Current medical treatment for inflammatory bowel disease (IBD) does not achieve 100% response rates, and a subset of refractory and severely ill patients have persistent active disease after being treated with all possible drug alternatives. Ustekinumab plus vedolizumab and vedolizumab plus anti-TNF were the most used biological therapies (CoT) for Crohn’s disease. For ulcerative colitis, the most used CoTs were vedolizumab plus anti-TNF and vedolizumab plus tofacitinib.
- inflammatory bowel diseases
- biologic treatment
- combination
1. Introduction
2. Global Efficacy and Safety of CoT
3. Usefulness and Safety of Biologic Combinations
Figure 1 shows the pooled rates of clinical response, clinical remission endoscopic response, endoscopic remission, and adverse event rates for the most used CoTs.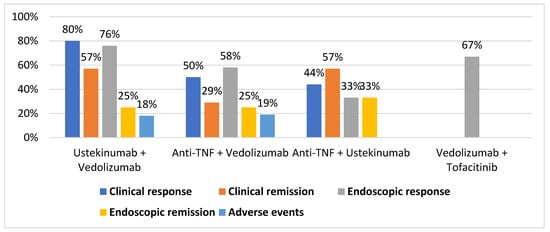
Table 1 shows the rates of clinical response, clinical remission, endoscopic response, endoscopic remission, and adverse event rates for each CoT.
| Clinical Response | Clinical Remission | Endoscopic Response | Endoscopic Remission | Adverse Events | ||
|---|---|---|---|---|---|---|
| Ustekinumab + Vedolizumab | Yang et al. | 5 of 7 | 4 of 7 | 5 of 8 | 2 of 8 | 1 of 8 |
| Kwapisz et al. | 4 of 5 | 0 of 5 | ||||
| Privitera et al. | 3 of 3 | 1 of 3 | ||||
| Glassner et al. | 11 of 13 | |||||
| TOTAL | 12 of 15 (80%) | 4 of 7 (57%) | 16 of 21 (76%) | 2 of 8 (25%) | 2 of 11 (18%) | |
| Anti-TNF + Vedolizumab | Yang et al. | 5 of 12 | 4 of 12 | 4 of 12 | 3 of 12 | 2 of 12 |
| Kwapisz et al. | 5 of 8 | 3 of 8 | ||||
| Privitera et al. | 3 of 6 | 3 of 6 | 1 of 6 | |||
| Glassner et al. | 24 of 36 | |||||
| TOTAL | 13 of 26 (50%) | 7 of 18 (29%) | 28 of 48 (58%) | 3 of 12 (25%) | 5 of 26 (19%) | |
| Anti-TNF + Ustekinumab | Yang et al. | 1 of 3 | 1 of 3 | 1 of 3 | 1 of 3 | |
| Kwapisz et al. | 2 of 2 | |||||
| Privitera et al. | 1 of 4 | 3 of 4 | ||||
| TOTAL | 4 of 9 (44%) | 4 of 7 (57%) | 1 of 3 (33%) | 1 of 3 (33%) | ||
| Secukinumab + Vedolizumab | Privitera et al. | 2 of 2 | ||||
| TOTAL | 2 of 2 (100%) | |||||
| Vedolizumab + Apremilast | Privitera et al. | 1 of 1 | 1 of 1 | |||
| TOTAL | 1 of 1 (100%) | 1 of 1 (100%) | ||||
| Vedolizumab + Tofacitinib | Glassner et al. | 8 of 12 | ||||
| TOTAL | 8 of 12 (67%) |
34. Summary
The most-used CoTs are shown in Table 2. Of them, vedolizumab plus ustekinumab and vedolizumab plus anti-TNF were the most effective CoTs for CD. Furthermore, vedolizumab plus anti-TNF and vedolizumab plus tofacitinib were the most effective CoTs for UC. The combination of ustekinumab and vedolizumab seems especially attractive because it might combine efficacy, safety, and persistence over time. Very recently, Stone et al. reported similarly good results in a retrospective series of 10 patients [12]. Data are preliminary and, in patients with UC and uncontrolled extraintestinal manifestations, CoT including anti-TNF or tofacitinib might be more effective.
