Your browser does not fully support modern features. Please upgrade for a smoother experience.
Please note this is a comparison between Version 2 by Catherine Yang and Version 1 by Khair Alhareth.
Pregnancy is a delicate state, during which timely investigation of possible physiological anomalies is essential to reduce the risk of maternal and fetal complications. Medical imaging encompasses different technologies to image the human body for the diagnosis, course of treatment management, and follow-up of diseases. Ultrasound (US) is currently the imaging system of choice for pregnant patients. However, sonographic evaluations can be non-effective or give ambiguous results. Therefore, magnetic resonance imaging (MRI), due to its excellent tissue penetration, the possibility of acquisition of three-dimensional anatomical information, and its high spatial resolution, is considered a valid diagnostical alternative.
- MRI
- magnetic resonance imaging
- pregnancy
1. Indications for MRI during Pregnancy
MRI was introduced in clinical practice in the early 1980s, and the first attempts to apply it among pregnant women were already reported in 1983 [10,11,12][1][2][3]. Commonly described indications for MRI during pregnancy can be classified into three main categories (Figure 1): non-obstetric, obstetric or gynecological, and fetal indications [13][4].
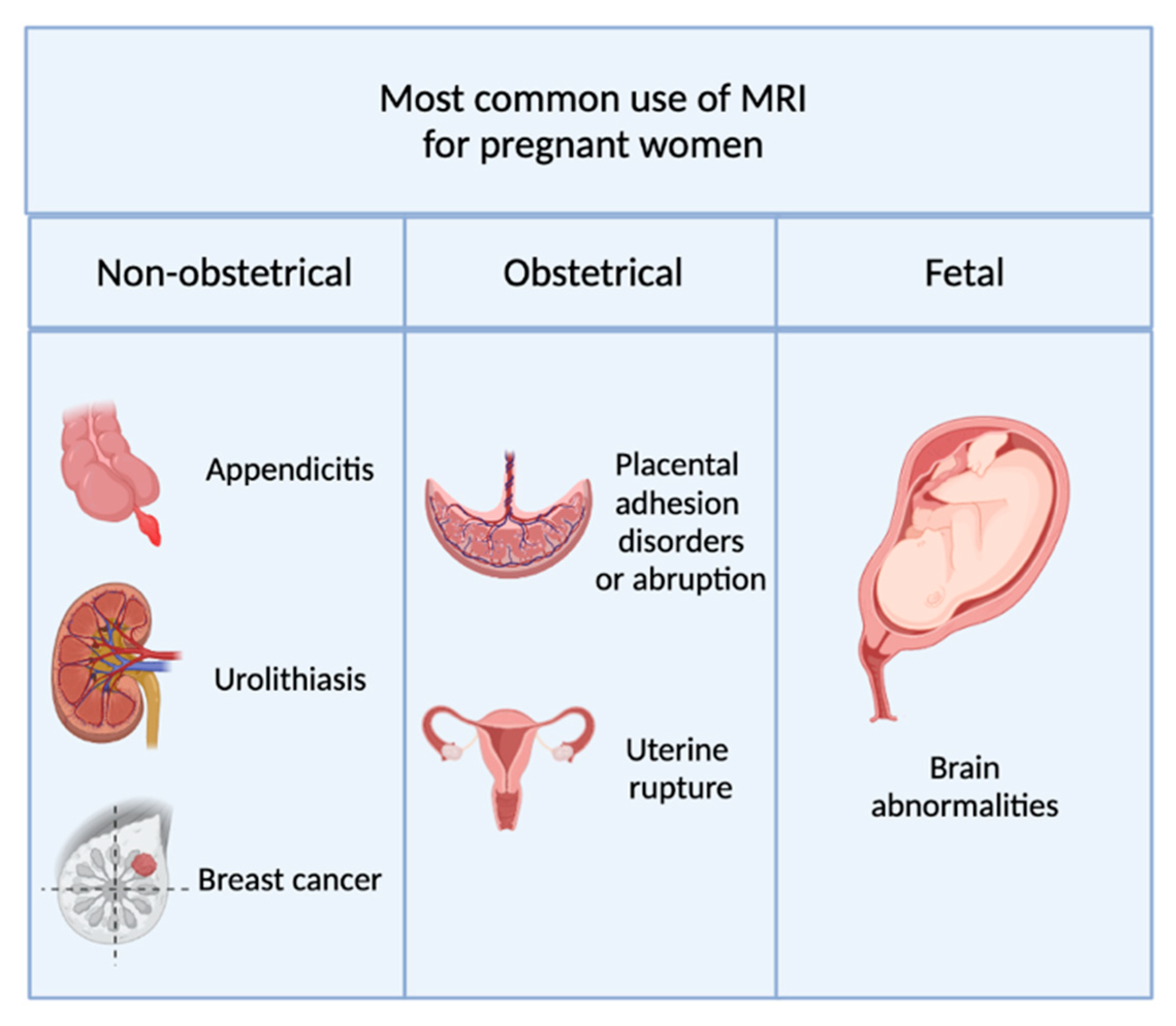
Figure 1.
