Conventional chemotherapy is the most common therapeutic method for treating cancer by the application of small toxic molecules that interact with DNA and cause cell death. Unfortunately, these chemotherapeutic agents are non-selective and can damage both cancer and healthy tissues, producing diverse side effects, and they can have a short circulation half-life and limited targeting. Many synthetic polymers have found application as nanocarriers of intelligent drug delivery systems (DDSs). Their unique physicochemical properties allow them to carry drugs with high efficiency, specifically target cancer tissue and control drug release. In recent years, considerable efforts have been made to design smart nanoplatforms, including amphiphilic block copolymers, polymer-drug conjugates and in particular pH- and redox-stimuli-responsive nanoparticles (NPs).
1. Introduction
After cardiovascular diseases, cancer is the second leading cause of death worldwide [
1]. Conventional chemotherapy is the most commonly used approach in cancer treatment, along with surgery, irradiation and immunotherapy [
2]. It is based on the application of small toxic chemotherapeutic molecules that interact with DNA molecules, modify them and induce cell death in cancer tissues [
3,
4]. Cancer cells have altered lipid and amino acid metabolic pathways, glycolysis, and redox homeostasis [
1,
5]. Indeed, altered energy metabolism with upregulated glucose transporter expression, disrupted redox homeostasis with upregulated glutathione transferase (GST) and high telomerase activityare responses that maintain DNA integrity, retaining replication, proliferation and cancer cell resistance [
1,
5,
6]. Chemotherapy has many disadvantages, including drug toxicity, rapid degradation, low specificity and limited targeting. In the last few decades, nanomedicine has assumed an important role in cancer therapy based on diverse tailor-made drug delivery systems (DDSs) [
7]. Nanomedicine produces materials with sizes ranging from 1–100 nm, which are used as drug nanocarriers with exceptional properties, such as their size, solubility, hydrophilicity, high specificity and a suitable drug-release profile. Nanocarriers also have an enhanced permeability and retention effect (EPR) due to their accumulation in cancer tissue with leaky vasculature [
8].
Chemotherapeutics are mostly drugs that are poorly soluble in water with a limited delivery to the target tissue. Encapsulation or entrapment of drugs in nanocarriers facilitates their transport in the circulation to the cancer tissue, inhibiting their rapid biodegradation and improving their bioavailability [
9]. Moreover, nanocarriers with incorporated drugs provide a longer circulation half-life of drugs, increasing their efficacy and enabling a lower dose of application [
2,
9]. Compared with natural polymers, synthetic nanocarriers can be tailored to control the release of encapsulated drugs by modifying their structure [
10].
2. Polymeric Nanoparticles (NPs)
Polymeric NPs are particles obtained from natural, semi-synthetic or synthetic polymers. Polymeric nanosystems are produced by a polymerization reaction of many monomer units, and under certain conditions, they can be organized and self-assemble with ananometric size (10–100 nm) [
10,
11,
12]. Due to the high diversity of their properties, NPs attract great attention as multifunctional nanocarriers in DDSs [
9,
11]
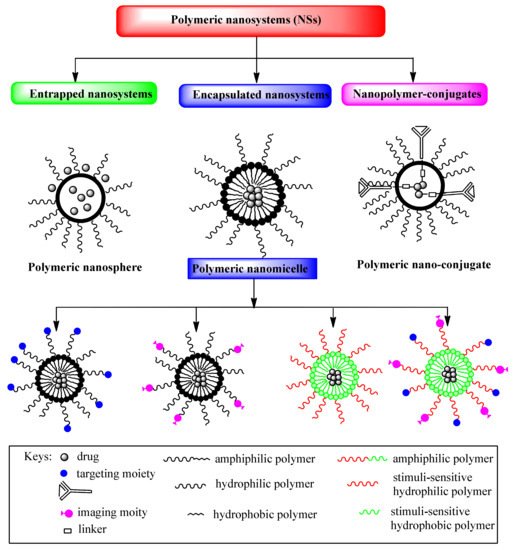
Depending on the preparation method, drugs can be entrapped, encapsulated or bound to polymeric NPs in the form of a nanosphere, a nanocapsule or a drug conjugate (
Figure 1) [
7,
9,
10]. Nanospheres are colloidal particles that entrap the drug inside their matrix by physical dispersion or by adsorption on the particle surface, while nanocapsules are systems consisting of a core cavity with an encapsulated drug and polymeric shell surrounding it. Polymeric capsules can be designed by the conjugation of targeting ligands that increase selectivity for cancer cells and improve intracellular drug delivery, as well as reducing different side effects and drug toxicity. Targeting ligands of polymeric capsules are commonly monoclonal antibodies (mAbs) or antibody fragments, aptamers, peptides and small molecules, such as folic acid, which are conjugated to the shell-forming block [
13,
14,
15,
16,
17,
18,
19]. These ligands are specifically bound to antigens or receptors that are overexpressed on the cancer cell [
20] and they enable cellular selectivity and intracellular delivery of polymeric micelles [
13]. Different designed polymeric capsules suitable for targeting the release of drugs are shown in
Figure 1. The efficacy of polymeric carriers modified with targeting ligands depends on the ligand properties, such as their density and binding affinities to receptors, which can enhance receptor internalization and the biodistribution of drugs. Drug-conjugates have a drug that is chemically bonded to the polymer through a linker/spacer. The bond drug-linker/spacer is a common breakage-point when the drug is released at the target site (
Figure 1).
