Acute myeloid leukemia (AML) is a disease characterized by uncontrolled proliferation of clonal myeloid blast cells that are incapable of maturation to leukocytes. AML is the most common leukemia in adults and remains a highly fatal disease with a five-year survival rate of 24%. More than 50% of AML patients have mutations in the FLT3 gene, rendering FLT3 an attractive target for small-molecule inhibition. Currently, there are several FLT3 inhibitors in the clinic, and others remain in clinical trials. However, these inhibitors face challenges due to lack of efficacy against several FLT3 mutants. Therefore, the identification of biomarkers is vital to stratify AML patients and target AML patient population with a particular FLT3 mutation.
1. Introduction
Acute myeloid leukemia (AML) is a hematological malignancy that accounts for the most common leukemia that occurs in adults. In the US, there were 20,240 cases and 11,400 deaths due to AML in 2021. The five-year relative survival rate for AML patients is 29.5%
[1]. The incidence of AML increases with age, whereby there are 1.3 cases per 100,000 of the population who are under 65 years old, whereas there are 12.2 cases per 100,000 of the population who are 65 years old and above
[2]. Several treatment options have improved the survival of younger patients, but the mortality remains high for elderly patients
[2][3][2,3].
The human flt3 (FMS-like tyrosine kinase 3) gene is located on chromosome 13q12 and has 24 exons
[4][6]. It encodes a membrane-bound glycosylated protein with a molecular weight of 160 kDa, along with a non-glycosylated isoform which is 143 kDa and not associated with the plasma membrane
[5][7]. FLT3 is a transmembrane protein that encodes for proto-oncogene FLT3. It is a member of the class III receptor tyrosine kinase family and plays an important role in the regulation of the hematopoiesis
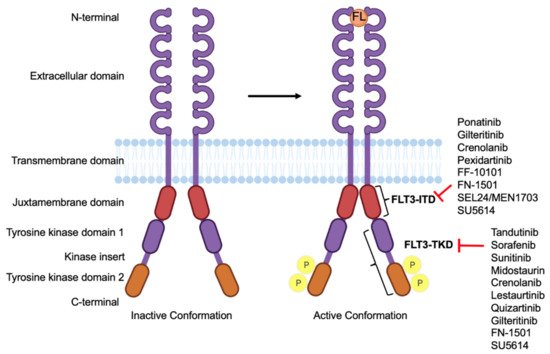
[6][8]. The structure of FLT3 consists of four regions: (i) an N-terminal, extracellular region consisting of five immunoglobulin domains involved in ligand binding; the proximal domain is involved in receptor dimerization, (ii) a transmembrane domain, (iii) a juxta membrane domain (JM), and (iv) an intracellular, C-terminal region with a split-kinase domain. The two substructures of this domain are called N-lobe and C-lobe, which are connected by an inter-kinase domain. These lobes consist of a TKD and are also indicated as the first tyrosine kinase (TK1) and second tyrosine kinase (TK2) domain, respectively
[7][9] (
Figure 1).
Figure 1. Structure of FLT3 and its drug targets. The structure of FLT3 in its inactive conformation which, upon binding to FLT3 ligand (FL), becomes active, resulting in its autophosphorylation. Different FLT3 inhibitors and their binding sites on their domains.
2. Biomarkers for FLT3 Inhibition in AML
A biomarker is a characteristic that is a measurable indicator of a biological process or response to an intervention. Molecular biomarkers are valuable in providing information about the biological behavior of the AML. These biomarkers can be classified into various categories, including diagnostic, predictive, prognostic, and pharmacodynamic biomarkers, based on their putative applications
[8][14].
Diagnostic biomarkers are used to confirm the presence of a disease and aid in the identification of individuals with a disease subtype. These biomarkers are used to identify people with a disease
[8][14]. For example, in the case of AML, gene rearrangements, gene fusions, and chromosomal translocations are used in the diagnosis
[9][15].
