Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Catherine Yang and Version 1 by Joaquim Soares do Brito.
The clinical course of patients with bone metastases is often impaired by bone complications, such as bone fractures, which have a substantial negative impact on clinical outcomes. The skeleton is a common site of metastatic disease in patients with advanced solid tumors, particularly breast, prostate, renal, thyroid and lung tumors. Medical advances over the last decades have been responsible for a progressive and remarkable increase in the survival of patients with cancer, and thus in the number of patients living with bone metastases (BM).
- bone metastasis
- pathologic fracture
- tailored approach
1. Breast Cancer Metastases
Breast cancer is among the carcinomas most frequently presenting BM. Breast BM typically exhibit lytic or mixed lesions [102][1]. For patients with solitary or oligometastatic disease (an unusual presentation), the treatment goal should be wide resection of metastases to enable long-term survival without evidence of disease [103,104][2][3]. Most often, however, patients with breast cancer BM present with multimetastatic disease. In this setting, non-invasive treatments, such as RT and BTAs without surgery, are plausible options, even with impending fractures (Figure 21) and when surgical treatment is particularly difficult. Nonetheless, this approach is always more straightforward for lesions presenting in the upper limbs compared with the lower limbs.
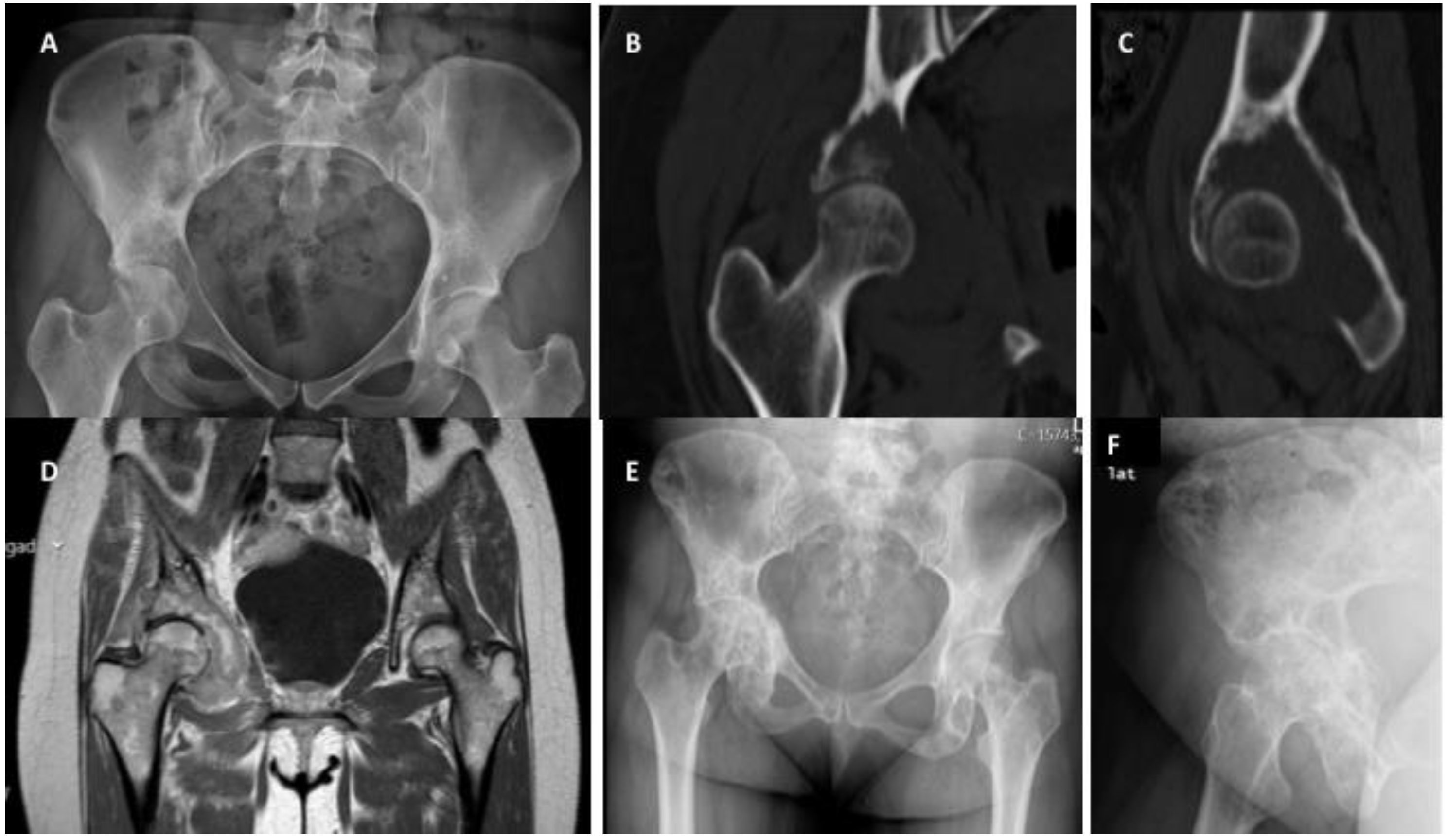
Figure 21. Right acetabular impending fracture in a female patient with breast cancer and multimetastatic bone disease: (A) anteroposterior pelvic radiograph showing a lytic lesion located in the right acetabulum, (B) pelvic coronal computed tomography showing in more detail the lytic bone metastasis on the right acetabulum, visible in plain radiograph, (C) sagittal computed tomography showing a detailed characterization of the lytic bone metastasis on the right acetabulum, (D) magnetic resonance coronal image showing the extension of breast cancer metastasis, occupying the right acetabulum, (E) pelvic anteroposterior radiograph showing an exceptional result three months after radiation and denosumab treatment of the impending fracture in (A), (F) alar view of the right acetabulum after radiation and denosumab treatment.
For pathologic fractures, and if stable bone reconstruction is achievable, osteosynthesis followed by RT and BTAs represents the first option. However, if stable reconstruction is not possible, bone segment replacement followed by EBRT and BTAs should be preferred (Figure 32).
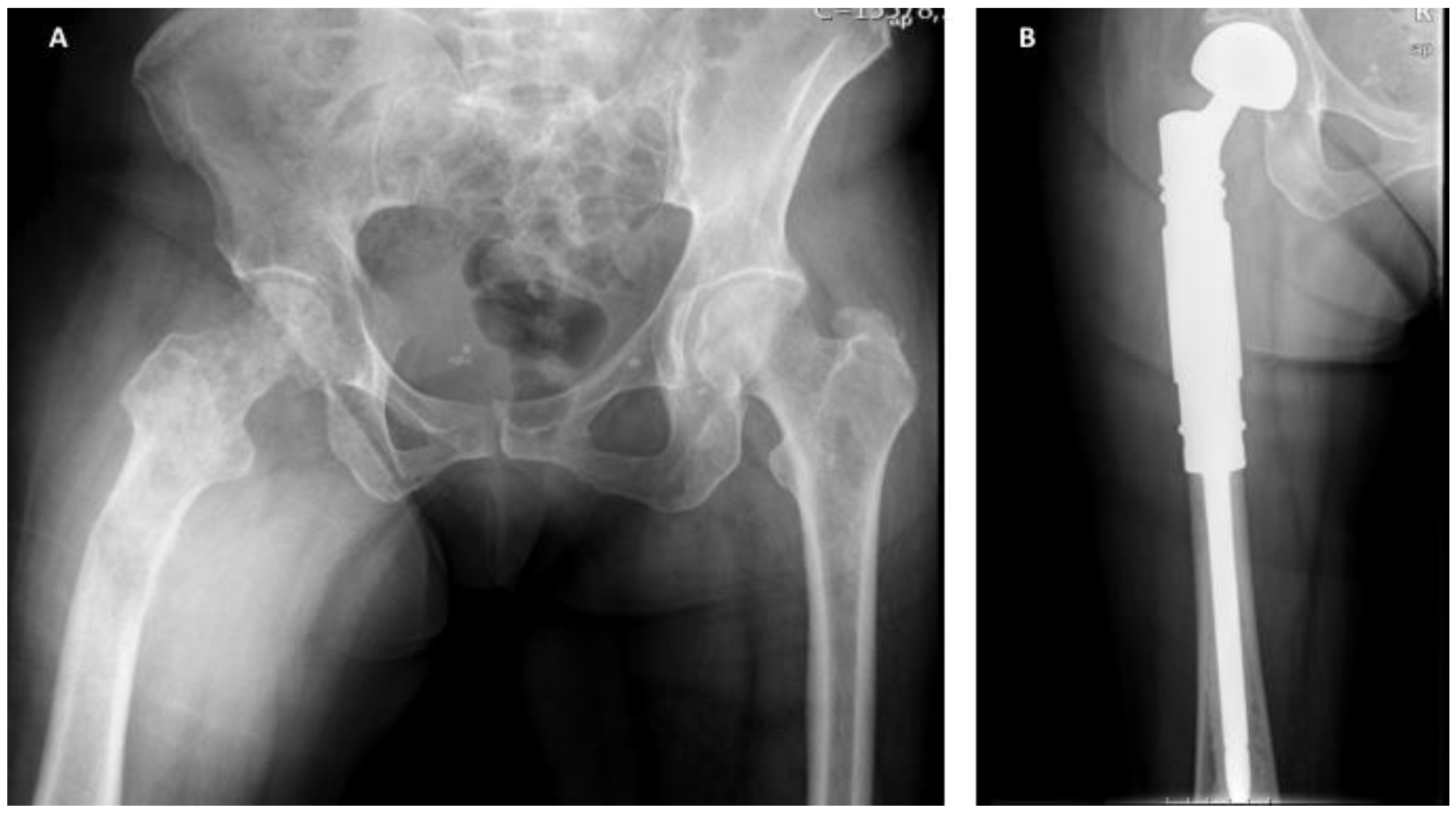
Figure 32. Extensive breast cancer bone metastasis in a female patient with multimetastatic bone disease: (A) anteroposterior pelvic radiograph showing a pathologic fracture in the right femur, not amenable for reconstruction due to extension of the metastatic bone disease, (B) immediate postoperative radiograph showing anteroposterior view of the right femur with a bipolar tumoral hip megaprosthesis, used to provide stability and pain relief. After surgery, the patient underwent local radiotherapy and bone-targeted agents.
2. Prostate Cancer Metastases
Prostate cancer often presents with BM, which are typically osteoblastic [105][4]. The process behind the development of osteoblastic metastases is still largely unknown but it seems to be related to the tumor production of osteoblastic factors, such as ET-1, growth differentiation factor 15, and bone morphogenic proteins [106][5]. Due to their osteoblastic nature, prostate BM display a lower probability of generating impending or pathologic fractures compared to other tumors, which is reflected in score systems, such as the one presented by Mirels (Table 1) [9][6].
Resection is the strategy of choice for patients presenting with solitary or oligometastatic disease, but similarly to breast carcinoma, these cases are extremely rare. For the more common cases, where patients have multimetastatic disease, the osteoblastic nature of metastases allows a watchful waiting approach, which is even more suitable for non-weight-bearing segments. Nonetheless, for impending (Mirels ≥ 9) or pathologic fractures, surgical stabilization or bone segment replacement should be performed as soon as possible. However, these procedures are extremely difficult due to the hardness and rigidity of prostate metastases, which can create drill or screw fractures during the surgical process (Figure 43).