Figure 1. Schematic illustration of multifunctional drug delivery systems.
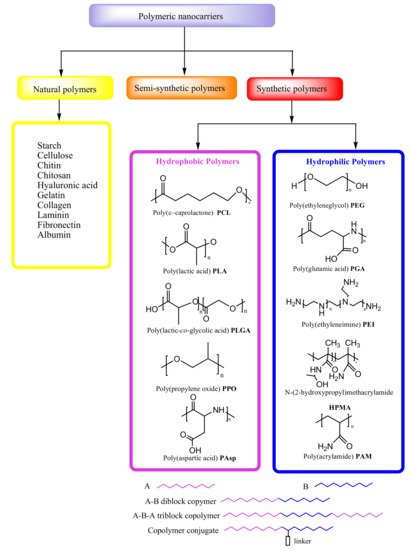
Natural polymers are biopolymers, including different classes of polysaccharides and proteins, which, due to their biocompatibility and biodegradability, are particularly suitable for medical applications, as in cell-based transplantation, tissue engineering and gene therapy [
10] (
Figure 2). Natural polymers can be combined with synthetic molecules through the chemical modification of their functional groups and so-called semi-synthetic polymers can mimic human tissue components. In formulations of controlled DDSs, synthetic polymers attract more attention than biopolymers due to the considerable potential for the design of their structure and modifications of their physicochemical properties (
Figure 2) [
8]. Synthetic polymeric micelles exhibita high capacityto incorporate a broad range of bioactive molecules, such as antisense oligonucleotides [
21], plasmid DNA [
22], proteins [
23], small interfering ribonucleic acids (siRNAs) [
24], messenger RNAs (mRNAs) [
25] and photosensitizers [
26], by tailoring the core-forming segments of the block copolymers. In fact, several poly-ion complex (PIC) micelles have been designed that incorporate negatively charged biomolecules by electrostatic interaction with positively charged block copolymers [
21,
27]. In addition, they can be stabilized by the covalent crosslinking of their core through disulfide bonds [
28], which can be cleaved under specific intracellular conditions, enabling the complexes to escape from endosomal compartments after endocytosis and to deliver the biomolecules to subcellular destinations [
29] without drug degradation. By introducing hydrophobic molecules such as cholesterol to the core [
30], PIC micelles become more stable, with a longer half-life in the bloodstream, allowing for the delivery of intact biomolecules to therapeutic targets. PIC micelles obtained from block copolymers with a core-forming polycation such as polyaspartamides, support enhanced delivery of biomacromolecules to the cytosol of cells, and the gene transfection in vitro and in vivo [
25,
29,
30,
31,
32,
33,
34,
35].
Figure 2. Types of polymeric nanocarriers.
In recent years, the great potential of synthetic polymers as drug carriers has been highlighted, particularly because of the possibility to develop DDSs with a target sustained/controlled release of drugs [
1]. The encapsulation of cancer drugs in polymeric micelles with modifications for cancer targeting and triggered release results inmore efficient drug delivery (
Figure 1).
In addition to biocompatibility and biodegradability, synthetic polymers used in DDSs should be activated at the site of action, to be stable in blood circulation, to have low toxicity and immunogenicity, and to provide protection fromthe degradation of drugs before the target tissue is reached. Additionally, it is necessary that polymer nanocarriers of DDSscan be easily synthesized without impurities [
8].
