Obstetric and newborn outcomes of assisted reproductive technology (ART) pregnancies are associated with significative prevalence of maternal and neonatal adverse health conditions, such as cardiovascular and metabolic diseases. These data are interpreted as anomalies in placentation involving a dysregulation of several molecular factors and pathways. It is not clear which extent of the observed placental alterations are the result of ART and which originate from infertility itself. These two aspects probably act synergically for the final obstetric risk. Data show that mechanisms of inappropriate trophoblast invasion and consequent altered vascular remodeling sustain several clinical conditions, leading to obstetric and perinatal risks often found in ART pregnancies, such as preeclampsia, fetal growth restriction and placenta previa or accreta.
- placenta
- placental dysfunction
- assisted reproduction techniques
- infertility
- preeclampsia
1. Introduction
2. Abnormal Placentation and ART: Molecular Factors and Involved Signaling
Abnormal placentation may present in a variety of phenotypes, severity, clinical conditions and consequences as the result of several types of infertility treatments and techniques used in ART. For these reasons, it becomes difficult to linearly relate placental influence to obstetrical and perinatal (or neonatal) outcomes after ART. An altered expression of factors and molecules involved in proper placental development, leading to impaired trophoblast invasion and subsequent reduced vascular remodeling and placenta hypoperfusion, sustain several clinical conditions leading to obstetric and perinatal risks often found in ART pregnancies, such as PE, FGR and placenta previa or accrete (Figure 1) [24,25,26,27,28][14][15][16][17][18]. Syncytiotrophoblast stress has been associated with a dysregulated expression of placental growth factor (PlGF) and soluble fms-like tyrosine kinase 1 (sFLT-1) [29,30][19][20]. Circulating levels of the anti-angiogenic factor sFLT-1 are increased, and those of PlGF are decreased even before the onset of the clinical symptoms of PE and FGR [31,32,33,34,35][21][22][23][24][25]. The increased ratio sFLT-1:PlGF is thought to contribute to the systemic endothelial response and correlate with the severity of FGR and PE.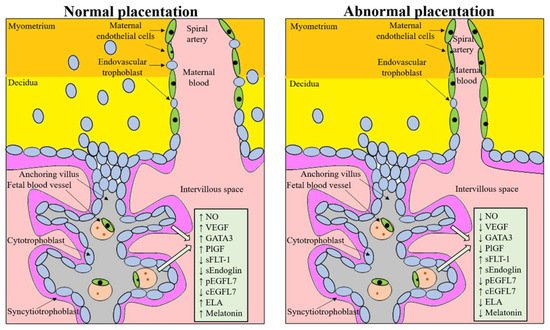
3. Pathophysiology of the Placenta in Pregnancy Complications and ART Pregnancies
3.1. Altered Hormonal Milieu Effect on Placental Development
Several common infertility conditions, such as endometriosis and PCOS, often treated with ART, are characterized by a hormonal dysregulation that affects proper placentation. In endometriosis, a defective deep placentation may derive from functional abnormalities of the eutopic endometrium, as well as an imbalance in endocrine and inflammatory markers [72][48]. PTB, placenta previa, placental abruption, gestational hypertension, PE, LBW, SGA, cesarean delivery, postpartum hemorrhage, and stillbirth have been significantly associated with endometriosis in a systematic review and meta-analyses, including in 39 studies [73][49]. PCOS is another condition leading to infertility, in which the defective trophoblast invasion and placentation may be caused by mother’s hyperandrogenism [74,75][50][51]. Testosterone can act directly on trophoblast invasion, with modifications of placenta morphology and function [76,77][52][53]. PCOS is a chronic low-grade inflammation associated with metabolic dysfunction that is enhanced in pregnancy by the induction of an endothelial dysfunction [78][54]. This condition might in turn prevent normal remodeling of spiral vessels and the physiologic decrease of uterine artery impedance, thus reducing the depth of endovascular trophoblast invasion. As a consequence of these patterns, in patients with PCOS the placental weight, thickness, density and volume was found significantly reduced [76][52].