Predictive biomarkers are used to identify the likelihood of response or lack of response to a particular therapy. These biomarkers help in the identification of patients most likely to benefit from a given treatment and spare other patients from the toxicities of ineffective therapies
[8][14]. NPM1 mutations and the FLT3-ITD allelic ratio (AR) are candidate predictive biomarkers in FLT3 AML
[10][16].
Prognostic biomarkers are used to identify the likelihood of a clinical event, disease recurrence, or progression in patients who have the disease
[8][14]. Mutations in the FLT3 gene, such as FLT3-ITD, confer a poor prognosis in AML patients
[11]. Pharmacodynamic biomarkers depict the biological response to a medical product or environmental agent in an individual. Such biomarkers are useful for clinical practice and therapeutic development
[8][14]. Various molecular markers, such as phosphorylation, and immune markers have been used in various studies
[12][13][17,18].
All these biomarkers are important because of their high clinical importance, and their expression can reveal the disease evolution in real time
[14][19]. So far, several biomarkers have been identified by various studies and clinical trials of FLT3 inhibitors, which are discussed in the sections below.
3. Diagnostic Biomarkers
Various diagnostics have been developed for detecting AML, including morphological, immunophenotyping, and gene fusion screening
[15][20]. For morphological diagnostics, bone marrow smears are examined for myeloblasts, monoblasts, and megakaryoblasts in the blast cells using Wright-Giemsa stains. Immunophenotyping using flow cytometry is used to determine the lineage of leukemia cells
[16][21]. In AML patients, leukemic cells express early, hematopoiesis-associated antigens (CD34, CD38, CD117, HLA-DR) and lack markers of myeloid and monocytic maturation (NSE, CD11c, CD14, CD64)
[9][17][18][19][15,22,23,24]. Similarly, cytogenetic abnormality can be detected in 50% to 60% of newly diagnosed AML patients. The majority of AML patients have nonrandom chromosomal translocations that often lead to gene rearrangements.
[20][21][22][25,26,27]. The World Health Organization (WHO) recognizes recurrent translocations and inversions in AML
[23][24][28,29] (
Table 1). Gene rearrangements, gene fusions, and loss of chromosomes are detected using fluorescence in situ hybridization (FISH) and reverse transcriptase–polymerase chain reaction (RT-PCR)
[25][26][30,31]. These include gene fusions in RUNX1-RUNX1T1 (runt-related transcription factor 1), CBFB-MYH11 (core-binding factor subunit beta–myosin heavy chain 11), acute promyelocytic leukemia (APL) with PML-RARA (promyelocytic leukemia/retinoic acid receptor alpha), MLLT3-KMT2A (mixed-lineage leukemia translocated to chromosome 3- lysine methyltransferase 2A), DEK-NUP214 (DEK oncogene–nucleoporin 214), and an inversion that repositions a distal GATA2 enhancer to activate MECOM expression. BCR-ABL1 is added to recognize that these cases may benefit from tyrosine kinase inhibitor therapy
[23][24][27][28][28,29,32,33]. Finally, for AML diagnosis, testing for mutations in three genes—FLT3, NPM1 (nucleophosmin 1), and CEBPA (CCAAT/enhancer binding protein (C/EBP) alpha)—is recommended
[29][30][31][34,35,36]. Additional genes with varying gene mutation frequency in AML patients include mixed-lineage leukemia (MLL), neuroblastoma RAS (NRAS), Wilms’ tumor type 1 (WT1), v-KIT, runt-related transcription factor (RUNX1), and iso-citrate dehydrogenase (IDH1)
[32][33][34][35][36][37][37,38,39,40,41,42].
Table 1.
