Halitosis, also known as fetor ex ore, bad breath or oral malodor, is a common disorder meaning unpleasant smell from the mouth.
Halitosis is a common problem that manifests as an unpleasant and disgusting odor emanating from the mouth[1]. Malodor is mainly caused by putrefactive actions of microorganisms on endogenous or exogenous proteins and peptides. Oral malodor is an embarrassing condition that affects a large percentage of the human population. This condition often results in nervousness, humiliation, and social difficulties, such as the inability to approach people and speak to them[2][3][4][5][6].
- Halitosis
- Malodor
- Volatile sulfur compounds
- hydrogen sulfide
- microbiota
- Fusobacterium
- Porphyromonas
- Prevotella
- periodontitis
- carcinogenesis
Halitosis is a common problem that manifests as an unpleasant and disgusting odor emanating from the mouth[1]. Malodor is mainly caused by putrefactive actions of microorganisms on endogenous or exogenous proteins and peptides. Oral malodor is an embarrassing condition that affects a large percentage of the human population. This condition often results in nervousness, humiliation, and social difficulties, such as the inability to approach people and speak to them[2][3][4][5][6].
1. Introduction
Halitosis experiences from about 15% to 60% of the human population worldwide[7][8][9][10][11][12]. Halitosis can be divided into extra-oral halitosis (EOH) and intra-oral halitosis (IOH)[2][3][5].
The factors that increase the likelihood of halitosis include periodontal diseases, dry mouth, smoking, alcohol consumption, dietary habits, diabetes, and obesity. Halitosis can also be affected by the general hygiene of the body (i.e., dehydration, starvation, and high physical exertion), advanced age, bleeding gums, decreased brushing frequency, but also by stress[3][13][14][15][16]. Produced during stress, catecholamines and cortisol increased hydrogen sulfide production by sub-gingival anaerobic bacteria[17]. The medications which can cause extra-oral halitosis were categorized into 10 groups: acid reducers, aminothiols, anticholinergics, antidepressants, antifungals, antihistamines and steroids, antispasmodics, chemotherapeutic agents, dietary supplements, and organosulfur substances[18].
More and more patients are struggling with bad breath and report this problem to their primary care practitioner for diagnosis and management[19][20]. However, many physicians, dentists, and biologists have insufficient knowledge regarding the cause and biochemistry of this disease.
2. Classifications of Halitosis
In the literature, mainly three classifications of halitosis are used, described by Miyazaki et al., 1999[21], Tangerman and Winkel in 2010[22], and Aydin and Harvey-Woodworth in 2014[23](Figure 1).
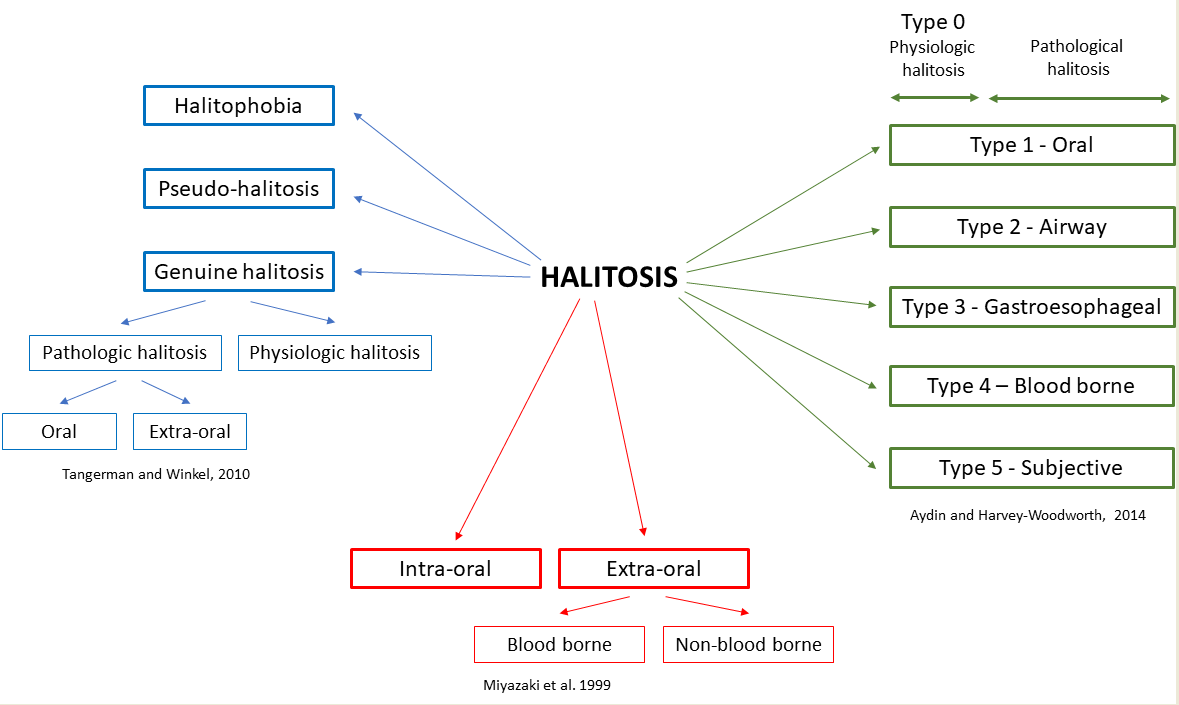
Figure 1. Classifications of halitosis[21][22][23][24].
