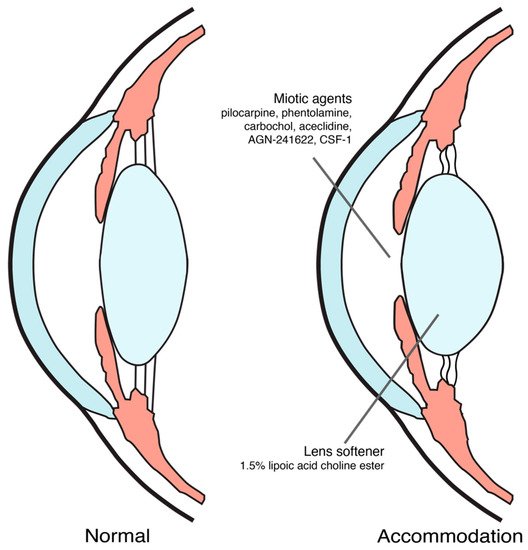
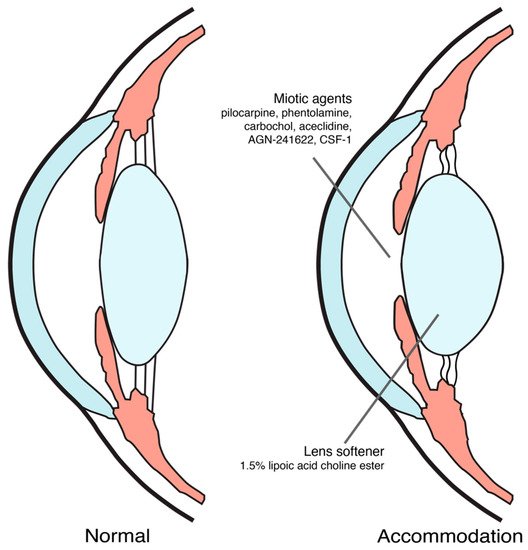
Pharmacological treatment of presbyopia may be an alternative for those who want a spectacle-free scenario and an easy-to-use method with lower risk of irreversible ocular adverse events. There are two main agents, miotics and lens softeners, investigated as agents for the pharmacological treatment. Miotic agents treat presbyopia by creating a pinhole effect which may increase the depth of focus at all working distances. Lens softeners increase the elasticity of the lens, which is targeted at one of the etiologic mechanisms of presbyopia.
1. Introduction
Presbyopia is a physiologically age-related reduction of accommodation leading to unsatisfied clarity of the near vision [1]. This condition usually starts after age of 45. In 2015, it was estimated that approximately 1.8 billion people were affected by presbyopia globally which was about 25% of the world population, and approximately 826 million people lacked proper visual correction. In the year 2030, the number of people with presbyopia is expected to be increasing to 2.1 billion people globally [2].
Accommodation is a mechanism enabling eyes to adjust their refraction power to focus on near objects. There are three main processes involved in accommodation. They are (1) ciliary muscle contraction, which in turn reduces the zonular tension and results in increased lens thickness, (2) pupillary constriction, and (3) convergence of both eyes [3][4]. The widely accepted cause of presbyopia is the stiffening of the lens, which limits lens thickening [5].
Presbyopia does not only affect the near vision, which is the distance between 20 and 40 cm from the eyes, but also affects the intermediate vision, which is the distance between 50 to 100 cm from the eyes [6].
Treatment and correction of presbyopia are still challenging since there are no drugs or procedures that can cause perfect vision at all distances without risk. Currently, there are several options to treat presbyopia: optical correction, including bifocal or progressive spectacles, monofocal or multifocal contact lenses, corneal or intraocular surgical procedures, and pharmacological treatment.
For optical correction with spectacles, such as monofocal, bifocal or multifocal lenses, they are common options because of easy access and non-invasive approach. However, spectacles are perceived by many patients as inconvenient [7][8][9]. Monovision contact lenses may deteriorate stereopsis since the lens is put on only one eye for near tasks. When there is a difference between focusing power of both eyes, the depth discrimination is affected [10]. Monovision associated with anisometropia of +2.00 diopters or higher may decrease stereoacuity [11]. Multifocal contact lenses may be an alternative to spectacles, however, they may cause discomfort, or inconvenience for some patients, particularly those who have never worn contact lens [12]. Contact lenses may also be related with a risk of serious ocular surface infections [13].
