Anxiety, depressive symptoms and stress have a significant influence on chronic musculoskeletal pain. Behavioral modification techniques have proven to be effective to manage these variables; however, the COVID-19 pandemic has highlighted the need for an alternative to face-to-face treatment.
1. Introduction
The COVID-19 pandemic has shaken our lives and jeopardized the treatment of countless patients with chronic pain
[1][2][1,2]. Chronic pain patients have shown a significant increase in their perceived pain in comparison with the pre-pandemic period
[3], as well as an increase in depressive symptoms, anxiety, loneliness, tiredness and catastrophizing
[3]. Nearly half of a sample of 2423 chronic pain patients had moderate to severe psychological distress
[4]. The worsening of mental health in patients with chronic pain is not without consequences; these variables have been linked to higher pain catastrophizing, pain-related fear and avoidance, and a higher risk of misuse of opioids
[5][6][5,6].
These patients need follow-up, a close relationship with health professionals and appropriate treatment, but social distancing prevents them from doing so
[1]. Chronic pain patients had higher self-isolation than participants without pain during the pandemic
[3]. Because it does not require being physically present, telerehabilitation, or the therapeutic use of technological devices, has been recommended for chronic pain management worldwide
[2]. Over the last few decades, behavioral modification techniques (BMT) have showed to be effective in the management of psychological variables in chronic pain patients
[7][8][7,8]. However, it is not clear if telematic BMT (e-BMT) is also effective to improve psychological variables and if it is as effective as in-person BMT. Some previous systematic reviews have assessed the effect of telerehabilitation based on BMT on variables such as pain intensity, disability, disease impact, physical function, pain-related fear of movement, and psychological distress
[9][10][11][12][9,10,11,12], showing promising results.
2. Descriptions of the Studies
From the 749 studies initially detected, a total of 41 RCTs were included
[13][14][15][16][17][18][19][20][21][22][23][24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43][44][45][46][47][48][49][50][51][52][53][41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81].
The PR
esearchISMA 2020 flow chart is detailed in Appendix A.2. We
rs included 5018 participants with a mean age ranging from 33.7 to 65.8 years. The patients were mostly women (N = 3631, 72.4%) diagnosed with chronic back pain
[19][24][44][51][52][47,52,72,79,80], chronic low back pain
[13][27][41,55], unspecific chronic pain
[15][23][25][28][31][39][40][41][42][43][45][46][47][48][53][43,51,53,56,59,67,68,69,70,71,73,74,75,76,81], fibromyalgia
[14][18][20][21][30][35][38][42,46,48,49,58,63,66], headache
[16][32][33][50][44,60,61,78], rheumatic disorders
[17][29][34][36][45,57,62,64], or others
[22][26][37][50,54,65]. Details of the participant’s characteristics and studies are shown in Appendix A.3.
The studies compared online cognitive-behavioral therapy
[14][15][17][18][19][26][27][31][35][42][44][51][52][53][42,43,45,46,47,54,55,59,63,70,72,79,80,81], acceptance and commitment therapy
[28][30][42][43][45][48][56,58,70,71,73,76], self-management
[24][31][34][38][39][40][41][49][52,59,62,66,67,68,69,77], mindfulness therapy
[33][37][42][44][48][61,65,70,72,76], or other e-BMT
[13][16][20][21][22][25][29][32][36][46][47][50][41,44,48,49,50,53,57,60,64,74,75,78], against most frequently waiting list
[15][16][18][20][23][26][28][29][32][34][36][40][43][44][46][47][49][51][52][53][43,44,46,48,51,54,56,57,60,62,64,68,71,72,74,75,77,79,80,81], usual care
[14][17][19][21][24][27][30][31][33][35][38][39][41][42][45][50][42,45,47,49,52,55,58,59,61,63,66,67,69,70,73,78], or in-person intervention
[22][35][48][50,63,76]. The intervention duration ranged between a single day
[37][65] and 6 months
[13][22][34][38][50][41,50,62,66,78]. The details of the interventions
are described in Appendix A.4 using the Behavior Change Technique Taxonomy (v1)
[54][82].