Acute myeloid leukemia and acute leukemias of ambiguous lineage (WHO, 2017).
|
| WHO Classification of Acute Myeloid Leukemia with Recurrent Genetic Abnormalities |
|
|
| AML with recurrent genetic abnormalities |
|
|
| AML with t(8;21)(q22;q22.1); RUNX1-RUNX1T1 |
|
|
| AML with inv(16)(p13.1q22) or t(16;16)(p13.1;q22); CBFB-MYH11 |
|
|
| APL with PML-RARA |
|
|
| AML with t(9;11)(p21.3;q23.3); MLLT3-KMT2A |
|
|
| AML with t(6;9)(p23;q34.1); DEK-NUP214 |
|
|
| AML with inv(3)(q21.3q26.2) or t(3;3)(q21.3;q26.2); GATA2, MECOM |
|
|
| AML (megakaryoblastic) with t(1;22)(p13.3;q13.3); RBM15-MKL1 |
|
|
| Provisional entity: AML with BCR-ABL1 |
|
|
| AML with mutated NPM1 |
|
|
| AML with biallelic mutations of CEBPA |
|
|
| Provisional entity: AML with mutated RUNX1 |
|
Interestingly, recent studies indicated that circulating micro RNAs (miRNAs) can be utilized as diagnostic biomarkers for AML. A study identified six serum miRNAs (miR-10a-5p, miR-93-5p, miR-129-5p, miR-155-5p, miR-181b-5p, and miR-320d) which were specifically upregulated in the serum of AML patients using a next-generation sequencing approach
[38][39][43,44].
Four miRNAs (let-7b, miR-128a, miR-128b, and miR-223) were used for the diagnosis of AML with 97% accuracy and analyzed using RT-PCR. miR-142-3p and miR-29a can also be used as diagnostic biomarkers for AML
[40][45]. Interestingly, miR-424 was downregulated in AML patients with NPM1 mutation regardless of FLT3 mutation, whereas miR-155 was upregulated in patients with FLT3-ITD regardless of the NPM1 mutation
[41][46].
These studies suggest that miRNAs from serum or blood samples can be effective diagnostic biomarkers for AML patients.
4. Predictive Biomarkers
There have been multiple FLT3 inhibitors in clinical trials, but predictive biomarkers remain undiscovered. In a recent study aimed at identifying gene expression changes associated with FLT3 mutation in AML patients, the transcriptomic patterns of six different cohorts of AML patients were analyzed, and a FLT3-mutation-like pattern was highly enriched in NPM1 and DNMT3A mutants. In addition, FLT3-like patterns consisted of numerous homeobox (HOX) genes
[42][47].
Based on the FLT3 mutations, companion diagnostics were generated that tested for a predictive biomarker
[43][48]. These tests classified patients into responders and non-responders and directly equated them to the administration of a drug
[44][49].
One such FDA-approved companion diagnostic test was the LeukoStrat CDx FLT3 mutation assay. This is a PCR-based, in vitro diagnostic test that detects ITD and TKD mutations D835 and I836 from the genomic DNA extracted from the mononuclear cells from peripheral blood or bone marrow aspirates of AML-diagnosed patients
[45][50].
This test was used with FLT3 inhibitors, including midostaurin, gilteritinib, and quizartinib
[46][51].
Similarly, co-occurrence of mutations in FLT3 with national comprehensive cancer network (NCCN)-listed gene mutations were used as predictive biomarkers
[47][48][52,53]. Co-occurrence of mutations in monoallelic, CCAAT/enhancer-binding protein alpha (moCEBPA) with FLT3-ITD/TKD led to a poor prognosis. Mutations in NPM1, DNMT3A, and FLT3-ITD were identified at higher rates in patients with intermediate-risk cytogenetics
[49][50][54,55]. It was seen that a group of AML patients with FLT3 plus NPM1 and/or DNMT3A mutations shared a similar transcriptomic background
[42][47]. The revised 2017 WHO classification has myeloid neoplasms with germline mutations in RUNX1, CEBPA, DDX41 (DEAD-box helicase 41), RUNX1, GATA2 (GATA binding protein 2), ETV6 (ETS variant transcription factor 6), SRP72 (signal recognition particle 72), and ANKRD26 (ankyrin repeat domain 26) as markers of AML predisposition
[24][51][52][29,56,57].