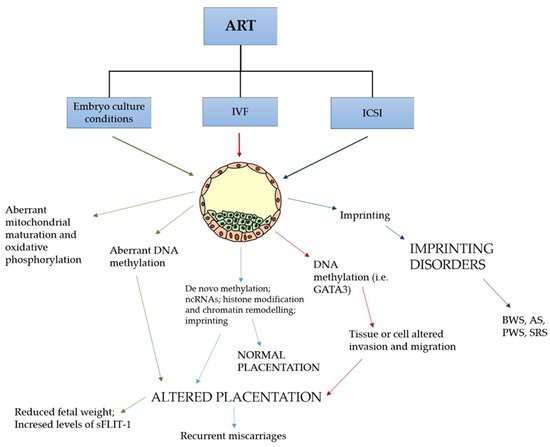
3.2. Epigenetic Changes after ART Techniques Are Associated with Altered Gene Expression in the Placenta and Congenital Imprinting Disorders
3.3. Immune Dysregulation at the Maternal-Fetal Interface
3.4. Mechanical Stress on Embryo and Placental Development (the Case of PGT-A)
PGT-A is an ART technique that is increasingly performed, considering that it represents 40% of all IVF cycles in the USA [115][68]. Its aim is to discover if produced embryos are aneuploid and, in this case, they should not be transferred into the uterus, in order to prevent implantation failure and miscarriages. PGT-A preliminarily requires the in vitro development of embryos up to the blastocyst stage, in order to collect 5 to 10 trophoblast cells. Embryos are then frozen while waiting for the genetic analysis results. Embryos with no or few aneuploidies are thawed and transferred (FET) in the uterine cavity after endometrial hormonal preparation using estrogen and progesterone. In this condition, natural ovulation and formation of the corpus luteum are suppressed. Similar to PGT-A, preimplantation genetic test for monogenic diseases (PGT-M) allows to screen for embryos affected by monogenic diseases.
4. Metabolic and Cardiovascular Consequences of Placental Dysregulation in Mothers Following ART
5. Health Risk in Infancy as a Consequence of Placental Dysfunction Following ART
According to the “developmental origins of health and disease theory” [143][76] and the Barker hypothesis of the developmental origins of chronic adult disease [144][77], placental dysfunction and abnormal fetal development may have long-term consequences on the neonate and his development, from childhood to adult life. A higher risk of diabetes mellitus and CVD were found in children whose mothers had PE and HDP, by long-term follow up observations [145,146][78][79]. A track of this condition is represented by the finding of reduced endothelial function in mothers and children after PE [147][80].
Additionally, there is increasing evidence that offspring conceived by IVF displays a level of vascular dysfunction similar to that seen in children spontaneously conceived by mothers with PE [132,133][69][70]. Of note, in 2015 in a randomized case-control trial, antioxidant administration to IVF children was able to improve NO bioavailability and responsiveness of both systemic and pulmonary circulation [149][81], thus indicating that vascular dysfunctions induced by ART are reversible in young people.
6. Simultaneous Action of Factors Dysregulating Normal Placentation
References
- Messerlian, C.; Maclagan, L.; Basso, O. Infertility and the risk of adverse pregnancy outcomes: A systematic review and meta-analysis. Hum. Reprod. 2013, 28, 125–137.
- Healy, D.L.; Breheny, S.; Halliday, J.; Jaques, A.; Rushford, D.; Garrett, C.; Talbot, J.M.; Baker, H.W. Prevalence and risk factors for obstetric haemorrhage in 6730 singleton births after assisted reproductive technology in Victoria Australia. Hum. Reprod. 2010, 25, 265–274.
- Palomba, S.; de Wilde, M.A.; Falbo, A.; Koster, M.P.; La Sala, G.B.; Fauser, B.C. Pregnancy complications in women with polycystic ovary syndrome. Hum. Reprod. Update 2015, 21, 575–592.