3. Methodological Quality and Risk of Bias
According to the PEDro scale, 30 were evaluated as having good
[13][14][15][16][17][18][19][20][21][22][23][27][28][30][31][34][35][36][37][38][40][42][43][44][45][47][48][49][50][52][41,42,43,44,45,46,47,48,49,50,51,55,56,58,59,62,63,64,65,66,68,70,71,72,73,75,76,77,78,80] and 11 as having fair methodological quality
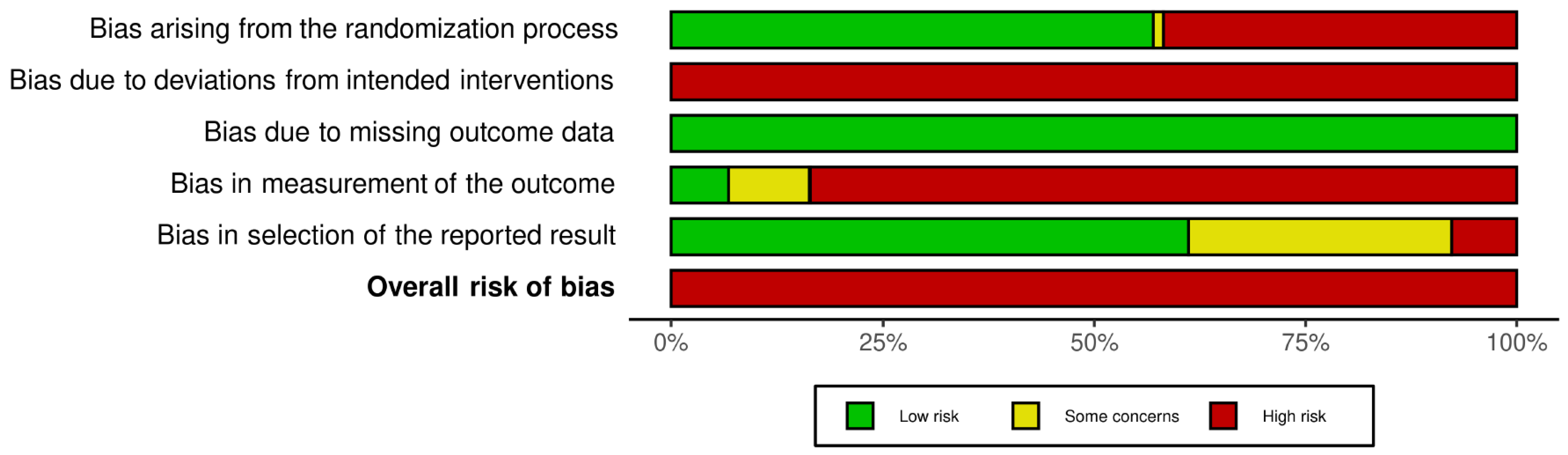
[24][25][26][29][32][33][39][41][46][51][53][52,53,54,57,60,61,67,69,74,79,81] (Appendix A.5). The inter-rater reliability of the methodological quality assessment between assessors was high (κ = 0.823). According to the Rob 2 scale, all the studies have a high risk of bias (100%) (
Figure 1 and Appendix A.6). The inter-rater reliability of the risk of bias assessment between assessors was high (κ = 0.884).
Figure 1. Risk of bias graph according to the Risk of Bias 2 tool.
Risk of bias graph according to the Risk of Bias 2 tool.
4. Qualitative Synthesis
Four studies compared e-BMT with in-person BMT. They applied CBT
[19][35][47,63], ACT
[48][76] or person-centered intervention
[22][50]. Two found non-statistically significant differences between groups for depressive symptoms (n = 253; MD = 0.24, 95% CI −2.32 to 2.80
[19][47] and MD = −0.51, 95% CI −2.42 to 1.40
[48][76]); however, Vallejo et al. found statistically significant between-group differences post-treatment in favor of e-BMT (n = 40; MD = −5.06, 95% CI −7.39 to −2.73)
[35][63]. One found a non-statistically significant difference between groups for anxiety (n = 128; MD = −4.20, 95% CI −10.58 to 2.17)
[48][76] and one found a non-statistically significant difference between groups for stress (n = 109; MD = −2.76, 95% CI −5.94 to 1.28)
[22][50].