Another study identified that the response to gilteritinib and crenolanib among relapsed FLT3
mut AML patients is higher in patients with mutations in NPM1 or DNMT3A and particularly in those with both genes mutated
[53][54][58,59]. When FLT3-ITD leukemias with mutations in NPM1 or DNMT3A are treated with quizartinib, the cell differentiation effect predominates over the cytotoxic mechanism
[55][60]. Additionally, a long non-coding RNA (lnc RNA) expression profile using RNA-seq identified that lncRNA RP11-342 M1.7, lncRNA CES1P1, and lncRNA AC008753.6 serve as predictive biomarkers for AML risk
[56][61].
5. Prognostic Biomarkers
FLT3 is widely overexpressed and the most frequently mutated gene in both pediatric and adult patients with AML
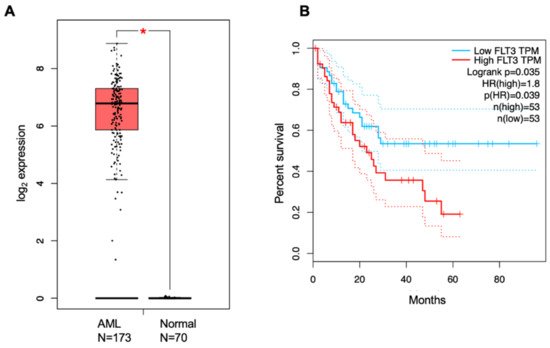
[57][62]. Higher expression of FLT3 results in poor overall survival (OS) in AML patients, as seen in the cancer genome atlas (TCGA) dataset analyzed by GEPIA. The hazard ratio is 1.8 for high-FLT3-expressing patients, indicating that these patients have a ~2 times greater chance of dying compared to the low-FLT3-expressing AML patients
[58][63] (
Figure 2).
Figure 2. Analysis of FLT3 expression in AML patients. (A) Transcript levels of FLT3 in AML patients versus control patients. (B) Percent survival of high-FLT3-expressing patients versus low-FLT3-expressing AML patients. The hazard ratio is 1.8, and the p-value is 0.035, as analyzed from the TCGA dataset upon GEPIA analysis.
FLT3 ligand (FL) is detectable during homeostasis and is increased in hypoplasia. FL is markedly elevated upon the depletion of the hematopoietic stem or progenitor cells. However, in FLT3
+ AML, the levels of FL fall to undetectable levels. It was observed that, after the induction of chemotherapy, FL levels are restored in patients with complete remission but not in patients with refractory disease. FL levels were measured in a randomized study with lestaurtinib where it was seen that patients achieving complete remission (CR) had higher FL levels after the completion of the therapy followed by a normal range after recovery. However, patients with refractory disease had a transient increase in FL levels followed by rapid depletion
[59][64]. Thus, FL levels have the potential to emerge as prognostic biomarkers to guide clinical decisions.
The presence or absence of specific gene mutations can be utilized to classify AML patients and determine their prognosis. The NCCN AML prognostic stratification system listed FLT3, NPM1, CEBPA, IDH1/2, DNMT3A (DNA methyltransferase 3A), KIT, TP53 (tumor suppressor 53), RUNX1, and ASXL1 (ASXL transcription factor) gene mutations for the classification of the AML patient population
[60][61][65,66]. Mutations of NRAS and IDH2 occur in FLT3-independent clones, but TET2 and IDH1 co-occur in FLT3-mutant clones
[62][67].