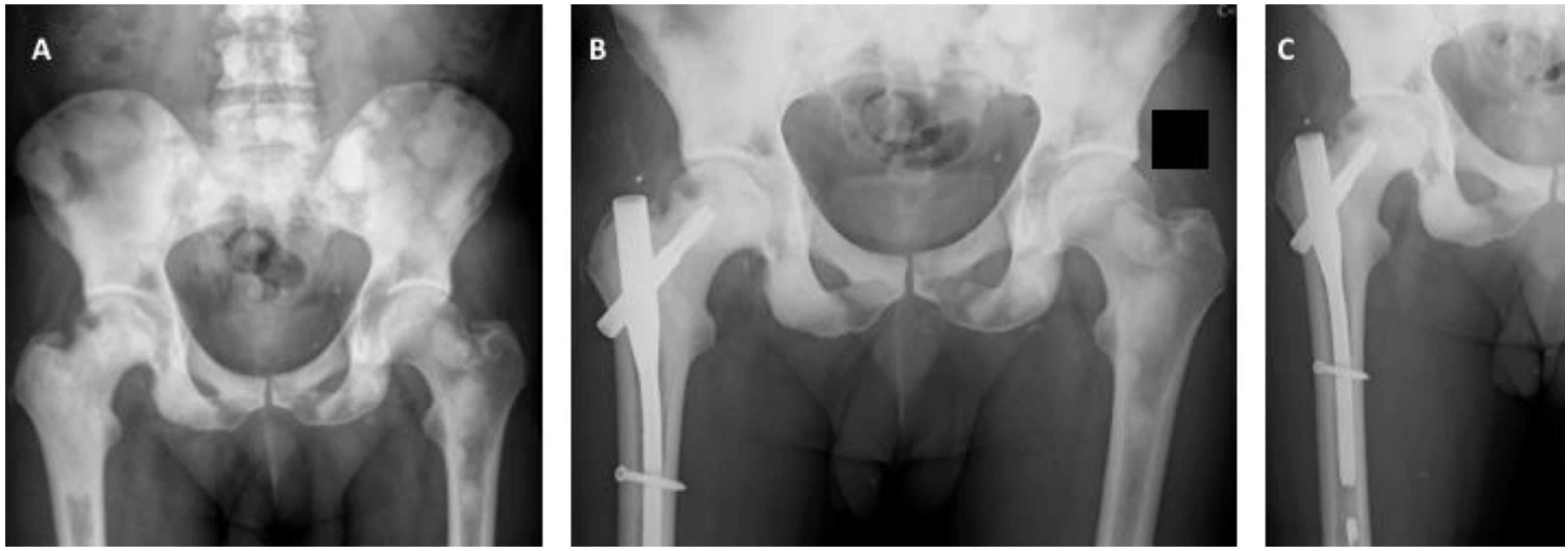
Figure 43. (A) Anteroposterior pelvic radiograph showing countless prostate carcinoma metastases around the lower spine, pelvis and proximal femur. Extensive invasion of the pertrochanteric area of the right proximal femur associated with mechanical pain can also be observed. (B) Postoperative anteroposterior radiograph of the pelvis after surgical stabilization of the right proximal femur metastasis using a cephalomedullary nail. (C) Anteroposterior radiograph of the right hip after surgical stabilization of prostate cancer metastasis in the proximal femur. A broken drill is visible in the medullary canal.
3. Lung Cancer Metastases
Lung carcinomas typically present with extensive metastatic disease and extremely osteolytic and destructive BM [107][7]. Similar to other tumor types, a wide resection should be attempted in the rare cases of patients with solitary metastatic disease. Despite the expected good response to radiation, bone metastases in the setting of lung carcinoma often present with pathologic fractures due to the highly destructive nature of the lesions (Figure 54). This destructive pattern makes reconstructive techniques difficult to execute. Although the same principle is true for impending fractures, radiation combined with BTAs can be attempted in cases with a Mirels score ≤7, and particularly for non-weight-bearing segments, since the probability of progress towards fracture is lower. Nevertheless, RT and additional BTAs should be added after the surgical procedure [108][8].