Surgical options, corneal or intraocular, are of increasing interest since they are based on most modern technologies. Corneal surgery, such as corneal monovision, corneal inlays, collagen shrinkage, or multifocal LASIK, was one of the common methods for presbyopia correction. They have shown successes in improving near vision, however, there are disadvantages, such as, reduction of intermediate or distance vision, decreased contrast sensitivity, dysphotopsia, or refractive regression. Due to these, some patients still need spectacles after the procedures [1][14]. Intraocular lenses (IOLs), such as monovision IOLs or multifocal IOLs, were also used for correction of presbyopia, with disadvantages, such as, dysphotopsia, or poorer intermediate vision, similar to corneal surgeries [14][15].
There are still risks of surgical complications, which are hardly reversible, and the best results are based on careful selection of patients. Moreover, good understanding of the limitation of the present technologies by patients and their trade-off nature are very important, for example, patients who gain spectacle-free of near or intermediate vision may experience some dysphotopsias in different lighting conditions or lose some sharpness of vision or stereopsis depending on the offered technology [16]. Finally, none of the present surgical technologies can offer full spectacles independence for the whole time of all activities.
Pharmacological treatment of presbyopia has been studied in recent years based on different drugs and different treatment regimens. Pharmacological treatment, in theory, may offer a benefit of having a spectacle-free condition with a lower risk of irreversible ocular complications, compared to surgery. In November 2021, U.S. FDA has approved 1.25% pilocarpine hydrochloride ophthalmic solution (AGN-190584) as an eye drop for treating presbyopia [17]. This is the first eye drop treatment of presbyopia that obtained U.S. FDA approval. It is possible that this approval may cause more interest in research on pharmacological treatment for presbyopia. On the other hand, there will be more data on efficacy and safety of the drug from the real-world experience, which may lead to better understanding of presbyopia.
2. Pharmacological Treatment in Presbyopia
Presbyopia is a physiologically age-related reduction of accommodation leading to unsatisfied clarity of the near vision [1]. This condition usually starts after age of 45. In 2015, it was estimated that approximately 1.8 billion people were affected by presbyopia globally which was about 25% of the world population, and approximately 826 million people lacked proper visual correction. In the year 2030, the number of people with presbyopia is expected to be increasing to 2.1 billion people globally [2].
Accommodation is a mechanism enabling eyes to adjust their refraction power to focus on near objects. There are three main processes involved in accommodation. They are (1) ciliary muscle contraction, which in turn reduces the zonular tension and results in increased lens thickness, (2) pupillary constriction, and (3) convergence of both eyes [3,4]. The widely accepted cause of presbyopia is the stiffening of the lens, which limits lens thickening [5].
Presbyopia does not only affect the near vision, which is the distance between 20 and 40 cm from the eyes, but also affects the intermediate vision, which is the distance between 50 to 100 cm from the eyes [6].
Treatment and correction of presbyopia are still challenging since there are no drugs or procedures that can cause perfect vision at all distances without risk. Currently, there are several options to treat presbyopia: optical correction, including bifocal or progressive spectacles, monofocal or multifocal contact lenses, corneal or intraocular surgical procedures, and pharmacological treatment.
For optical correction with spectacles, such as monofocal, bifocal or multifocal lenses, they are common options because of easy access and non-invasive approach. However, spectacles are perceived by many patients as inconvenient [7,8,9]. Monovision contact lenses may deteriorate stereopsis since the lens is put on only one eye for near tasks. When there is a difference between focusing power of both eyes, the depth discrimination is affected [10]. Monovision associated with anisometropia of +2.00 diopters or higher may decrease stereoacuity [11]. Multifocal contact lenses may be an alternative to spectacles, however, they may cause discomfort, or inconvenience for some patients, particularly those who have never worn contact lens [12]. Contact lenses may also be related with a risk of serious ocular surface infections [13].
