- Schoenen, J.; Gonce, M.; Delwaide, P.J. Painful legs and moving toes: A syndrome with different physiopathologic mechanisms. Neurology 1984, 34, 1108–1112.
- Lugaresi, E.; Cirignotta, F.; Coccagna, G.; Montagna, P. Nocturnal myoclonus and restless legs syndrome. Adv. Neurol. 1986, 43, 295–307.
- Jankovic, J.; Pardo, R. Segmental myoclonus. Clinical and pharmacologic study. Arch. Neurol. 1986, 43, 1025–1031.
- Liu, R.; Moizuddin, M.; Hung, S. Painful legs and moving toes: Case report and review of literature. Br. J. Med. Pract. 2011, 4, a431.
- Tan, A.K.; Tan, C.B. The syndrome of painful legs and moving toes—A case report. Singap. Med. J. 1996, 37, 446–447.
- Gastaut, J.L. Jambes douloureuses et orteils instables. Un cas d’origine médicamenteuse . Rev. Neurol. 1986, 142, 641–642. (In French)
- Malapert, D.; Degos, J.D. Jambes douloureuses et orteils instables. Neuropathie induite par la cytarabine . Rev. Neurol. 1989, 145, 869–871. (In French)
- Schwartzman, R.J.; Kerrigan, J. The movement disorder of reflex sympathetic dystrophy. Neurology 1990, 40, 57–61.
- Bhatia, K.P.; Bhatt, M.H.; Marsden, C.D. The causalgia-dystonia syndrome. Brain 1993, 116, 843–851.
- Sandyk, R. Neuroleptic-induced “painful legs and moving toes” syndrome: Successful treatment with clonazepam and baclofen. Ital. J. Neurol. Sci. 1990, 11, 573–576.
- Villarejo, A.; Porta-Etessam, J.; Camacho, A.; De La Aleja, J.G.; Martínez-Salio, A.; Penas, M. Gabapentin for painful legs and moving toes syndrome. Eur. Neurol. 2004, 51, 180–181.
- Aizawa, H. Gabapentin for painful legs and moving toes syndrome. Intern. Med. 2007, 46, 1937.
- Bhargava, P.; Pandav, V.; Peche, S. A pediatric case of painful legs and moving toes syndrome. Pediatr. Neurol. 2013, 49, 298–299.
- Eisa, M.; Singer, C.; Sengun, C.; Russel, A.; Jabbari, B.; Papapetropoulos, S. Treatment of painful limbs/moving extremities with botulinum toxin type A injections. Eur. Neurol. 2008, 60, 104–106.
- Peña, E.; Llanero, M. Painful legs and moving toes syndrome associated with a sacral Tarlov cyst. Parkinsonism Relat. Disord. 2011, 17, 645–646.
- Bovier, P.; Hilleret, H.; Tissot, R. Traitement par le progabide d’un cas de syndrome des jambes douloureuses et orteils instables . Rev. Neurol. 1985, 141, 422–424. (In French)
- Azzi, J.; Atweh, S.; Saade, N.; Jabbour, R. Neuroleptics as a cause of painful legs and moving toes syndrome. BMJ Case Rep. 2014, 2014, bcr2014205117.
- Gordon, M.F.; Diaz-Olivo, R.; Hunt, A.L.; Fahn, S. Therapeutic trial of milacemide in patients with myoclonus and other intractable movement disorders. Mov. Disord. 1993, 8, 484–488.
- Ri, S.; Kivi, A.; Wissel, J. The Safety and Effect of Local Botulinumtoxin a Injections for Long-Term Management of Chronic Pain in Post-Herpetic Neuralgia: Literature Review and Cases Report Treated with Incobotulinumtoxin A. J. Pers. Med. 2021, 11, 758.
- Durham, P.L.; Cady, R.; Cady, R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: Implications for migraine therapy. Headache 2004, 44, 35–42.
- Lucioni, A.; Bales, G.T.; Lotan, T.L.; McGehee, D.S.; Cook, S.P.; Rapp, D.E. Botulinum toxin type A inhibits sensory neuropeptide release in rat bladder models of acute injury and chronic inflammation. BJU Int. 2008, 101, 366–370.
- McMahon, H.T.; Foran, P.; Dolly, J.O.; Verhage, M.; Wiegant, V.M.; Nicholls, D.G. Tetanus toxin and botulinum toxins type A and B inhibit glutamate, gamma-aminobutyric acid, aspartate, and met-enkephalin release from synaptosomes. Clues to the locus of action. J. Biol. Chem. 1992, 267, 21338–21343.
- Wissel, J.; Ri, S. Assessment, goal setting, and botulinum neurotoxin a therapy in the management of post-stroke spastic movement disorder: Updated perspectives on best practice. Expert Rev. Neurother. 2021, 30, 1–16.
- Rodriguez, R.L.; Fernandez, H.H. Sustained benefit of painful legs moving toes syndrome with botulinum toxin type A. J. Clin. Neurosci. 2013, 20, 1031–1032.
- Argyriou, A.A.; Papapetropoulos, S. Botulinum toxin type A for painful limbs moving extremities. Mov. Disord. 2010, 25, 125.
- Schoffer, K. Painful leg moving toes treated with botulinum toxin type A: A video report. Mov. Disord. 2010, 25, 784–785.
- Kivi, A.; Ri, S.; Wissel, J. What clinicians and patients want: The past, the presence, and the future of the botulinum toxins. Toxicon 2020, 177, 46–51.
- Raina, G.B.; Piedimonte, F.; Micheli, F. Posterior spinal cord stimulation in a case of painful legs and moving toes. Stereotact Funct. Neurosurg. 2007, 85, 307–309.
- Wider, C.; Kuntzer, T.; Olivier, P.; Debatisse, D.; Nancoz, R.; Maeder, P.; Bogousslavsky, J.; Vingerhoets, F. Painful hand and moving finger treated by wearing a glove. Neurology 2006, 67, 491–493.