Miyazaki et al. divided halitosis as intra-oral (IOH) and extra-oral (EOH)[21]. Extra-oral halitosis can be of bloodborne or non-bloodborne origin and covers about 5–10% of all halitosis[22]. Bloodborne-related causes include diabetes metabolic disorders, kidney and liver diseases, and certain drugs and food. Non-bloodborne-related causes include respiratory and gastrointestinal diseases. Meanwhile, pathological conditions in the oral cavity are responsible for 80–90% of IOH[2][3][25]. Both aerobic and anaerobic bacteria can be responsible for IOH. These microorganisms tend to produce foul-smelling, sulfur-containing gases called volatile sulfur compounds (VSCs)[23][26].
In the classification of Tangerman and Winkel[22], halitosis is classified as genuine and delusional. Delusional halitosis (monosymptomatic hypochondriasis; imaginary halitosis) is a condition in which patients believe that their breath is smelly and offensive. The social pressure of having fresh smelling breath increases the number of people that are preoccupied with this condition. However, the perception of oral malodor does not always reflect actual clinical oral malodor[27]. Self-perceived halitosis was found to be more prevalent amongst males, particularly smokers, compared to females. However, there are no statistical differences when comparing with different age groups[28]. Genuine halitosis is further subdivided into physiological and pathological halitosis. Physiological halitosis (foul morning breath, morning halitosis) is caused by saliva retention, as well as the putrefaction of entrapped food particles. Meanwhile, intra- and extra-oral causes are responsible for pathological halitosis[3][4][19].
Aydin and Harvey-Woodworth divided pathologic halitosis into five types: Type 1 (oral), Type 2 (airway), Type 3 (gastroesophageal), Type 4 (blood-borne) and Type 5 (subjective). Moreover, it is Type 0 halitosis (physiologic odor), which can be a connection of the physiologic contributions of oral, airway, gastroesophageal, blood-borne, and subjective halitosis. Any combination of the above types can be present in every healthy person[23].
References
- Pieniążek, A.; Pietrzak, M.; Halitoza-etiologia, metody diagnostyki i leczenie. Halitosis-etiology, methods of diagnosis and treatment. J. Health Study Med. 2017, 2, 101–122.
- Anbari, F.; Ashouri Moghaddam, A.; Sabeti, E.; Khodabakhshi, A. Halitosis: Helicobacter pylori or oral factors. Helicobacter 2019, 24, e12556.
- De Geest, S.; Laleman, I.; Teughels, W.; Dekeyser, C.; Quirynen, M. Periodontal diseases as a source of halitosis: A review of the evidence and treatment approaches for dentists and dental hygienists. Periodontology 2000 2016, 71, 213–227.
- Kapoor, U.; Sharma, G.; Juneja, M.; Nagpal, A. Halitosis: Current concepts on etiology, diagnosis and management. Eur. J. Dent. 2016, 10, 292–300.
- Seerangaiyan, K.; van Winkelhoff, A.J.; Harmsen, H.J.M.; Rossen, J.W.A.; Winkel, E.G. The tongue microbiome in healthy subjects and patients with intra-oral halitosis. J. Breath. Res. 2017, 11, 036010.
- Veloso, D.J.; Abrão, F.; Martins, C.H.G.; Bronzato, J.D.; Gomes, B.P.F.A.; Higino, J.S.; Sampaio, F.C. Potential antibacterial and anti-halitosis activity of medicinal plants against oral bacteria. Arch. Oral Biol. 2020, 110, 104585.
- Seemann, R.; Filippi, A.; Michaelis, S.; Lauterbach, S.; John, H.-D.; Huismann, J. Duration of effect of the mouthwash CB12 for the treatment of intra-oral halitosis: A double-blind, randomised, controlled trial. J. Breath Res. 2016, 10, 036002.
- Kumbargere Nagraj, S.; Eachempati, P.; Uma, E.; Singh, V.P.; Ismail, N.M.; Varghese, E. Interventions for managing halitosis. Cochrane Database Syst. Rev. 2019, 12, CD012213.
- Nadanovsky, P.; Carvalho, L.B.M.; Ponce de Leon, A. Oral malodour and its association with age and sex in a general population in Brazil. Oral Dis. 2007, 13, 105–109.