3. Amphiphilic Block Copolymers as Carriers in Drug Delivery Systems
3.1. Hydrophobic and Hydrophilic Polymeric Nanocarriers
Polymeric micelles are the most common nanocarriers of DDSs as
regards the original core-shell structure [
8]. They consist of amphiphilic block copolymers with hydrophilic and hydrophobic units that self-assemble in water solution at the critical micelle concentration (CMC). Micellar polymeric units can be formed in different ways, such as diblock copolymers (A-B), triblock copolymers (A-B-A) and copolymer conjugates (
Figure 2) [
9].
The hydrophobic core is suitable for encapsulating poorly water-soluble drugs, and the pharmacokinetics of drug release can be controlled by its modification. The most frequently used hydrophobic polymers for core formation of NPs are: poly(ε-caprolactone) (PCL), poly(lactic acid) (PLA), poly(lactic-
co-glycolic acid) (PLGA), poly(propylene oxide) (PPO) and poly(aspartic acid) (PAsp) (
Figure 2). The hydrophilic polymers that are most frequently considered for the hydrophilic shell of NPs in DDS include poly(ethylene glycol) (PEG), poly(glutamic acid) (PGA), poly(ethyleneimine) (PEI), N-(2-hydroxypropyl)methacrylamide (HPMA) and poly(acrylamide) (PAM) (
Figure 2). A frequently used hydrophilic polymer of DDSs is PEG, which providesdistinctstability to NPs due to the reduction of nonspecific interactions with blood proteins, thus preventing their aggregation [
36].
3.2. Block Copolymers of DDSs in Cancer Therapy
Poly(ethylene glycol)-b-poly(ε-caprolactone)(PEG-PCL) is a polyether-polyester diblock copolymer, synthesized by ring-opening polymerization of ε-caprolactone and PEG [
37]. It is suitable for a variety of DDSs because ofits high biocompatibility, biodegradability and low toxicity. Many DDSs based on PEG-PCL with different hydrophilic/hydrophobic ratios (PEG/PCL) have been obtained, enablinghigher cellular internalization byincreasingPEGcontribution(PEG/PCL = 5/5) [
38]. Çırpanlı et al. have recently developed PEG-PCL nanocarriers for the controlled delivery of camptothecin (CPT), whose active lactone form was maintained by drug entrapment to hydrophobic PCL, preventing drug hydrolysis in the carboxylate inactive form (
Table 1) [
39]. Furthermore, Hu et al.have designed a nanoplatform with paclitaxel (PTX) encapsulated in a triblock PCL-PEG-PCL copolymer that in combination with circadian chrono-modulated chemotherapy confirmed sustained drug release and a lower cytotoxic effect compared with free PTX injection [
40]. Hong et al. obtained image-guided polymeric micelles, including a folate-conjugated PEG-b-PCL copolymer loaded with doxorubicin (DOX) and superparamagnetic iron oxide nanoparticles (SPIONs) [
41]. Active targeting was achieved by the conjugation of folic acid to the PEG-b-PCL shell-forming block, allowing micelles to specifically bind to receptors for folic acid that are overexpressed on the tumor cells. Drug-delivery efficiency and diagnostics were considerably improved by the combination of active tumor targeting and imaging in human hepatic carcinoma cells (Bel 7402 cells). Bel 7402 cells overexpress surface receptors for folic acid that bind these folate-conjugated polymeric micelles, providing targeted delivery of DOX to the cancer cells and exhibiting high inhibition of proliferation as compared to non-targeted micelles. The epidermal growth factor receptor (EGFR) is a transmembrane glycoprotein with an intracellular tyrosine kinase domain, which is overexpressed on the cells of solid cancers [
42]. Lee et al. developed EGF-receptor-targeted PEG-b-PCL micelles with incorporated DOX and labeled with
111In. Images were taken with micro-SPECT/CT intratumoral distribution of both targeted and non-targeted micelles confirmedenhanced accumulation in tumor tissue with the targeted micelles (T-BCM) as compared to non-targeted micelles (NT-BCM) [
43].