- Vambergue, A.; Fajardy, I. Consequences of gestational and pregestational diabetes on placental function and birth weight. World J. Diabetes 2011, 2, 196–203.
- Helmerhorst, F.M.; Perquin, D.A.M.; Donker, D.; Keirse, M.J.N.C. Perinatal outcome of singletons and twins after assisted conception: A systematic review of controlled studies. BMJ 2004, 328, 261–264.
- Pandey, S.; Shetty, A.; Hamilton, M.; Bhattacharya, S.; Maheshwari, A. Obstetric and perinatal outcomes in singleton pregnancies resulting from IVF/ICSI: A systematic review and meta-analysis. Hum. Reprod. Update 2012, 18, 485–503.
- Luke, B. Pregnancy and birth outcomes in couples with infertility with and without assisted reproductive technology: With an emphasis on US population-based studies. Am. J. Obstet. Gynecol. 2017, 217, 270–281.
- Ginström Ernstad, E.; Wennerholm, U.; Khatibi, A.; Petzold, M.; Bergh, C. Neonatal and maternal outcome after frozen embryo transfer; increased risks in programmed cycles. Am. J. Obstet. Gynecol. 2019, 221, 126.e1–126.e18.
- Saito, K.; Kuwahara, A.; Ishikawa, T.; Morisaki, N.; Miyado, M.; Miyado, K.; Fukami, M.; Miyasaka, N.; Ishihara, O.; Irahara, M.; et al. Endometrial preparation methods for frozen-thawed embryo transfer are associated with altered risks of hypertensive disorders of pregnancy, placenta accreta, and gestational diabetes mellitus. Hum. Reprod. 2019, 34, 1567–1575.
- Sunderam, S.; Kissin, D.M.; Zhang, Y.; Folger, S.G.; Boulet, S.L.; Warner, L.; Callaghan, W.M.; Barfield, W.D. Assisted reproductive technology surveillance—United States, 2016. MMWR Surveill. Summ. 2019, 68, 1–23.
- Luke, B.; Brown, M.B.; Eisenberg, M.L.; Callan, C.; Botting, B.J.; Pacey, A.; Alastair, G. In vitro fertilization and risk for hypertensive disorders of pregnancy: Associations with treatment parameters. Am. J. Obstet. Gynecol. 2020, 222, 350.e1–350.e13.
- Manna, C. Maternal-Fetal Medicine, Practical Aspects Il; Arduini, D., Palermo, M.S.F., Eds.; AMOLCA Publishing House: Medellin, Colombia, 2021.
- Xiang, M.; Chen, S.; Zhang, X.; Ma, Y. Placental diseases associated with assisted reproductive technology. Reprod. Biol. 2021, 21, 100505.
- Brosens, I.; Pijnenborg, R.; Vercruysse, L.; Romero, R. The “Great Obstetrical Syndromes” are associated with disorders of deep placentation. Am. J. Obstet. Gynecol. 2011, 204, 193–201.
- Fisher, S.J. Why is placentation abnormal in preeclampsia? Am. J. Obstet. Gynecol. 2015, 213 (Suppl. 4), S115–S122.
- Burton, G.J.; Yung, H.W.; Cindrova-Davies, T.; Charnock-Jones, D.S. Placental endoplasmic reticulum stress and oxidative stress in the pathophysiology of unexplained intrauterine growth restriction and early onset preeclampsia. Placenta 2009, 30, S43–S48.
- Jackson, M.R.; Walsh, A.J.; Morrow, R.J.; Mullen, J.B.; Lye, S.J.; Ritchie, J.W. Reduced placental villous tree elaboration in small-for-gestational-age pregnancies: Relationship with umbilical artery Doppler waveforms. Am. J. Obstet. Gynecol. 1995, 172, 518–525.
- Redman, C.W.; Sargent, I.L. Latest advances in understanding preeclampsia. Science 2005, 308, 1592–1594.