| Study | VEDO+ USTE |
AntiTNF+ VEDO |
AntiTNF+ USTE |
TOFA+ VEDO |
TOFA+ USTE |
TOFA+ TNF |
Other ** |
|---|---|---|---|---|---|---|---|
| Goessens et al. * [13] | 16 | 36 | 8 | 12 | - | 1 | 8 |
| Glassner et al. [11] | 25 | 7 | 8 | 3 | 9 | 1 | |
| Kwapisz et al. [14] | 5 | 8 | 2 | ||||
| Privitera et al. ** [10] | 3 | 6 | 4 | 3 | |||
| Yang et al. [9] | 8 | 13 | 3 | ||||
| TOTAL | 62 | 75 | 20 | 21 | 3 | 10 | 19 |
References
- Raine, T.; Bonovas, S.; Burisch, J.; Kucharzik, T.; Adamina, M.; Annese, V.; Bachmann, O.; Bettenworth, D.; Chaparro, M.; Czuber-Dochan, W.; et al. ECCO Guidelines on Therapeutics in Ulcerative Colitis: Medical Treatment. J. Crohn’s Colitis 2021, 16, 2–17.
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, T.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohn’s Colitis 2020, 14, 4–22.
- Colombel, J.F.; Reinisch, W.; Mantzaris, G.J.; Kornbluth, A.; Rutgeerts, P.; Tang, K.L.; Oortwijn, A.; Bevelander, G.S.; Cornillie, F.J.; Sandborn, W.J. Randomised clinical trial: Deep remission in biologic and immunomodulator naïve patients with Crohn’s disease—A SONIC post hoc analysis. Aliment. Pharmacol. Ther. 2015, 41, 734–746.
- Hirten, R.P.; Iacucci, M.; Shah, S.; Ghosh, S.; Colombel, J.F. Combining Biologics in Inflammatory Bowel Disease and Other Immune Mediated Inflammatory Disorders. Clin. Gastroenterol. Hepatol. 2018, 16, 1374–1384.
- Grieco, M.J.; Remzi, F.H. Surgical Management of Ulcerative Colitis. Gastroenterol. Clin. N. Am. 2020, 49, 753–768.
- Ricart, E. Current status of mesenchymal stem cell therapy and bone marrow transplantation in IBD. Dig. Dis. 2012, 30, 387–391.
- Gold, S.L.; Steinlauf, A.F. Therapy in Patients With Inflammatory Bowel Disease: A Review of the Literature. Gastroenterol. Hepatol. 2021, 17, 406–414.
- Ribaldone, D.G.; Pellicano, R.; Vernero, M.; Caviglia, G.P.; Saracco, G.M.; Morino, M.; Astegiano, M. Dual biological therapy with anti-TNF, vedolizumab or ustekinumab in inflammatory bowel disease: A systematic review with pool analysis. Scand. J. Gastroenterol. 2019, 54, 407–413.
- Yang, E.; Panaccione, N.; Whitmire, N.; Dulai, P.S.; Casteele, N.V.; Singh, S.; Boland, B.S.; Collins, A.; Sandborn, W.J.; Panaccione, R.; et al. Efficacy and Safety of Simultaneous Treatment with Two Biologic Medications in Refractory Crohn’s Disease. Aliment. Pharmacol. Ther. 2020, 51, 1031–1038.
- Privitera, G.; Onali, S.; Pugliese, D.; Renna, S.; Savarino, E.; Viola, A.; Ribaldone, D.G.; Buda, A.; Bezzio, C.; Fiorino, G.; et al. Dual Targeted Therapy: A Possible Option for the Management of Refractory Inflammatory Bowel Disease. J. Crohn’s Colitis 2021, 15, 335–339.