Table 1. Polymeric-anticancer drug nanoparticles (NPs), their loading mode and function.
|
Polymer
|
Drug
|
Loading Mode
|
Function
|
Reference
|
|
PEG-PCL
|
Camptothecin (CPT)
|
Entrapment
|
Colon, breast, ovarian, lung and brain cancers
|
[39]
|
|
PCL-PEG-PCL
|
Paclitaxel (PTX)
|
Encapsulation
|
Lung cancers in combination with chrono-modulated chemotherapy
|
[40]
|
|
PLGA-PEG
|
Paclitaxel (PTX)
|
Encapsulation
|
Breast, pancreatic and ovarian and brain cancers
|
[44]
|
|
PLGA-TPGS
|
Doxorubicin(DOX)- Metformin (Met)
|
Encapsulation
|
Multidrug resistance P388 cancer cell lines
|
[45]
|
|
PEG-PGlu
|
Cisplatin
|
Encapsulation
|
Solid cancers
|
[50,51,52]
|
|
mPEG-PLGA-PGlu
|
Doxorubicin(DOX)
|
Encapsulation
|
Breast cancer
|
[54]
|
|
PEG-PAsp
|
Paclitaxel (PTX)
|
Entrapment
|
Advanced stomach cancer
|
[55,56,57]
|
|
PEO-b-PAsp
|
Doxorubicin
|
Entrapment
|
Pancreatic cancer
|
[58]
|
|
PEO-PPO-PEO
|
Doxorubicin.
|
Encapsulation
|
Metastatic adenocarcinoma of the esophagus and gastroesophageal junction
|
[59,60]
|
|
PCLLA-PEG-PCLLA
|
Doxorubicin (DOX)
|
Encapsulation
|
Breast cancer
|
[61]
|
|
PEI-PLA
|
Paclitaxel (PTX)
|
Entrapment
|
Lung cancer
|
[62]
|
|
PEG
|
Camptothecin (CPT)SN38 Irinotecan (C-11)
|
Copolymer-drug conjugation
|
Colorectal, metastatic breast cancer, platinum-resistant ovarian cancer and metastatic cervical cancer
|
[63,64,65,66,67,68]
|
|
HPMA
|
Doxorubicin (DOX)
|
Copolymer-drug conjugation
|
Lung and breast cancer
|
[69,70]
|
|
HPMA
|
Paclitaxel (PTX)
|
Copolymer-drug conjugation
|
Solid cancers
|
[71]
|
|
HPMA
|
Diaminocyclohexane(DACH)-platinum
|
Copolymer-drug conjugation
|
Solid cancer, ovarian cancer
|
[72,73,74,75]
|
3.3. Polymer-Drug Conjugates in Cancer Therapy
Some PEG- and HPMA-drug conjugates are approved by the FDA and have found clinical application due to their excellent properties, such as good solubility in water and many organic solvents, high hydrophilicity, low toxicity and immunogenicity [
88,
89]. Several important polymer-drug conjugates used in cancer therapy are summarized in
Table 1.
PEG-based conjugates with the drugs camptothecin (CPT), camptothecin derivatives, SN38 and irinotecan (C-11), used as topoisomerase I inhibitors, have progressed to phases I and II of clinical studies [
63,
64,
65]. These PEG-based conjugates carry the drugs in a lactone-active form bonded to PEG through a glycine spacer. The PEG-CPT conjugate known as prothecan displayed low toxicity and satisfactory tolerance in phase II studies in patients with adenocarcinoma of the stomach and the gastroesophageal (GE)junction, although it confirmed significantly lower drug loading (1.7%) than other polymer-drug conjugates [
63]. PEG-SN38 (EZN-2208) and PEG-irinotecan (NKTR-102) conjugates were synthesized by coupling a 4 arm PEG of 40 kDa with SN38 and irinotecan, respectively [
66,
67]. Irinotecan is a derivative of SN38 containing an additional bis-piperidine group, which the PEG-irinotecan conjugate releases at the targeting site of action, forming the active metabolite SN-38. However, the PEG-SN38 conjugate provided a longer half-life of SN38 in the circulation and it is up to a 245-fold more efficient thanPEG-irinotecan conjugate in human cancer cell lines [
67]. The anticancer activity of PEG-SN38 was revealed in the therapy of breast, colorectal and pancreatic cancers. The PEG-irinotecanconjugate had a half-life of 15 days compared to 4 h for free irinotecan [
75]. The PEG-irinotecan conjugate combined with cetuximab has entered into phase II study in the therapy of ovarian, breast, colorectal and cervical cancers [
68].
4. Stimuli-Responsive Polymer-Drug Conjugates
In the last two decades, many smart nanoplatforms have been designed by introducing stimuli and targeting moieties into polymers of DDSs [
93,
94,
95,
96,
97]. Some pH- and redox-responsive polymeric NPs are described here as the most commonly used triggers in DDSs.