5. Quantitative Synthesis
5.1. Depressive Symptoms
According to the influence analyses,
rwe
searchers conducted a sensitivity analysis without Dear et al.
[15][43].
ResearchWe
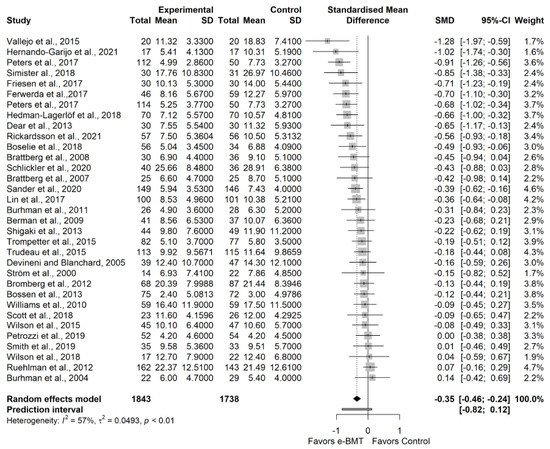
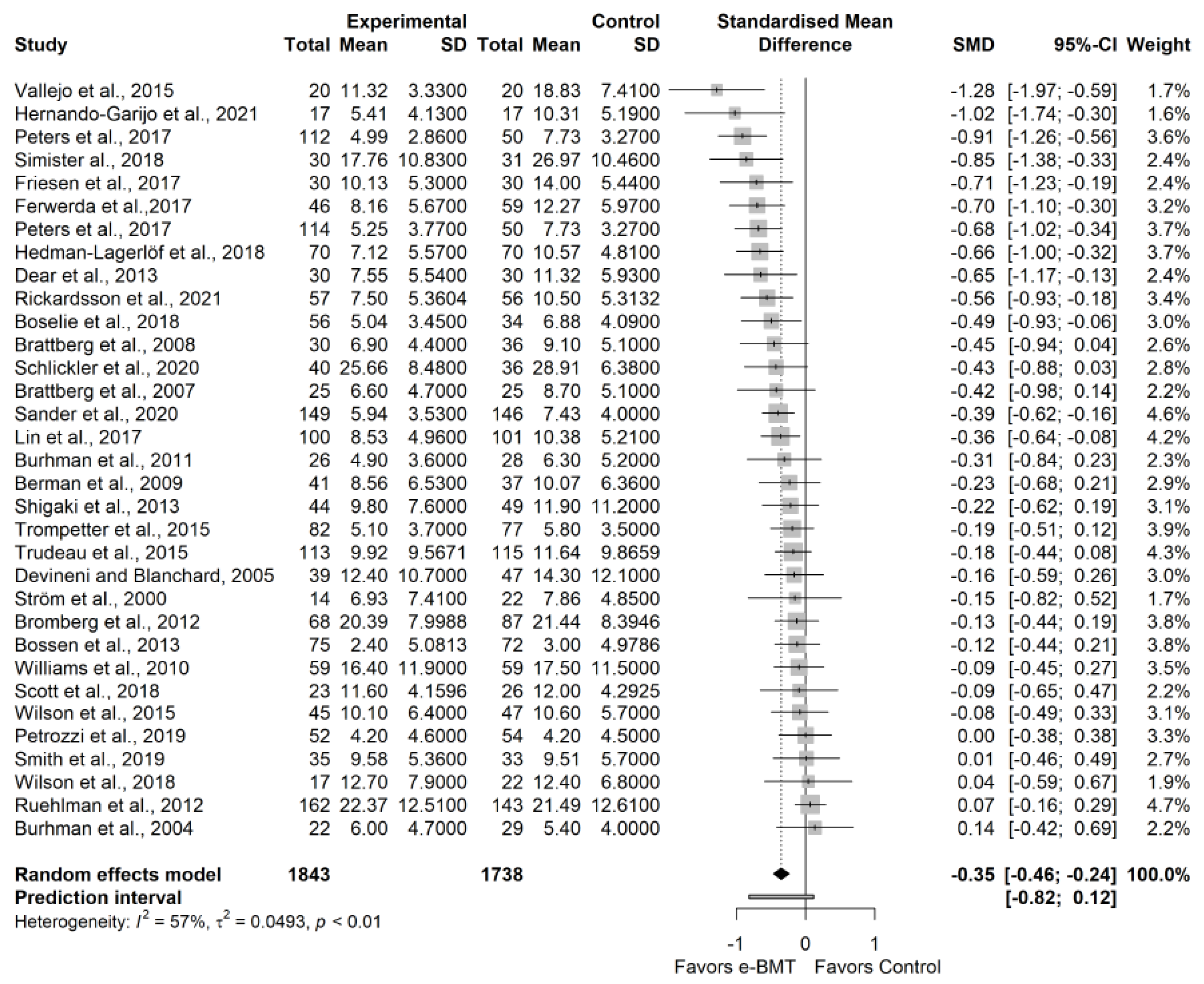
rs found a statistically significant small effect size (32 RCTs; n = 3531; SMD = −0.35; 95% CI −0.46, −0.24) of e-BMT on depressive symptoms compared with usual care or waiting list, with significant heterogeneity (Q = 74.06 (
p < 0.01); I
2 = 57% (36%, 71%); PI −0.82, 0.12) and a low strength of evidence (
Figure 2). Since PI crosses zero,
rwe
searchers cannot be confident that future studies will not find contradictory results; however, the results appear to be robust to different
p-value functions. With respect to the presence of publication bias, the funnel and Doi plots show an asymmetrical pattern, demonstrating minor asymmetry (LFK index = −1.62). When the sensitivity analysis is adjusted for publication bias, there is still a small significant effect. S
tatistical analyses are detailed in Appendix A.7. Subgroup analyses are detailed in
Table 1a.
Figure 2. Sensitivity analysis of the depressive symptoms variable for telematic behavioral modification techniques against usual care or waiting list. Negative results favor the intervention group. The