- Benschop, L.; Schalekamp-Timmermans, S.; Broere-Brown, Z.A.; Roeters van Lennep, J.E.; Jaddoe, V.W.V.; Roos-Hesselink, J.W.; Ikram, M.K.; Steegers, E.A.P.; Robert, J.M.; Gandley, R.E. Placental growth factor as an indicator of maternal cardiovascular risk after pregnancy. Circulation 2019, 139, 1698–1709.
- Redman, C.W.; Staff, A.C. Preeclampsia, biomarkers, syncytiotrophoblast stress, and placental capacity. Am. J. Obstet. Gynecol. 2015, 213 (Suppl. 4), S9.e1–S9.e4.
- Zeisler, H.; Llurba, E.; Chantraine, F.; Vatish, M.; Staff, A.C.; Sennström, M.; Olovsson, M.; Brennecke, S.P.; Stepan, H.; Allegranza, D.; et al. Pre-dictive Value of the sFlt-1:PlGF Ratio in Women with Suspected Preeclampsia. N. Engl. J. Med. 2016, 374, 13–22.
- Stepan, H.; Unversucht, A.; Wessel, N.; Faber, R. Predictive value of maternal angiogenic factors in second trimester pregnancies with abnormal uterine perfusion. Hypertension 2007, 49, 818–824.
- Hertig, A.; Berkane, N.; Lefevre, G.; Toumi, K.; Marti, H.P.; Capeau, J.; Uzan, S.; Rondeau, E. Maternal serum sFLT-1 concentration is an early and reliable predictive marker of preeclampsia. Clin. Chem. 2004, 50, 1702–1703.
- Tidwell, S.C.; Ho, H.N.; Chiu, W.H.; Torry, R.J.; Torry, D.S. Low maternal serum levels of placenta growth factor as an antecedent of clinical preeclampsia. Am. J. Obstet. Gynecol. 2001, 184, 1267–1272.
- Thadhani, R.; Mutter, W.P.; Wolf, M.; Levine, R.J.; Taylor, R.N.; Sukhatme, V.P.; Ecker, J.; Karumanchi, S.A. First trimester placental growth factor and solu-ble fms-like tyrosine kinase 1 and risk for preeclampsia. J. Clin. Endocrinol. Metab. 2004, 89, 770–775.
- Cui, L.; Shu, C.; Liu, Z.; Tong, W.; Cui, M.; Wei, C.; Tang, J.J.; Liu, X.; Hu, J.; Jiang, J.; et al. The expression of serum sEGFR, sFlt-1, sEndoglin and PLGF in preeclampsia. Pregnancy Hypertens. 2018, 13, 127–132.
- Levine, R.J.; Lam, C.; Qian, C.; Yu, K.F.; Maynard, S.E.; Sachs, B.P.; Sibai, B.M.; Epstein, F.H.; Romero, R.; Thadhani, R.; et al. Soluble endoglin and other circulating antiangiogenic factors in preeclampsia. N. Engl. J. Med. 2006, 355, 992–1005.
- Lacko, L.A.; Massimiani, M.; Sones, J.L.; Hurtado, R.; Salvi, S.; Ferrazzani, S.; Davisson, R.L.; Campagnolo, L.; Stuhlmann, H. Novel expression of EGFL7 in placental trophoblast and endothelial cells and its implication in preeclampsia. Mech. Dev. 2014, 133, 163–176.
- Massimiani, M.; Vecchione, L.; Piccirilli, D.; Spitalieri, P.; Amati, F.; Salvi, S.; Ferrazzani, S.; Stuhlmann, H.; Campagnolo, L. Epidermal growth factor-like domain 7 promotes migration and invasion of human trophoblast cells through activation of MAPK, PI3K and NOTCH signaling pathways. Mol. Hum. Reprod. 2015, 21, 435–451.