Due to increased aerobic glycolysis, cancer cells have an acidic environment (pH 6.5–7.2), in particular the intracellular organelles such as endosomes (pH 5–6) and lysosomes (pH 4–5) [
93]. Therefore, many pH-responsive DDSs were designed by covalent attachment of the drug to the polymeric NPs via an acid-labile bond. Bae et al. created diblock PEG-b-Pasp copolymers conjugated with the drug adriamycin via a hydrazone bond, which can be easily cleaved under the acidic conditions found in cancer cells, followed by rapid release of the drug and break-up of copolymers [
93]. The hydrazone bond of diverse nanoplatforms has been successfully applied to transport different anticancer drugs such as DOX, PCX and cisplatin [
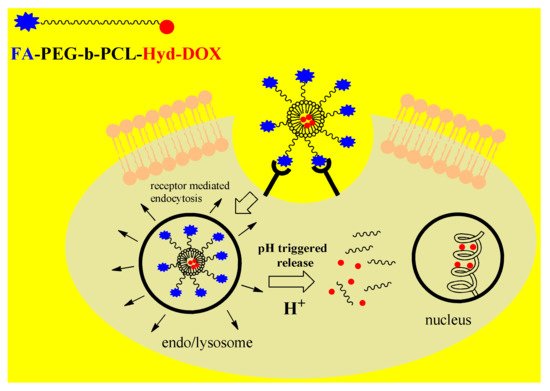
8]. Guo et al. designed a multifunctional polymeric-drug conjugate, FA-PEG-b-PCL-hyd-DOX, with a diblock PEG-PCL copolymer bound to DOX via a labile hydrazone bond, and decorated with folic acid (FA) [
8]. This DDS exerts cancer targeting ability through the folate receptor (FR) interfering with endocytosis and pH-triggered drug release by the breaking of the hydrazine bond under acidic conditions (
Figure 3).
Figure 3. Mechanism of action of pH-responsive polymer nanoparticles(NPs) decorated with targeting ligand folic acid (FA) and with the drug doxorubicin(DOX)bound via a hydrazone bond to diblock copolymerPoly(ethylene glycol)-b-poly(ε-caprolactone)(PEG-PCL).
Due to the increased concentration of glutathione (GSH)in the cytosol and subcellular organelles, there is a redox potential difference between the intra- and extracellular micro environments of normal cellsthat is larger in cancer cells because of the 2- to 4-fold higher concentration of GSH [
8]. The significant increase in the intracellular redox potential was used as an internal stimulus for creating intelligent DDSs by introducing a redox-sensitive functional group into the polymeric nanocarriers or reducible linker. Similar to the previously described polymeric-drug conjugate, FA-PEG-b-PCL-hyd-DOX, Shi et al. designed a redox-responsive FA-PECL
SS-DOX nanocomplex by linking PEG and PCL polymers via a redox-sensitive disulfide bond [
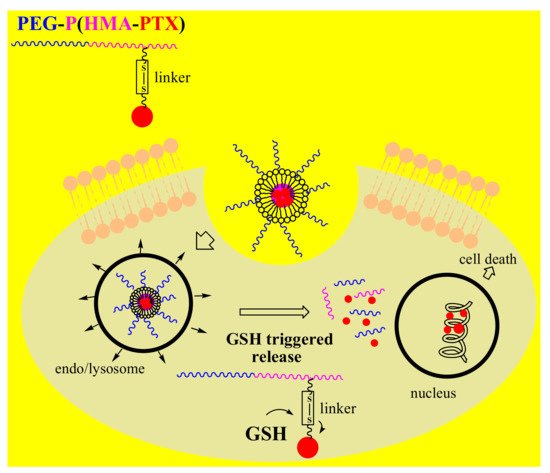
96]. Thus, as a result of stimulation by the acidic and reducing medium of cancer cells, GSH triggered DOX release by breaking the disulfide bond, with the drug efficiently killing the cancer cells. Recent studies have also introduced a novel multifunctional redox-responsive DDS based on the amphiphilic diblock PEG-b-PHEMA copolymer and covalently bounded PTX via a disulfide linker to poly(2-hydroxyethyl methacrylate)PHEMA in NPs (
Figure 4) [
97]. This biocompatible polymer-drug conjugate, PEG-b-P(HEMA-PTX),possessedglutathione-dependent cytotoxicity, providing higher proliferation inhibition in glutathione monoester-pretreated HeLa cells than in non-pretreated HeLa cells.
Figure 4. Mechanism of action of redox-responsive polymernanoparticles (NPs) with bonded drug PTX via a disulfide linker to diblock copolymerPoly(ethylene glycol)-b-poly(2-hydroxyethyl methacrylate)(PEG-b-PHEMA).