small boxes with the squares represent the point estimate of the effect size and sample size. The lines on either side of the box represent a 95% confidence interval (CI). e-BMT: Telematic Behavioral Modification Techniques.
Table 1.
Subgroup analysis.
| Outcomes Sub = Analysis |
N Studies |
SMD |
Lower Limit 95%CI |
Upper Limit
95% CI |
Q |
I2 |
| (a) Depressive Symptoms—Treatment |
| ACT |
5 |
−0.39 |
−0.71 |
−0.07 |
6.38 |
37% |
| CBT |
11 |
−0.46 |
−0.73 |
−0.19 |
29.21 |
66% |
| Positive Psychology |
2 |
−0.61 |
−1.77 |
0.55 |
0.45 |
0% |
| Self-management |
8 |
−0.12 |
−0.26 |
0.03 |
6.30 |
0% |
| Other types of treatment |
7 |
−0.30 |
−0.58 |
−0.03 |
11.19 |
46% |
| Depressive Symptoms—Chronic Musculoskeletal disorder |
| Back pain |
| Only e-BMT |
| 17 |
| −0.34 |
| −0.45 |
| −0.22 |
| 26.85 |
| 37% |
| e-BMT added to usual care |
| 4 |
| −0.19 |
| −0.59 |
| 0.22 |
4.95 |
39% |
| Anxiety—Methodological Quality according to the PEDro scale |
| Fair methodological quality |
5 |
−0.18 |
−0.40 |
0.04 |
6.61 |
24% |
| Good methodological quality |
16 |
−0.37 |
−0.49 |
−0.24 |
22.28 |
33% |
Abbreviatures: ACT: Acceptance and Commitment therapy; CBT: Cognitive-behavioral therapy; CI: Confidence interval; e-BMT: Telematic behavioral techniques; N/A: Not Applicable; SMD: Standardized mean difference; Y/N: Yes.