- Nalçaci, R.; Dülgergil, T.; Oba, A.A.; Gelgör, I.E. Prevalence of breath malodour in 7–11-year-old children living in Middle Anatolia, Turkey. Community Dent. Health 2008, 25, 173–177.
- Bornstein, M.M.; Kislig, K.; Hoti, B.B.; Seemann, R.; Lussi, A. Prevalence of halitosis in the population of the city of Bern, Switzerland: A study comparing self-reported and clinical data. Eur. J. Oral Sci. 2009, 117, 261–267.
- Yokoyama, S.; Ohnuki, M.; Shinada, K.; Ueno, M.; Wright, F.A.C.; Kawaguchi, Y. Oral malodor and related factors in Japanese senior high school students. J. Sch. Health 2010, 80, 346–352.
- Chen, X.; Zhang, Y.; Lu, H.-X.; Feng, X.-P. Factors Associated with Halitosis in White-Collar Employees in Shanghai, China. PLoS ONE 2016, 11, e0155592.
- Boyanova, L. Stress hormone epinephrine (adrenaline) and norepinephrine (noradrenaline) effects on the anaerobic bacteria. Anaerobe 2017, 44, 13–19.
- De Lima, P.O.; Nani, B.D.; Rolim, G.S.; Groppo, F.C.; Franz-Montan, M.; Alves De Moraes, A.B.; Cogo-Müller, K.; Marcondes, F.K. Effects of academic stress on the levels of oral volatile sulfur compounds, halitosis-related bacteria and stress biomarkers of healthy female undergraduate students. J. Breath Res. 2020, 14, 036005.
- Wu, J.; Cannon, R.D.; Ji, P.; Farella, M.; Mei, L. Halitosis: Prevalence, risk factors, sources, measurement and treatment—A review of the literature. Aust. Dent. J. 2020, 65, 4–11.
- Caroline Morini Calil; Gisele Mattos Oliveira; Karina Cogo; Antonio Carlos Pereira; Fernanda Klein Marcondes; Francisco Carlos Groppo; Effects of stress hormones on the production of volatile sulfur compounds by periodontopathogenic bacteria.. Brazilian Oral Research 2014, 28, 1-8, 10.1590/1807-3107bor-2014.vol28.0008.
- Hamed Mortazavi; Behrad Rahbani Nobar; Shervin Shafiei; Drug-related Halitosis: A Systematic Review.. Oral health & preventive dentistry 2020, 18, 399-407.
- Bicak, D.A. A Current Approach to Halitosis and Oral Malodor—A Mini Review. Open Dent. J. 2018, 12, 322–330.
- Gokdogan, O.; Catli, T.; Ileri, F. Halitosis in otorhinolaryngology practice. Iran. J. Otorhinolaryngol. 2015, 27, 145–153.
- Miyazaki, H.; Arao, M.; Okamura, K.; Kawaguchi, Y.; Toyofuku, A.; Hoshi, K.; Yaegaki, K.; Tentative classification of halitosis and its treatment needs. Niigata Dent. J. 1999, 32, 7–11.
- Albert Tangerman; E G Winkel; Extra-oral halitosis: an overview. Journal of Breath Research 2010, 4, 017003, 10.1088/1752-7155/4/1/017003.
- Murat Aydin; C. N. Harvey-Woodworth; Halitosis: a new definition and classification. British Dental Journal 2014, 217, E1-E1, 10.1038/sj.bdj.2014.552.
- Rainer Seemann; Maurício Duarte Da Conceição; Andreas Filippi; John Greenman; P Lenton; S Nachnani; Marc Quirynen; S Roldan; H. Schulze; Nir Sterer; et al.A TangermanE G WinkelK. YaegakiM Rosenberg Halitosis management by the general dental practitioner—results of an international consensus workshop. Journal of Breath Research 2014, 8, 017101, 10.1088/1752-7155/8/1/017101.
- Koczorowski, R.; Karpiński, T.M.; Halitosis—Problem społeczny. Halitosis—A social problem. Now. Lek. 2001, 70, 657–664.
- Albert Tangerman; Edwin G. Winkel; Volatile Sulfur Compounds as The Cause of Bad Breath: A Review. Phosphorus, Sulfur, and Silicon and the Related Elements 2013, 188, 396-402, 10.1080/10426507.2012.736894.
- Haslina Rani; Masayuki Ueno; Takashi Zaitsu; Sayaka Furukawa; Yoko Kawaguchi; Factors associated with clinical and perceived oral malodor among dental students.. Journal of medical and dental sciences 2015, 62, 33–41.
- Salwa Abdulrahman Alsadhan; Self-perceived halitosis and related factors among adults residing in Riyadh, Saudi Arabia. A cross sectional study.. The Saudi Dental Journal 2016, 28, 118-123, 10.1016/j.sdentj.2016.06.001.