- Glassner, K.; Oglat, A.; Duran, A.; Koduru, P.; Perry, C.; Wilhite, A.; Abraham, B.P. The use of combination biological or small molecule therapy in inflammatory bowel disease: A retrospective cohort study. J. Dig. Dis. 2020, 21, 264–271.
- Stone, M.; Morrison, M.; Forster, E. P076 The Role of Dual Biologic Therapy in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2021, 116, S20.
- Goessens, L.; Colombel, J.F.; Outtier, A.; Ferrante, M.; Sabino, J.; Judge, C.; Saeidi, R.; Rabbitt, L.; Armuzzi, A.; Domenech, E.; et al. Safety and efficacy of combining biologics or small molecules for inflammatory bowel disease or immune-mediated inflammatory diseases: A European retrospective observational study. United Eur. Gastroenterol. J. 2021, 9, 1136–1147.
- Kwapisz, L.; Raffals, L.E.; Bruining, D.H.; Pardi, D.S.; Tremaine, W.J.; Kane, S.V.; Papadakis, K.A.; Coelho-Prabhu, N.; Kisiel, J.B.; Heron, V.; et al. Combination Biologic Therapy in Inflammatory Bowel Disease: Experience From a Tertiary Care Center. Clin. Gastroenterol. Hepatol. 2021, 19, 616–617.
- Gniadecki, R.; Bang, B.; Sand, C. Combination of antitumour necrosis factor-α and anti-interleukin-12/23 antibodies in refractory psoriasis and psoriatic arthritis: A long-term case-series observational study. Br. J. Dermatol. 2016, 174, 1145–1146.
- Hamilton, T. Treatment of psoriatic arthritis and recalcitrant skin disease with combination therapy. J. Drugs Dermatol. 2008, 7, 1089–1093.
- Krell, J.M. Use of alefacept and etanercept in 3 patients whose psoriasis failed to respond to etanercept. J. Am. Acad. Dermatol. 2006, 54, 1099–1101.
- Weinblatt, M.; Combe, B.; Covucci, A.; Aranda, R.; Becker, J.C.; Keystone, E. Safety of the selective costimulation modulator abatacept in rheumatoid arthritis patients receiving background biologic and nonbiologic disease-modifying antirheumatic drugs: A one-year randomized, placebo-controlled study. Arthritis Rheum. 2006, 54, 2807–2816.
- Weinblatt, M.; Schiff, M.; Goldman, A.; Kremer, J.; Luggen, M.; Li, T.; Chen, D.; Becker, J.C. Selective costimulation modulation using abatacept in patients with active rheumatoid arthritis while receiving etanercept: A randomised clinical trial. Ann. Rheum. Dis. 2007, 66, 228–234.
- Greenwald, M.W.; Shergy, W.J.; Kaine, J.L.; Sweetser, M.T.; Gilder, K.; Linnik, M.D. Evaluation of the safety of rituximab in combination with a tumor necrosis factor inhibitor and methotrexate in patients with active rheumatoid arthritis: Results from a randomized controlled trial. Arthritis Rheum. 2011, 63, 622–632.
- Van Vollenhoven, R.F.; Wax, S.; Li, Y.; Tak, P.P. Safety and efficacy of atacicept in combination with rituximab for reducing the signs and symptoms of rheumatoid arthritis: A phase II, randomized, double-blind, placebo-controlled pilot trial. Arthritis Rheumatol. 2015, 67, 2828–2836.
- Olbjørn, C.; Rove, J.B.; Jahnsen, J. Combination of Biological Agents in Moderate to Severe Pediatric Inflammatory Bowel Disease: A Case Series and Review of the Literature. Pediatr. Drugs 2020, 22, 409–416.
- Dolinger, M.; Spencer, E.; Lai, J.; Dunkin, D.; Dubinsky, M. Dual biologic and small molecule therapy for the treatment of refractory pediatric inflammatory bowel disease. Inflamm. Bowel Dis. 2021, 27, 1210–1214.