5.2. Anxiety
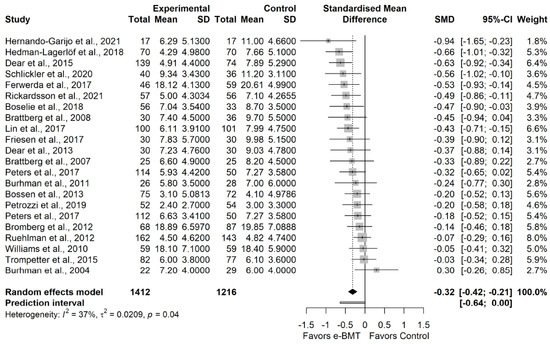
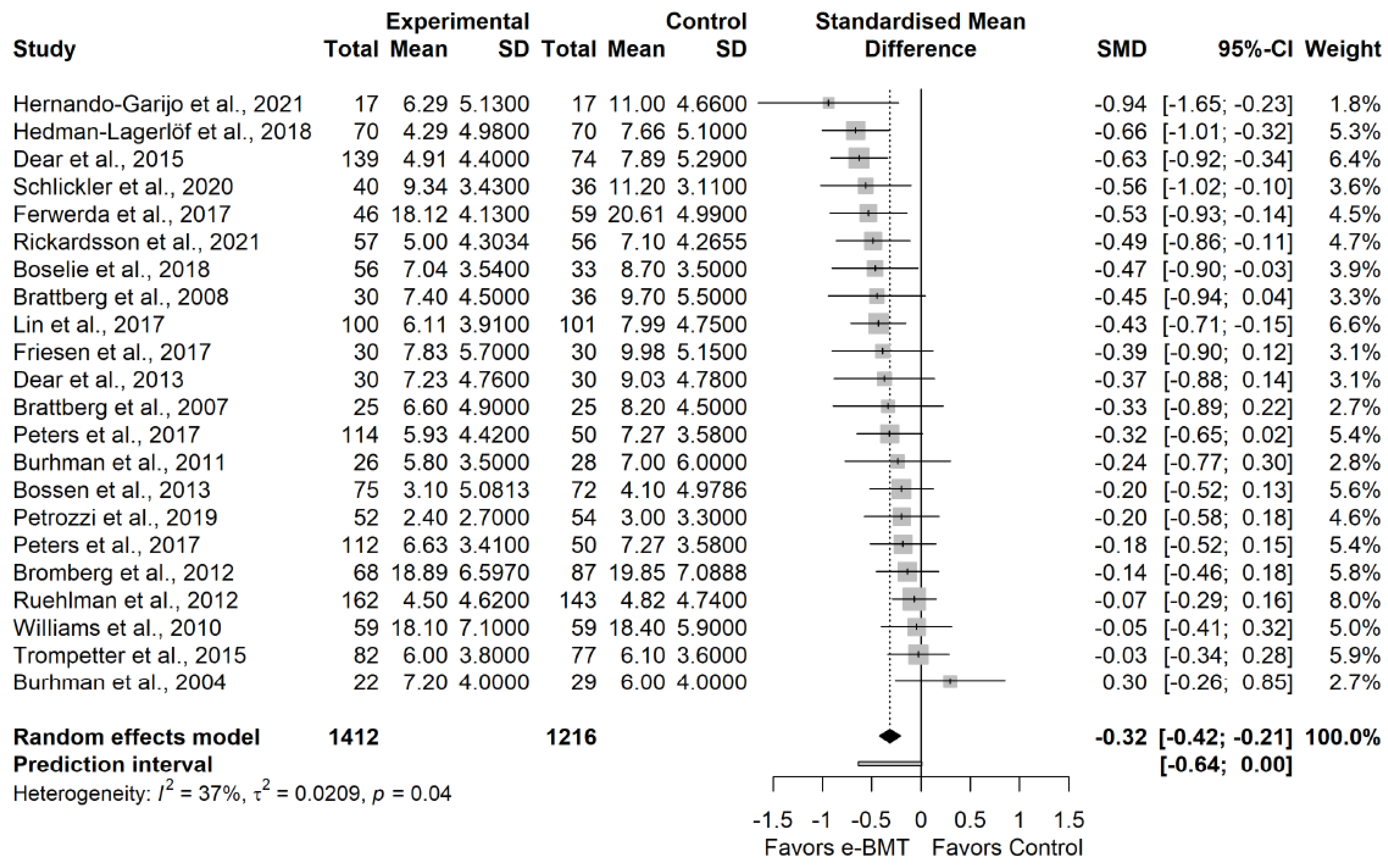
According to the influence analyses, researchers conducted a sensitivity analysis without Trudeau et al. [34]. Researchers found a statistically significant small effect size (21 RCTs; n = 2578; SMD = −0.32; 95% CI −0.42, −0.21) of e-BMT on anxiety compared with usual care or waiting list, with significant heterogeneity (Q = 33.47 (
According to the influence analyses, we conducted a sensitivity analysis without Trudeau et al. [62]. We found a statistically significant small effect size (21 RCTs; n = 2578; SMD = −0.32; 95% CI −0.42, −0.21) of e-BMT on anxiety compared with usual care or waiting list, with significant heterogeneity (Q = 33.47 (p
= 0.04); I2
= 37% (0%, 63%); PI −0.64, 0.00) and a moderate strength of evidence (Figure 3). Since PI crosses zero, researchers cannot be confident that future studies will not find contradictory results; however, the results appear to be robust to different
). Since PI crosses zero, we cannot be confident that future studies will not find contradictory results; however, the results appear to be robust to different p-value functions. With respect to the presence of publication bias, the funnel and Doi plots show a symmetrical pattern, demonstrating no asymmetry (LFK index = −0.48). Subgroup analyses are detailed in
-value functions. With respect to the presence of publication bias, the funnel and Doi plots show a symmetrical pattern, demonstrating no asymmetry (LFK index = −0.48). Statistical analyses are detailed in Appendix A.8. Subgroup analyses are detailed in Table 1b.
b.
Figure 3. Sensitivity analysis of the anxiety variable for telematic behavioral modification techniques against usual care or waiting list. Negative results favor the intervention group. The small boxes with the squares represent the point estimate of the effect size and sample size. The lines on either side of the box represent a 95% confidence interval (CI). e-BMT: Telematic Behavioral Modification Techniques.
5.3. Stress
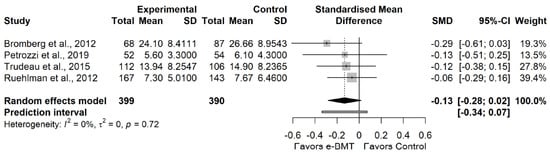