Summary of the most common indications for MRI during pregnancy.
1.1. Non-Obstetric Indications
Pregnancy-associated anatomical changes, organ displacement (taking place especially during the second and third trimesters), physiological leukocytosis (elevated white blood cell count), and non-specificity of symptoms such as abdominal pain nausea and vomiting, render the diagnosis of various pathologies on pregnant patients harder [14,15][5][6].
Appendicitis is one of the most common non-obstetric causes of abdominal pain in pregnancy [13][4]. An early diagnosis is paramount to avoid unnecessary or negative surgical interventions and reduce the risk of fetal loss associated with the eventuality of appendiceal rupture or abscess [13,14,16][4][5][7]. MRI has been indicated by many as a powerful diagnostic tool for appendicitis, especially after inconclusive ultrasound examinations [13,14,16,17][4][5][7][8]. Other gastrointestinal and pancreaticobiliary pathologies that imply diagnosis by MRI are bowel obstruction, cholelithiasis, and pancreatitis [13][4].
Urologic pathologies such as urolithiasis and renal colic are other common reasons for pregnant women’s hospitalization. Early diagnosis is essential to prevent complications such as pyelonephritis or colic-induced preterm labor [13,15][4][6].
MRI can also be used as an alternative to US and CT for the diagnosis of cancer. Breast cancer is the most frequently diagnosed cancer in pregnant women [18,19][9][10]; other gynecological malignancies, such as cervical and ovarian cancer, or increasingly common colorectal cancers, may also prompt the need for MRI investigations [16,18,20][7][9][11]. This imaging system can also be applied in the evaluation of the brain, chest maternal diseases, musculoskeletal disorders, cardiovascular post-operative evaluation, and monitoring of congenital or acquired heart pathologies [21,22][12][13].
1.2. Obstetric and Gynecological Indications
Placenta adhesion disorders are among the most common obstetrical indications for MRI examinations and the cause of most failures in pregnancy [23][14].
Normally, the placenta is not in contact with the myometrium. In pathological conditions, according to how deeply placental tissues invade the myometrium, three cases can be distinguished:
-
Placenta accreta, in which placental villi adhere to the myometrium.
-
Placenta increta, where placental villi invade the myometrium.
The first-line diagnostic tool for this pathology is US. However, sonographic results are often equivocal and might leave uncertainty about the depth of placental invasion. Ultrasound visualization of this organ is also difficult in cases of posteriorly implanted placenta, where the latter is attached to the back wall of the uterus near the spine. In these situations, additional MRI imaging can be used [25][16]. The diagnosis of adhesion disorders is essential to plan the surgical management, contain the extent of possible hemorrhage at the moment of delivery, and detect eventual perforation of adjacent organs in case of percreta [14,16,21,26][5][7][12][17].
Placental abruption (the placenta detached prematurely from the myometrium after 20 weeks of gestation) represents another complication that in extreme cases could lead to fetal death [13][4]. Ultrasound detection of hematomas related to placental abruption is difficult and often leads to false diagnoses [13,21][4][12]. The use of MRI is helpful for correct identification [27][18].
Early detection of ectopic pregnancies (the fertilized ovum is implanted outside the uterine cavity) is crucial to prevent women’s mortality and preserve their fertility. MRI often allows for a more precise diagnosis compared to the transvaginal US, especially in cases of unusual presentations [24][15]. The use of MRI has also been reported in the context of the prediction of uterine rupture or individuation of ovarian torsions, adnexal masses, and fibroids [24,27][15][18].