Surgical options, corneal or intraocular, are of increasing interest since they are based on most modern technologies. Corneal surgery, such as corneal monovision, corneal inlays, collagen shrinkage, or multifocal LASIK, was one of the common methods for presbyopia correction. They have shown successes in improving near vision, however, there are disadvantages, such as, reduction of intermediate or distance vision, decreased contrast sensitivity, dysphotopsia, or refractive regression. Due to these, some patients still need spectacles after the procedures [1,14]. Intraocular lenses (IOLs), such as monovision IOLs or multifocal IOLs, were also used for correction of presbyopia, with disadvantages, such as, dysphotopsia, or poorer intermediate vision, similar to corneal surgeries [14,15].
There are still risks of surgical complications, which are hardly reversible, and the best results are based on careful selection of patients. Moreover, good understanding of the limitation of the present technologies by patients and their trade-off nature are very important, for example, patients who gain spectacle-free of near or intermediate vision may experience some dysphotopsias in different lighting conditions or lose some sharpness of vision or stereopsis depending on the offered technology [16]. Finally, none of the present surgical technologies can offer full spectacles independence for the whole time of all activities.
Pharmacological treatment of presbyopia has been studied in recent years based on different drugs and different treatment regimens. Pharmacological treatment, in theory, may offer a benefit of having a spectacle-free condition with a lower risk of irreversible ocular complications, compared to surgery. In November 2021, U.S. FDA has approved 1.25% pilocarpine hydrochloride ophthalmic solution (AGN-190584) as an eye drop for treating presbyopia [17]. This is the first eye drop treatment of presbyopia that obtained U.S. FDA approval. It is possible that this approval may cause more interest in research on pharmacological treatment for presbyopia. On the other hand, there will be more data on efficacy and safety of the drug from the real-world experience, which may lead to better understanding of presbyopia.
2. Pharmacological Treatment in Presbyopia
Until now, proposed mechanisms of action for pharmacological treatment of presbyopia were inducing miosis and softening the lens [9][18][19][9,18,19], as shown in Figure 1. The ongoing trials on pharmacological treatment of presbyopia were summarized in Table 1.
Pharmacological treatment for presbyopia mechanism of action.
Ongoing studies on pharmacological treatment for presbyopia from clinicaltrials.gov (at the time of writing).
| Drugs |
N |
Study Design |
Instillation Method |
Primary Outcome |
NCT ID |
Phase |
| |
Miotic agents |
|
| 1.25% pilocarpine [20] |
230 |
Multi-center, double-masked, randomized, vehicle-controlled, parallel-group study |
Twice daily binocularly for 14 days |
Percentage of participants gaining 3 lines or more in mesopic, high contrast, binocular DCNVA at day 14 |
NCT04983589 |
3 |
| 1.25% pilocarpine [21] |
54 |
Randomized, double-masked, crossover study |
Twice daily binocularly for 14 days |
Overall Composite Driving Z score approximately 1 h after study intervention instillation |
NCT04837482 |
3 |
| AGN-241622 [22] |
144 |
Phase 1/2, dose-ascending, multi-center, randomized, double-masked, vehicle-controlled study |
Single drop binocularly |
Number of patients experiencing a treatment emergent adverse event after single administration of AGN-241622 at day 2 and day 14 |
NCT04403763 |
1/2 |
| CSF-1 [23] |
300 |
4-visit, multi-center, randomized, double-masked, vehicle-controlled study |
Twice daily binocularly for 2 weeks |
Percentage of subjects with a ≥ 3-line gain in BDCVA at 40 cm and no loss in BDCVA ≥ 5 letters at 4 m at day 8 |
NCT04599933 |
3 |
| CSF-1 [24] |
300 |
4-visit, multi-center, randomized, double-masked, vehicle-controlled study |
Twice daily binocularly for 2 weeks |
Percentage of subjects with a ≥ 3-line gain in BDCVA at 40 cm and no loss in BDCVA ≥ 5 letters at 4 m at day 8 |
NCT04599972 |
3 |
| 1% phentolamine [25] |
150 |
Randomized, quadruple-masked, parallel-group study |
Single drop binocularly |
Percentage of subjects with ≥15 letters of improvement in photopic binocular DCNVA after 6 h |
NCT04675151 |
2 |
| Carbachol and brimonidine [26] |
450 |
Multi-center, randomized, double-masked study |
Single drop binocularly |
Percentage of subjects with 3-line gains in near VA with the loss of at least 1 line in DVA |
NCT05135286 |
3 |
| PBOHB compound [27] |
11 |
Single group study |
Single drop binocularly |
Jaeger near uncorrected visual acuity improvement after 1 h |
NCT05006911 |
1 |
| Pilocarpine cream [28] |
120 |
Multi-center, randomized, double-masked, placebo-controlled, parallel group study |
Once daily binocularly for 28 days |
Binocular DCNVA after 28 days |
NCT05124275 |
2 |
| Pilocarpine Spray [29] |
139 |
Randomized, triple-masked, crossover, placebo-controlled study |
Single drop binocularly |
Proportion of subjects gaining ≥ 15 letters in mesopic, high contrast, binocular DCNVA at 120 min post-treatment |
NCT05114486 |
3 |
| |
Lens softeners |
|
| 1.5% lipoic acid choline ester [30] |
225 |
Multi-center, randomized, placebo-controlled, double-masked, dose-ranging study |
Twice daily binocularly |
Change in Binocular DNCVA From Baseline at Month 3 |
NCT04806503 |
2 |
Abbreviation: BDCVA—Best-distance corrected visual acuity, DCNVA—Distance corrected near visual acuity, DVA—Distance visual acuity, PBOHB—pilocarpine, brimonidine, oxymetazoline, hyaluronic acid and bromfenac.