We found no statistically significant effect size (4 RCTs; n = 789; SMD = −0.13; 95% CI −0.28, 0.02) of e-BMT on stress compared with usual care or waiting list, with significant heterogeneity (Q = 1.33 (p
= 0.72); I2
= 0% (0%, 85%); PI −0.34, 0.07) and a moderate strength of evidence (Figure 4). Since PI crosses zero, researchers cannot be confident that future studies will not find contradictory results. With respect to the presence of publication bias, the funnel and Doi plots show an asymmetrical pattern, demonstrating minor asymmetry (LFK index = −1.55). When the sensitivity analysis is adjusted for publication bias, there is no influence on the estimated effect. 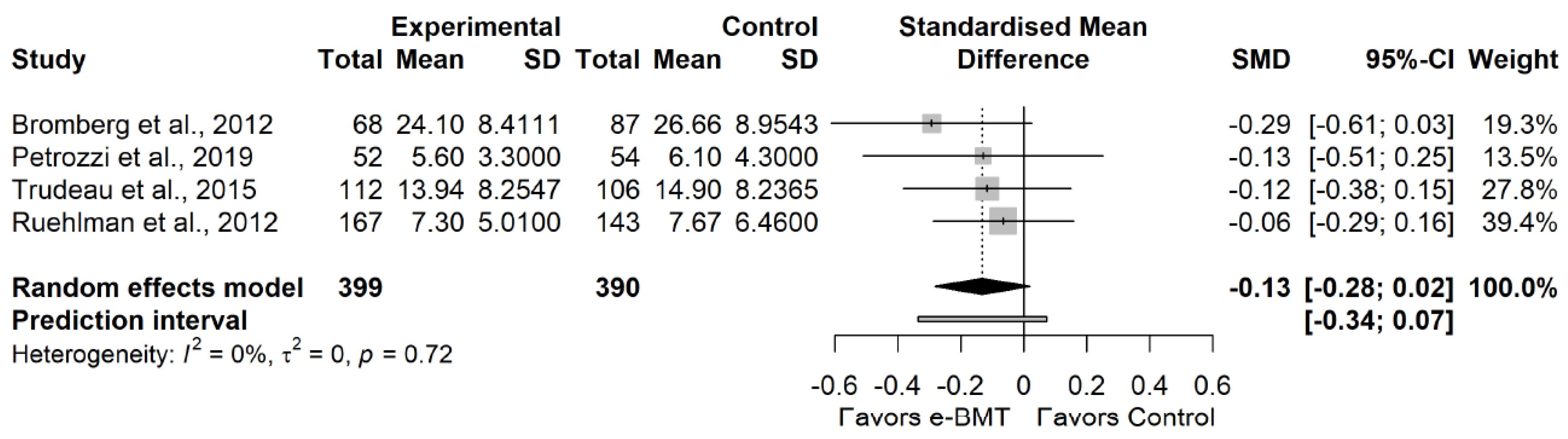
). Since PI crosses zero, we cannot be confident that future studies will not find contradictory results. With respect to the presence of publication bias, the funnel and Doi plots show an asymmetrical pattern, demonstrating minor asymmetry (LFK index = −1.55). When the sensitivity analysis is adjusted for publication bias, there is no influence on the estimated effect. Statistical analyses are detailed in Appendix A.9.
Figure 4. Statistical analysis of the stress variable for telematic behavioral modification techniques against usual care or waiting list. Negative results favor intervention group. The small boxes with the squares represent the point estimate of the effect size and sample size. The lines on either side of the box represent a 95% confidence interval (CI). e-BMT: Telematic Behavioral Modification Techniques.
GRADE’s overall strength of the evidence is detailed in
Table 2.
Table 2.
GRADE’s overall strength of the evidence.
| Certainty Assessment |
|
No. of
Participants |
Effect |
Certainty |
Outcome
(No. of Studies) |
Study
Design |
Risk of Bias |
Inconsistency |
Indirectness |
Imprecision |
Publication Bias |
e-BMT |
Control |
Absolute
(95% CI) |
|
| Depressive symptoms (n = 32) |
RCT |
Serious |
Serious |
Not serious |
Not serious |
Not serious |
1843 |
1688 |
−0.35
(−0.46; −0.24) |
Low
⊕⊕ |
Anxiety
(n = 21) |
RCT |
Serious |
Not Serious |
Not serious |
Not serious |
Not serious |
1412 |
1166 |
−0.32
(−0.42; −0.21) |
Moderate
⊕⊕⊕ |
Stress