1.3. Fetal Indications
Fetal MRI is employed in the structural and functional evaluation of the fetus [21,28][12][19]. Being mainly used for the individuation of CNS anomalies, MRI has also been implicated in the investigation of the neck, lungs (volumetric estimation), cardiac position and conformation, liver (congenital diaphragmatic hernias), bowel, and urinary tract [21,29][12][20].
2. Safety Issues of Non-Contrast-Enhanced MRI during Pregnancy
To create images, MRI exploits the interaction between protons of molecules within the body (mainly water) and an external magnetic field. In the absence of a strong magnetic field, protons in ourthe body spin around their axis. The axes of different protons are randomly oriented in space [30][21]. When the body is put inside a high magnetic field (1.5 T or 3T in clinical diagnostics [31][22]), all the protons axes align in the direction of the magnetic field, and a net magnetization, called longitudinal magnetization, is generated [32][23]. During the application of an opportune radiofrequency pulse (RF), the total magnetization is tilted out of alignment, and a new, transverse magnetization component arises. When the RF pulse is removed, both components of the magnetization return, or relax, to their previous states under the influence of the magnetic field. During this relaxation process, the body produces an RF signal, which is detected and processed to produce an image [32][23].
MRI images include areas of diverse shades of gray, which correspond to different body components. Endogenous contrast of MRI is due to chemical, physical, and proton density differences in tissues [31][22]. Because of these differences, tissues have different relaxation times, called longitudinal (T1) and transverse (T2), which are the cause of the different shades of gray in the MRI scan (Figure 2).
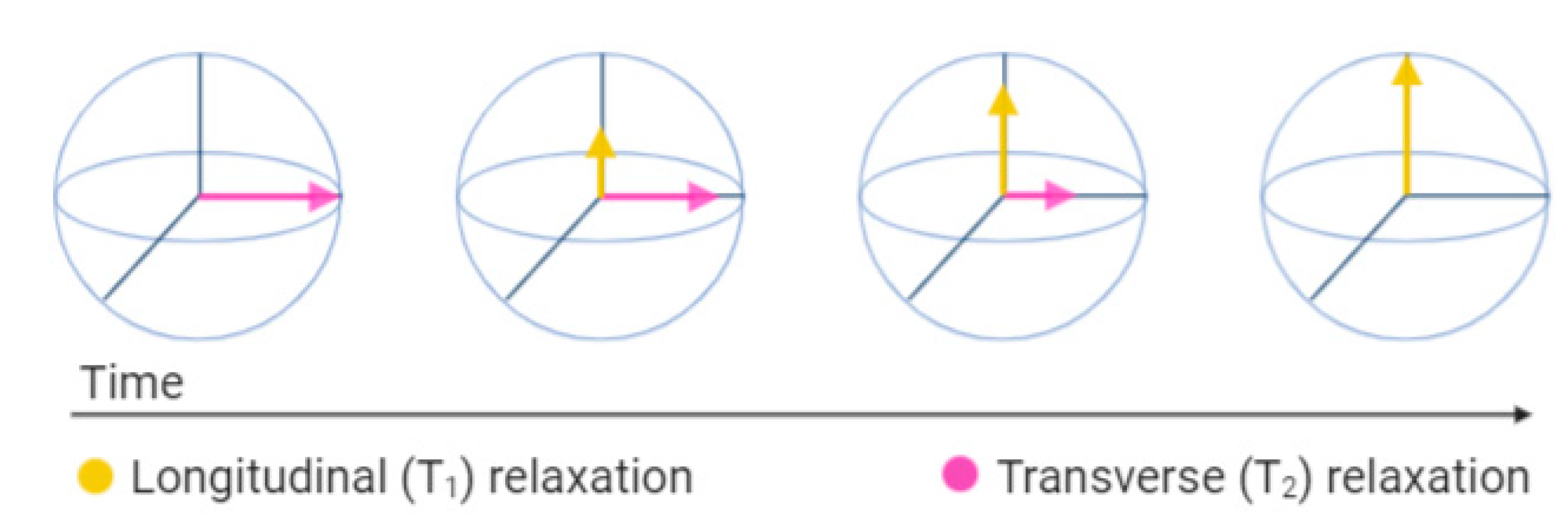
Figure 2.
