4. Magnetic Resonance Spectroscopy
Nuclear magnetic resonance spectroscopy of protons, referred to as
1H-MRS, has been used since the early 1990s to obtain metabolic information about brain metabolism and detect changes in neurochemistry caused by asphyxia
[50][66]. The magnetic field that a particular proton experiences is influenced by its chemical environment. Differently sited protons will therefore resonate at different frequencies. This so-called chemical shift is used in
1H-MRS to discern different metabolites. There is compelling evidence for the excellent prognostic value of
1H-MRS in newborns with HIE
[51][41][13,14]. NAA and lactate measured in the deep gray matter have been demonstrated to be the most useful biomarkers in the assessment of metabolic changes associated with HIE
[52][15]. The predictive value for an adverse outcome is excellent, and not affected by therapeutic hypothermia
[51][52][13,15]. These metabolites have a long T2 relaxation time and are therefore best detected using a long (>130 ms) echo-time, which improves the signal-to-noise ratio of these metabolites due to the attenuation of signals from metabolites with a shorter time of relaxation.
NAA is found in high concentrations in neurons and has been described as a surrogate biomarker of neuronal integrity and function
[53][67]. Total NAA (tNAA; NAA + N-acetylaspartylglutamate) in the deep gray matter was shown to be significantly lower in newborns with adverse outcomes at 18–22 months of age during the first 2 weeks after birth
[53][67]. In a prospective multicenter cohort study, Lally et al. demonstrated that using
1H-MRS, thalamic NAA concentration alone could accurately predict an adverse neurodevelopmental at 18–24 months of age, with a sensitivity of 100% and specificity of 97%
[41][14]. However, measuring absolute concentrations of metabolites is difficult, as the detection level of NAA falls in the millimolar range and requires internal or external standards. Although water-unsuppressed concentration can be used as an internal standard, this may be unreliable as the amount of intracellular and extracellular brain water may be altered by perinatal asphyxia
[54][69]. Metabolite ratios such as NAA/choline are often used instead and have also been demonstrated to be predictive of outcome in newborns with HIE
[55][70].
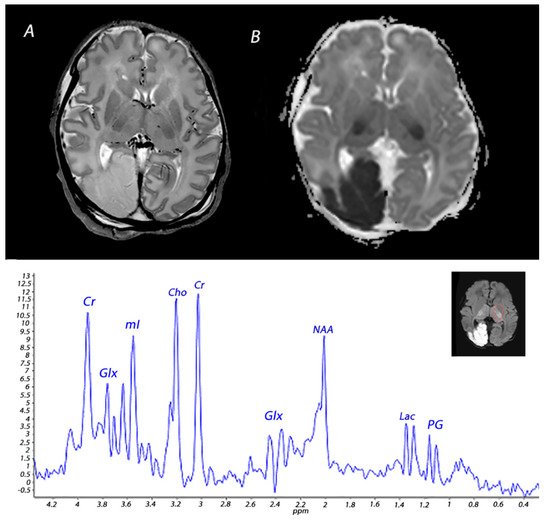
Lactate is a product of anaerobic metabolism, hence increased in hypoxic-ischemic conditions. It has a chemical shift of 1.33 ppm and presents as a doublet peak on spectra obtained with a short echo-time (35–40 ms) or long echo-time (272–288 ms), and an inverted peak with an echo-time around 136–144 ms (
Figure 4). Changes in lactate concentrations due to HIE are often transient; a study analyzing cerebral lactate concentrations in infants with HIE receiving therapeutic hypothermia showed high levels of lactate during hypothermia in infants with moderate-severe HIE, which slightly decreased after cooling and subsequently normalized by the end of the first week after birth
[56][71]. The cerebral lactate remained low in infants with no or mild brain injury during the first 2 weeks after birth. These temporal resolutions are important to take into account when interpreting
1H-MRS findings. Recently, it was demonstrated that during the first 24–96 h after birth tNAA concentration, ADC values, lactate levels, and lactate/tNAA ratios all had high prognostic value in infants with HIE undergoing therapeutic hypothermia, but only tNAA retained its good prognostic value in the second week after birth
[57][72]. Moreover, it is important to consider gestational age when interpreting
1H-MRS spectra. The presence of a lactate peak may be normal in preterm infants, and these infants may show relatively decreased NAA levels compared to term neonates
[58][59][73,74].
In the past, phosphorus MRS (
31P-MRS) was used to study brain energy metabolism in human infants. Although an association between
31P-MRS findings and neurodevelopmental outcomes has been demonstrated in newborns with perinatal asphyxia, it is not routinely performed in the clinical setting
[60][61][75,76].