- Lacko, L.A.; Hurtado, R.; Hinds, S.; Poulos, M.G.; Butler, J.M.; Stuhlmann, H. Altered feto-placental vascularization, feto-placental malperfusion and fetal growth restriction in mice with Egfl7 loss of function. Development. 2017, 144, 2469–2479.
- Massimiani, M.; Salvi, S.; Tiralongo, G.M.; Moresi, S.; Stuhlmann, H.; Valensise, H.; Lanzone, A.; Campagnolo, L. Circulating EGFL7 distinguishes between FGR and PE: An observational case-control study. Sci. Rep. 2021, 11, 17919.
- Massimiani, M.; Lacko, L.A.; Burke Swanson, C.S.; Salvi, S.; Argueta, L.B.; Moresi, S.; Ferrazzani, S.; Gelber, S.E.; Baergen, R.N.; Toschi, N.; et al. Increased circulating levels of Epidermal Growth Factor-like Domain 7 in pregnant women affected by preeclampsia. Transl. Res. 2019, 207, 19–29.
- Massimiani, M.; Tiralongo, G.M.; Salvi, S.; Fruci, S.; Lacconi, V.; La Civita, F.; Mancini, M.; Stuhlmann, H.; Valensise, H.; Campagnolo, L. Treatment of pregnancies complicated by intrauterine growth restriction with nitric oxide donors increases placental expression of Epidermal Growth Factor-Like Domain 7 and improves fetal growth: A pilot study. Transl. Res. 2021, 228, 28–41.
- Valensise, H.; Vasapollo, B.; Novelli, G.P.; Giorgi, G.; Verallo, P.; Galante, A.; Arduini, D. Maternal and fetal hemodynamic effects induced by nitric oxide donors and plasma volume expansion in pregnancies with gestational hypertension complicated by intrauterine growth restriction with absent end diastolic flow in the umbilical artery. Ultrasound Obstet. Gynecol. 2008, 31, 55–64.
- Berbets, A.; Koval, H.; Barbe, A.; Albota, O.; Yuzko, O. Melatonin decreases and cytokines increase in women with placental insufficiency. J. Matern.-Fetal Neonatal Med. 2019, 25, 1–6.
- Chuffa, L.G.; Lupi, L.A., Jr.; Seiva, F.R.; Martinez, M.; Domeniconi, R.F.; Pinheiro, P.F.; Dos Santos, L.D.; Martinez, F.E. Quantitative proteomic profiling reveals that diverse metabolic pathways are influenced by melatonin in an in vivo model of ovarian carcinoma. J. Proteome Res. 2016, 15, 3872–3882.
- De Almeida Chuffa, L.G.; Seiva, F.R.F.; Cucielo, M.S.; Silveira, H.S.; Reiter, R.J.; Lupi, L.A. Mitochondrial functions and melatonin: A tour of the reproductive cancers. Cell. Mol. Life Sci. 2019, 76, 837–863.
- Itoh, M.T.; Ishizuka, B.; Kudo, Y.; Fusama, S.; Amemiya, A.; Sumi, Y. Detection of melatonin and serotonin N-acetyltransferase and hydroxyindole-Omethyltransferase activities in the rat ovary. Mol. Cell Endocrinol. 1997, 136, 7–14.
- Itoh, M.T.; Ishizuka, B.; Kuribayashi, Y.; Amemiya, A.; Sumi, Y. Melatonin, its precursors, and synthesizing enzyme activities in the human ovary. Mol. Hum. Reprod. 1999, 5, 402–408.
- El-Raey, M.; Geshi, M.; Somfai, T.; Kaneda, M.; Hirako, M.; Abdel-Ghaffar, A.E.; Sosa, G.A.; El-Roos, M.E.A.; Nagai, T. Evidence of melatonin synthesis in the cumulus oocyte complexes and its role in enhancing oocyte maturation in vitro in cattle. Mol. Reprod. Dev. 2011, 78, 250–262.