2.1. Miotic Agents
Most of the current presbyopia pharmacological treatment options aim at inducing temporary miosis causing a pinhole effect to increase the depth of focus through parasympathetic pathway.
Miotic agents were used as either a monotherapy or in combination therapy with another miotic agent or other agents for treatment of presbyopia. Whereas most of them were used in combination therapy, the only two agents studied for monotherapy were pilocarpine and phentolamine.
2.1.1. Pilocarpine HCl Ophthalmic Solution 1.25%—The U.S. FDA Approved Agent for Presbyopia
Pilocarpine is a miotic agent that has been used and studied in different concentrations, different forms and also as a combination with other drugs for presbyopia. It can induce miosis and ciliary body contraction which would also help in lens accommodation [31].
The daily use of pilocarpine hydrochloride ophthalmic solution 1.25% monotherapy in both eyes is the regimen which has been approved by the U.S. FDA. Pilocarpine ophthalmic solution was stored at a pH between 3.5 to 5.5 for its stability, the agent would have low bioavailability at this acidity. However, it was claimed that pilocarpine HCl ophthalmic solution 1.25% for the treatment of presbyopia could adapt to the pH of ocular surface within 1 min [32].
In phase 3 studies of this agent (GEMINI 1 and GEMINI 2), which were submitted for this approval, the eye drop was applied in each eye daily for 30 days and compared with placebo [33][34]. The key inclusion criteria of these studies were patients with presbyopia aged 40–55 years old, distance-corrected near visual acuity (DCNVA) between 20/40 to 20/100 and best distance correction between −4.00 to +1.00 D sphere and between −2.00 to +2.00 D cylinder. Participants were randomized into the treatment group (n = 375) and placebo group (n = 375). The mean age of participants was 49.6 ± 3.75 and 49.8 ± 3.38 in the treatment group and placebo group, respectively, and the majority of participants (85%) was Caucasian [35].
Since presbyopia affects both near and intermediate vision, outcome measures of both studies included four outcomes for near vision and one for intermediate vision. All of these outcomes were determined at different hours post-instillation on the 30th day of continuous use, therefore in the following sentences, ‘hours’ means hour post-instillation on the 30th day of continuous use. The outcomes for near vision were (1) the primary outcome, a percentage of participants with at least 3-line improvement in mesopic, high-contrast, binocular DCNVA without losing more than 5 letters of mesopic, high contrast, binocular corrected-distance visual acuity (CDVA) at 3 h, (2) a percentage of participants with at least 3-line improvement in mesopic, high-contrast, binocular DCNVA from 0.25 to 8 h, (3) changes from baseline in mesopic DCNVA from 0.25 to 10 h, and (4) a percentage of participants achieving photopic, binocular DCNVA of 20/40 or better at 1 h and 3 h. The outcome for intermediate vision was changes from baseline in photopic, high-contrast, binocular distance-corrected intermediate visual acuity (DCIVA) at 1 h and 3 h [33][34][35].