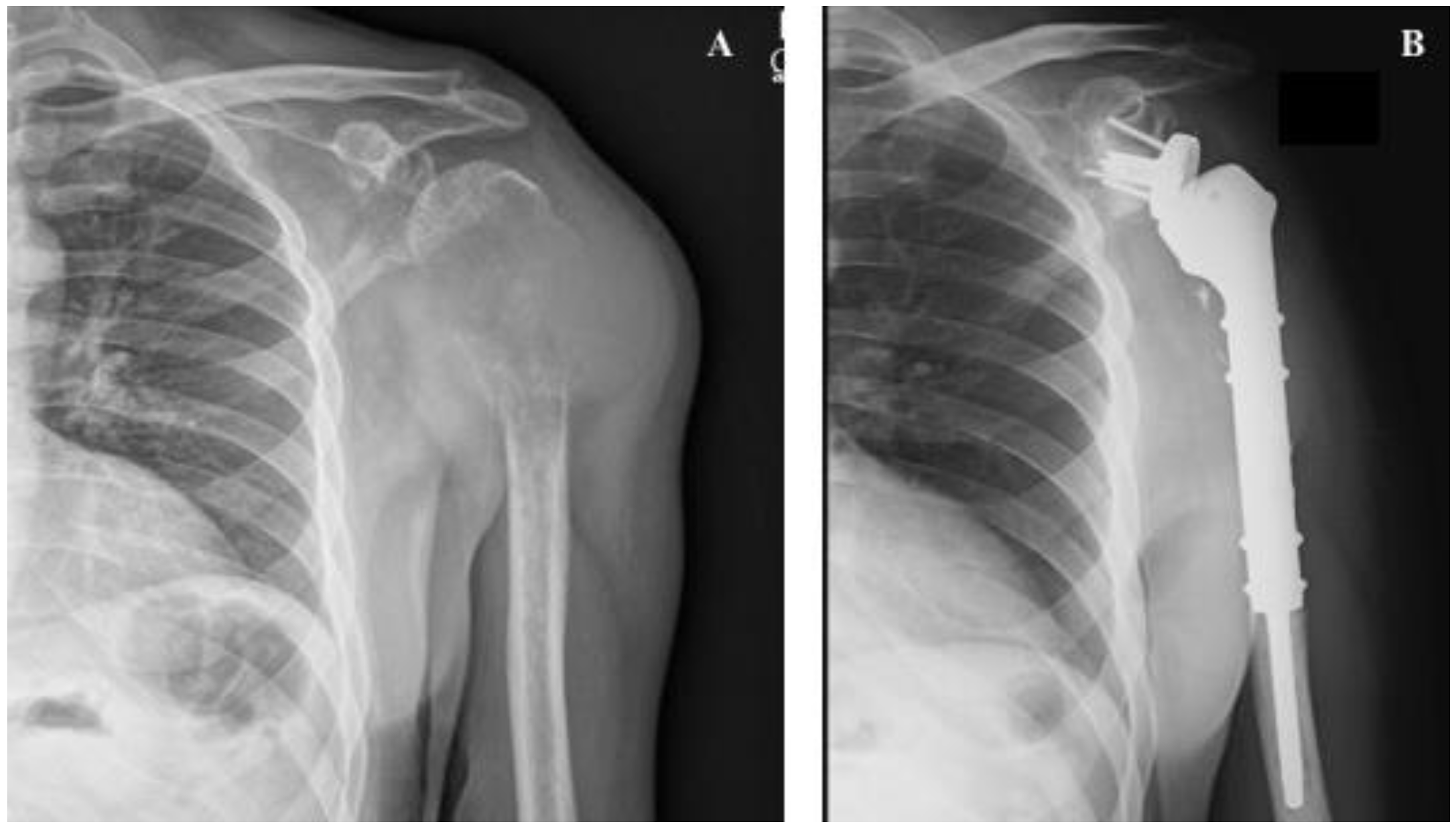
Figure 54. Shoulder megaprosthesis in a solitary proximal humerus lung metastasis: (A) preoperative image showing the left humerus with pathologic fracture secondary to lung carcinoma. An important soft tissue component is visible. (B) Postoperative image showing shoulder reverse megaprosthesis.