Representation of the longitudinal (T
1
) and transverse (T
2
) magnetization vectors after the radiofrequency pulse (RF) is turned off.
To date, there are no data that have definitively demonstrated harmful effects on the fetus caused by MRI exposure of the pregnant woman in any trimester of gestation [12,13,33,34,35][3][4][24][25][26]. However, prospective and longitudinal studies are lacking; therefore, long-term safety has not yet been established [12,13,33,34,35][3][4][24][25][26]. The American College of Radiology (ACR), indeed, recommends pregnancy screening for women before MRI scanning. In the case of pregnancy confirmation, ACR advises the use of MRI only if [34][25]:
-
It is not prudent to delay the examination until the completion of pregnancy;
-
The information needed cannot be obtained through other non-ionizing techniques;
-
The data gained may influence the management of the patient or the fetus.
The main theoretical risks associated with the use of non-contrast MRI during pregnancy are due to the implication of strong static magnetic fields (1.5 T or 3 T commonly in clinical use), gradient fields, and radiofrequency pulses (RF) [4,12,13,33][27][3][4][24].
2.1. Static Magnetic Fields and Teratogenicity
It has been shown in vitro that cell migration, differentiation, and proliferation can be affected by static magnetic fields [4,12,13,35,36][27][3][4][26][28]. Static magnetic field exposure have shown teratogenic effects in animal studies [4,12,13,35][27][3][4][26]. This suggests potential negative effects on organogenesis during the first trimester of pregnancy. However, direct extrapolation from animal models is not applicable, and no study has shown any MRI-induced teratogenic effect on humans so far [4,12,13,35][27][3][4][26].
2.2. Gradient Fields and Hearing Damage
Rapid time-varying magnetic fields are responsible for the production of acoustic noise [4,12,13][27][3][4]. The American Academy of Pediatrics considers 90 dB to be the limit above which the ear of the fetus can suffer permanent damage [37][29]. MRI generates acoustic noise ranging between 80 dB and 120 dB [4,38][27][30]. Maternal tissues and amniotic fluid attenuates the sound around 30 dB, but since the exact value is still uncertain, MRI evaluations can theoretically represent a risk for fetal hearing damage [4,12,13,38][27][3][4][30]. Several retrospective studies have not found any evidence of hearing abnormalities due to fetal MRI exposure, but prospective studies are also lacking in this case [12][3].
2.3. Radiofrequency Pulses and Tissue Heating
Radiofrequency pulses energy into the body in the form of heat [4,12,13,35][27][3][4][26]. In humans, heat-induced abnormalities in the fetus have been associated with an increase in maternal temperature greater than 2–2.5 °C for 30–60 min [4,13,38][27][4][30]. Since the heat gradient decreases from the body surface to the center, fetal heat is usually less than what has been shown to be detrimental [4][27]. Animal studies on pigs did not find any substantial increase in fetus heat after 3 T MR examinations within 30 min of duration [12,33][3][24]. Human studies failed to demonstrate reproducible harmful effects of mother or fetus exposure to clinically used magnetic fields (1.5 T or 3 T) [33,39,40,41][24][31][32][33]. Therefore, scanning at up to 3 T for less than 30 min is considered safe by the ACR.
3. Safety Issues of Contrast-Enhanced MRI during Pregnancy
The endogenous contrast produced by body components is not always enough to appropriately decipher MRI images. MRI, indeed, suffers from low sensitivity [31][22]. Contrast-enhanced MRI (CE-MRI) is a magnetic resonance modality in which exogenous substances are administered to increase the quality of images [8][34].
The most common MRI contrast agents (CA) are either complexes of paramagnetic ions, such as gadolinium Gd3+ and manganese Mn2+, or superparamagnetic iron oxide nanoparticles (SPIONs) [42,43][35][36]. Paramagnetic contrast agents usually shorten T1 relaxation time, resulting in the enhanced part being brighter (positive agents), while iron oxide particles shorten T2, producing a darker enhanced area (negative agents) [42][35]. Different SPIONs have been used in the past in MRI imaging of liver, spleen, and lymph nodes [44][37]; however, due to poor commercial interest, iron and manganese-based contrast agents are no longer commercially available [43,44,45][36][37][38].