2.1.2. Other Miotic Agents
Another form of pilocarpine topical drug as ophthalmic cream monotherapy for presbyopia has also been studied. There is an ongoing phase 2 study on various concentrations of this pilocarpine ophthalmic topical cream on their safety and efficacy after using the medication twice a day for 28 days and assessing DCNVA as the primary outcome [28].
A phase 3 study on a 2% pilocarpine ophthalmic solution spray, another alternative mode of delivery, has been conducted with the primary outcome measures as DCNVA at 120 min after instillation [29].
Phentolamine is a nonselective alpha-adrenergic antagonist that has been studied for monotherapy. An ophthalmic solution of 1% phentolamine mesylate could decrease pupil diameter and create pinhole effect. The results from a phase 2b study by Pepose et al., using this drug once daily in the evening for 14 days, compared with placebo, showed that patients in the treatment group had at least 1-line improvement in DCNVA at day 15. There was no difference in conjunctival hyperemia between both treatment and placebo groups [36].
For the combination of a miotic agent with another miotic agent or other agents, the aim is either to gain addition effect between each drug or to reduce the side effects from the miotic agent.
There are several studies evaluating pilocarpine in combination with anti-inflammatory agents or vasoconstrictive agents to minimize adverse events of conjunctival injection or ocular inflammation that may be induced by pilocarpine. An ongoing randomized controlled study has been initiated to compare between monotherapy of miotic agents and the combination of two miotic agents. There were four treatment groups for the comparison in this study: phentolamine and pilocarpine, phentolamine alone, pilocarpine alone and placebo, DCNVA in these treatment groups were compared at baseline and at 6 h [25].
2.2. Lens Softeners
Loss of lens elasticity is associated with advanced age and presbyopia. This may be related to an increase in disulfide bonds formation in the collagen of aging lens, possibly due to oxidative stress [37]. Inducing miosis might be an effective mechanism for treatment of presbyopia by creating a pinhole effect but it might not address the etiology of this condition. Lens softening, on the other hand, might be an agent that could make a change at its pathophysiology.
There was in vitro evidence showing that lipoic acid, an antioxidant, could reduce disulfide bonds in the lens protein, and thus increase lens elasticity [37]. However, lipoic acid alone as an eye drop had limited ocular penetration because of its lipid solubility [38]. Bonding lipoic acid with choline allows the drug to better penetrate into the aqueous humor [39].
In a study by Korenfeld et al., 1.5% lipoic acid choline ester ophthalmic solution (UNR844) was compared with placebo for DCNVA and adverse events. The inclusion criteria were patients with presbyopia aged 45–55 years, monocular DCNVA worse than 20/40 in each eye, best-corrected distance visual acuity of 20/20 or better, and manifested spherical equivalent between −4.00 to +4.00 D. From a total of 75 patients enrolled, they were randomized into the treatment group and the placebo group with 2:1 ratio, resulting in 50 patients in the former and 25 patients in the latter. The mean age of the treatment group and the placebo group was 50.1 ± 3.2 and 51.4 ± 3.0, respectively; 70.67% of patients were Caucasians [39].
The treatment group were given 1.5% lipoic acid choline ester ophthalmic solution unilaterally in their nondominant eye twice daily on day 1–7, and then given bilaterally twice daily on day 8–91. There was significantly improved in DCNVA from baseline in the treatment group compared with the placebo group over the course of 91 days (0.198 vs. 0.099 LogMAR VA units). Moreover, about a third of the patients with 1.5% lipoic acid had a sustained bilateral improvement of at least 1-line DCNVA at day 301. In terms of adverse events, the most common was eye irritation at 6%. Patients also reported asthenopia, eye pruritus, and foreign body sensation. For ocular safety, there were no clinical changes in non-dilated pupil diameter, ocular comfort, intraocular pressure (IOP), distance vision, or other ocular findings in the treated eyes [39].
3. Conclusions
With the recent U.S. FDA approval of 1.25% pilocarpine for treatment of presbyopia, this agent is becoming an alternative option for those in the US who may not want to wear spectacles for near tasks. It is possible that this agent may be approved in other countries and more patients may be able to access this agent in the future. This would give an opportunity to investigate on safety and efficacy of this agent in the real world, particularly for long-term use, which is essential.
Pharmacological treatment of presbyopia is, without a doubt, one of the promising fields in research in ophthalmology since all people who are more than 45 years old will have this condition eventually.