(n = 4) |
RCT |
Serious |
Not serious |
Not serious |
Not serious |
Not serious |
399 |
390 |
−0.13
(−0.28; 0.02) |
Moderate
⊕⊕⊕ |
| 5 |
−0.24 |
−0.53 |
0.05 |
5.58 |
28% |
| Fibromyalgia |
7 |
−0.66 |
−1.01 |
−0.31 |
14.16 |
58% |
| Headache |
3 |
−0.14 |
−0.19 |
−0.09 |
0.02 |
0% |
| Rheumatic disorders |
4 |
−0.28 |
−0.68 |
0.12 |
5.85 |
49% |
| Unspecified chronic pain |
13 |
−0.33 |
−0.51 |
−0.15 |
36.61 |
65% |
| Depressive Symptoms—Added to usual care treatment? (Y/N) |
| Only e-BMT |
24 |
−0.34 |
−0.46 |
−0.22 |
52.26 |
54% |
| e-BMT added to usual care |
8 |
−0.41 |
−0.80 |
−0.03 |
21.79 |
68% |
| Depressive Symptoms—Intervention duration |
| Between 1 and 6 weeks |
6 |
−0.02 |
−0.17 |
0.12 |
2.44 |
0% |
| Between 7 and 11 weeks |
18 |
−0.46 |
−0.61 |
−0.31 |
36.70 |
51% |
| 12 weeks and more |
8 |
−0.26 |
−0.50 |
−0.03 |
12.54 |
44% |
| Depressive Symptoms—Methodological Quality according to the PEDro scale |
| Fair methodological quality |
7 |
−0.18 |
−0.43 |
0.07 |
10.86 |
45% |
| Good methodological quality |
25 |
−0.39 |
−0.52 |
−0.26 |
54.08 |
54% |
| (b) Anxiety—Treatment |
| ACT |
3 |
−0.31 |
−0.93 |
0.31 |
4.75 |
58% |
| CBT |
10 |
−0.31 |
−0.50 |
−0.12 |
14.71 |
39% |
| Positive psychology |
2 |
−0.37 |
-1.28 |
0.53 |
0.28 |
0% |
| Self-Management |
3 |
−0.20 |
−0.70 |
0.30 |
2.34 |
15% |
| Other types of treatment |
4 |
−0.41 |
−0.97 |
0.14 |
8.43 |
64% |
| Anxiety—Chronic Musculoskeletal disorder |
| Unspecific back pain |
3 |
−0.09 |
−0.75 |
0.58 |
2.43 |
18% |
| Fibromyalgia |
5 |
−0.45 |
−0.85 |
−0.05 |
8.17 |
51% |
| Headache |
1 |
−0.14 |
−0.85 |
0.18 |
N/A |
N/A |
| Rheumatic disorders |
2 |
−0.35 |
-2.47 |
1.77 |
1.67 |
40% |
| Unspecified chronic pain |
10 |
−0.33 |
−0.47 |
−0.19 |
16.12 |
38% |
| Anxiety—Intervention duration |
| 1 to 6 weeks |
2 |
0.02 |
-1.96 |
2.01 |
1.41 |
29% |
| 7 to 11 weeks |
13 |
−0.41 |
−0.50 |
−0.31 |
10.34 |
0% |
| 12 weeks and more |
6 |
−0.25 |
−0.56 |
0.06 |
9.13 |
45% |
| Anxiety—Added to usual care treatment? (Y/N) |
6. Discussion
The primary aim
of th
ereis systematic review with meta-analysis was to evaluate the effectiveness of e-BMT compared with usual care/waiting list or in-person BMT in terms of psychological variables. Secondly,