When the administration of contrast to pregnant women is strictly required, gadolinium is the only recommended solution, because no animal or human fetal studies assess the safety of other agents during pregnancy [2][39].
3.1. Safety of Contrast Agents Containing Gadolinium
Currently, clinically used contrast agents are gadolinium-based (GBCA). These substances shorten T1, making the enhanced part of the image brighter [42][35]. Due to its similar size to calcium (Ca2+) ion, paramagnetic Gd3+ can compete in biological processes in which calcium is involved, resulting in toxicity for the human body [6][40]. For this reason, agents for clinical use are complexes in which the Gd3+ ion is chelated by a ligand to prevent its release and reduce its toxicity [46][41]. Agents can be distinguished into linear or macrocyclic, ionic, and non-ionic, depending on the total charge of the complex and the molecular structure of the ligand [6][40]. Macrocyclic or ionic agents are usually considered safer than linear or non-ionic ones because of the smaller probability of Gd3+ release from the complexes [6,47][40][42].
The main safety concerns pertaining to the use of these contrast agents in pregnancy are associated with their potential to be teratogenic, induce neonatal nephrogenic systemic fibrosis (NSF), and bioaccumulate into tissues [12,13,47][3][4][42].
Teratogenicity
Different animal studies have demonstrated that GBCAs can cross the placenta after maternal intravenous administration [12,13,47,48,49][3][4][42][43][44]. Once in the fetal circulation, they undergo renal clearance and are excreted in fetal urine, re-entering the amniotic fluid [13,47,48,50][4][42][43][45]. Prolonged permanence of contrast agents in the amniotic fluid and possible fetal re-absorption may increase the risk of Gd3+dechelation, raising concerns about fetal safety [13,47,50][4][42][45]. Results of animal studies regarding the teratogenicity of GBCAs are controversial [12,47,48][3][42][43].
Different studies on humans have not shown any fetal harm attributable to gadolinium exposure during pregnancy [12,47,48][3][42][43]. However, they are limited by their retrospective data collection and small sample size [12,47,48][3][42][43]. The only cohort, longitudinal, and relatively large sample-size study, by Ray et al., did not demonstrate any increase in congenital anomalies after fetal exposure to gadolinium. However, a slight increase in the risk of stillbirth was reported in previously gadolinium-exposed neonates [51][46].
Nephrogenic Systemic Fibrosis
Nephrogenic systemic fibrosis (NSF) is a rare condition, mainly characterized by fibrosing skin lesions, which may also imply the fibrosis of internal organs [12,46][3][41]. Multiple studies have shown the connection between GBCAs exposure and the occurrence of NSF in subjects with renal impairment [12,46][3][41]. Fetal exposure to gadolinium raises concerns about the risk of neonatal NSF development [12,13][3][4]. Ray et al. have, indeed, found a higher rate of incidence of inflammatory, rheumatologic, and infiltrative skin conditions in neonates exposed to gadolinium compared to an unexposed group [51][46]. However, no NSFs have been reported so far in children under 6 years of age [12][3].
Bioaccumulation
Bioaccumulation of gadolinium in human tissues such as bone, skin, brain, or liver has been demonstrated by many post-mortem studies on subjects that underwent multiple exposures [12,46][3][41] Postnatal animal studies confirmed these findings, showing higher deposition degrees for linear agents than for macrocyclic ones [12,46][3][41]. Concerns regarding tissue deposition are related to potential gadolinium dechelation over time, resulting in the release of the toxic free ion [12][3]. However, the long-term consequences of gadolinium chelate bioaccumulation are still unknown.
In conclusion, the latest ACR, ACOG (American College of Obstetricians and Gynecologists), and ESUR (European Society of Urogenital Radiology) guidelines recommend avoiding the use of GBCAs during pregnancy, and their use is restricted only to patients for whom the benefits would considerably outweigh the risks for the fetus [2,33,52][39][24][47]. More specifically, the ESUR recommends, when strictly needed, administrating the lowest dose of the most stable agent [52][47].
In general, the use of diagnostical MRI on pregnant women is the best choice when ultrasound fails to provide sufficient information for a medical decision. However, the use of MRI during pregnancy should always be assessed through a case-by-case analysis, considering the benefits it could bring to the mother and her offspring against potential risks.