4. Renal Cancer Metastases
Renal cancer metastases are characterized by extensive lytic, highly vascularized bone lesions with the particular feature of being radiation-resistant [109,110][9][10]. Due to these features, renal cancer metastases almost always require surgery, either to provide stabilization or perform substitution of the bone segment or articulation (Figure 65). If open surgery is planned, preoperative embolization is of paramount importance to technically facilitate the procedure and minimize potentially life-threatening blood loss [111][11].
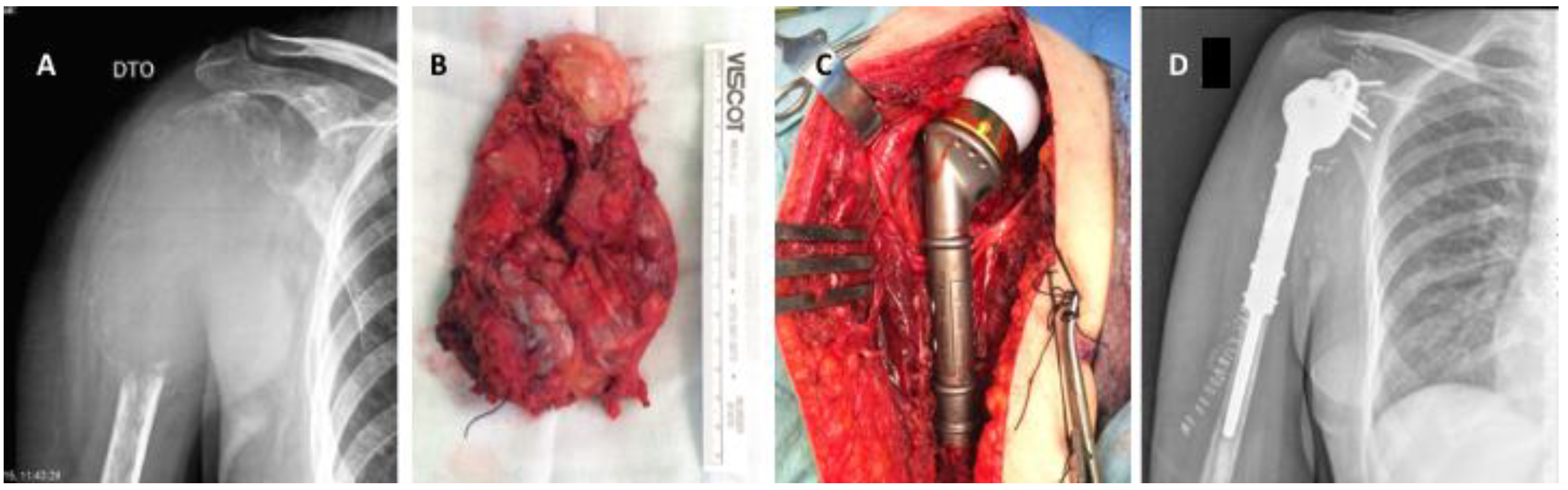
Figure 65. Shoulder megaprosthesis in a solitary kidney cancer metastasis in the proximal humerus: (A) preoperative image showing the right humerus with an extensive osteolytic lesion and pathologic fracture secondary to kidney carcinoma. An important soft tissue component is visible. (B) Tumor specimen after en bloc resection, (C) intraoperative image showing the tumoral megaprosthesis in place, (D) immediate postoperative anteroposterior radiograph.
As with all other carcinomas, patients with solitary or oligometastatic bone disease should undergo total tumor resection, while those with multimetastatic disease are candidates for a less aggressive surgical approach.