researcherswe aimed to sub-analyze the results by intervention parameters and diagnostic conditions. The main results found that e-BMT seems to be an effective option for the management of anxiety and depressive symptoms in patients with musculoskeletal conditions causing chronic pain but not to improve stress symptoms. e-BMT does not seem to provide greater improvement than in-person BMT for psychological variables.
Several research studies have been published and have shown similar results to those found
in herethis review with meta-analysis with regard to depressive and anxiety symptoms. For example, the rapid review conducted by Varker et al.
[55][83] aimed to evaluate the effectiveness of e-BMT (by videoconference) and also through conventional mobile phone calls for people with high levels of anxiety and depression. The main results showed that both rehabilitation modalities produced significant positive results in terms of decreasing the levels of both psychological variables. In addition to this, the re
svie
archw conducted by McCall et al.
[56][84] found that delivering psychological telematic interventions resulted in a significant decrease in depressive symptoms but could not be proven to be effective in comparison to face-to-face psychological intervention. Anxiety symptoms could not be assessed. This work included few studies, so the results have to be interpreted with caution.
In addition to being a possible alternative to in-person treatment, e-BMT appears to be a cost-effective technique compared to in-person BMT. De Boer et al. compared e-BMT and in-person BMT in patients with chronic pain and found that the costs of online CBT were EUR 199 lower than in-person BMT
[57][85]. Similarly, Aspvall et al. found that after 6 months of follow-up in children and adolescents with obsessive compulsive disorder, there was a difference of USD 1688 in favor of e-BMT
[58][86]. Healthcare systems and guidelines should seriously consider implementing e-BMT in the management of patients with musculoskeletal disorders causing chronic pain.