Mutations in the FLT3 gene are of prognostic value for detecting AML in patients. The most common FLT3 mutations (FLT3
mut) occur in the JM domain internal tandem duplications, FLT3-ITD
mut, or in the tyrosine kinase domain, FLT3-TKD
mut. FLT3-ITD
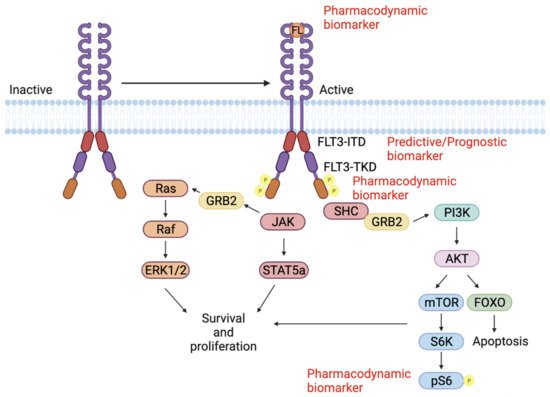
mut, are in-frame mutations consisting of duplications of 3–400 base pairs which lead to an elongated JM. This results in constitutive activation of the FLT3 receptor and the downstream signaling (
Figure 3)
[63][64][68,69].
Figure 3. FLT3 signaling pathway. FL binds to the FLT3 receptor and induces receptor dimerization and conformational changes. FLT3 autophosphorylation activates intracellular signaling cascades including RAS/RAF/MAPK PI3K/AKT/mTOR and JAK/STAT. These pathways control cell proliferation, survival, and apoptosis. These different proteins can be used as predictive, prognostic, and pharmacodynamic biomarkers.
The prognostic value of FLT3-ITD is determined by various factors, including the allele ratio (AR), ITD length, karyotype, insertion site, and co-mutations (NPM1)
[11][65][11,70]. AR is the ratio of ITD-mutated alleles to wild-type alleles (FLT3-ITD/FLT3 wild-type). Similarly, variant allele frequency is determined by the ratio of ITD-mutated alleles to ITD-mutated and wild-type alleles. The European Leukemia Net (ELN) identified a value of 0.5 as a cut-off to distinguish between low and high AR
[66][71]. FLT3-ITD insertion (AR > 0.51) is associated with an unfavorable, relapse-free survival, RFS (
p = 0.0008) and OS (
p = 0.004)
[67][72]. However, a recent study depicted that the size of FLT3-ITD mutations has no prognostic impact on the overall survival, relapse, or complete remission rate among newly diagnosed AML patients treated with chemotherapy
[68][73].
Favorable relapse risk and OS was seen with the occurrence of co-mutations NPM1, along with FLT3
mut, in young adult AML patients
[69][74]. In patients with concurrent NPM1
mut, the OS and relapse risk were comparable between FLT3 wild-type and FLT3-ITD
mut (AR < 0.5), but worse when AR ≥ 0.5
[70][75]. Among patients with NPM1 wild-type, all FLT3-ITD
mut patients had an increased risk of relapse and inferior OS, regardless of the AR. The European Leukemia Net (ELN) guidelines categorize FLT3-ITD
mut AML into three categories: favorable (NPM1
mut with FLT3 wild-type or NPM1
mut with FLT3-ITD AR < 0.5), intermediate (NPM1
mut with FLT3-ITD AR > 0.5 or NPM1WT with FLT3-ITD AR < 0.5), and adverse (NPM1WT with FLT3-ITD AR > 0.5)
[71][76]. Although the AR ratio is predictive of the severity of AML in the patients, a strict threshold cannot be established for clinical decision making. This is because the current assays are not optimized, and there is a high intrasample variability
[72][77].
FLT3-TKD mutations have prognostic value in the overall AML patient population, but the impact of FLT3-TKD
mut AR remains obscure. However FLT3-TKD
mut has a high incidence in co-occurrence with mutations in NPM1, CEBPA, and NRAS
[73][78]. These TKD mutations can be identified and detected using next-generation sequencing (NGS). Additionally, computational, biology-based algorithms, such as Pindel, show high sensitivity and specificity in detecting these gene alterations
[74][79].