- Amireault, P.; Dube, F. Serotonin and its antidepressant-sensitive transport in mouse cumulus-oocyte complexes and early embryos. Biol. Reprod. 2005, 73, 358–365.
- Sakaguchi, K.; Itoh, M.T.; Takahaashi, N.; Tarumi, W.; Ishizuka, B. The rat oocyte synthesises melatonin. Reprod. Fertil. Dev. 2013, 25, 674–682.
- Tamura, H.; Takasaki, A.; Miwa, I.; Taniguchi, K.; Maekawa, R.; Asada, H.; Taketani, T.; Matsuoka, A.; Yamagata, Y.; Shimamura, K.; et al. Oxidative stress impairs oocyte quality and melatonin protects oocytes from free radical damage and improves fertilization rate. J. Pineal Res. 2008, 44, 280–287.
- Zheng, M.; Tong, J.; Li, W.P.; Chen, Z.J.; Zhang, C. Melaton in concentration in follicular fluid is correlated with antral follicle count (AFC) and in vitro fertilization (IVF) outcomes in women undergoing assisted reproductive technology (ART) procedures. Gynecol. Endocrinol. 2018, 34, 446–450.
- De Almeida Chuffa, L.G.; Seiva, F.R.F.; Cucielo, M.S.; Silveira, H.S.; Reiter, R.J.; Lupi, L.A. Clock genes and the role of melatonin in cancer cells: An overview. Melatonin Res. 2019, 2, 133–157.
- Moshkdanian, G.; Moghani-Ghoroghi, F.; Pasbakhsh, P.; Nematollahi-Mahani, S.N.; Najafi, A.; Kashani, S.R. Melatonin upregulates ErbB1 and ErbB4, two primary implantation receptors, in pre-implantation mouse embryos. Iran. J. Basic Med. Sci. 2017, 20, 655–661.
- Pan, B.; Qazi, I.H.; Guo, S.; Yang, J.; Qin, J.; Lv, T.; Zang, S.; Zhang, Y.; Zeng, C.; Meng, Q.; et al. Melatonin improves the first cleavage of parthenogenetic embryos from vitrified-warmed mouse oocytes potentially by promoting cell cycle progression. J. Anim. Sci. Biotechnol. 2021, 12, 84.
- Brosens, I.; Brosens, J.J.; Fusi, L.; Al-Sabbagh, M.; Kuroda, K.; Benagiano, G. Risks of adverse pregnancy outcome in endometriosis. Fertil. Steril. 2012, 98, 30–35.
- Breintoft, K.; Pinnerup, R.; Henriksen, T.; Rytter, D.; Uldbjerg, N.; Forman, A.; Arendt, L. Endometriosis and Risk of Adverse Pregnancy Outcome: A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 667.
- Jindal, P.; Regan, L.; Fourkala, E.O.; Rai, R.; Moore, G.; Goldin, R.D.; Sebire, N.J. Placental pathology of recurrent spontaneous abortion: The role of histopathological examination of products of conception in routine clinical practice: A mini review. Hum. Reprod. 2007, 22, 313–316.
- Longtine, M.S.; Nelson, D.M. Placental dysfunction and fetal programming: The importance of placental size, shape, histopathology, and molecular composition. Semin. Reprod. Med. 2011, 29, 187–196.
- Palomba, S.; Russo, T.; Falbo, A.; Di Cello, A.; Tolino, A.; Tucci, L.; La Sala, G.B.; Zullo, F. Macroscopic and microscopic findings of the placenta in women with polycystic ovary syndrome. Hum. Reprod. 2013, 28, 2838–2847.
- Palomba, S.; Russo, T.; Falbo, A.; Di Cello, A.; Amendola, G.; Mazza, R.; Tolino, A.; Zullo, F.; Tucci, L.; La Sala, G.B. Decidual endovascular trophoblast invasion in women with polycystic ovary syndrome: An experimental case-control study. J. Clin. Endocrinol. Metab. 2012, 97, 2441–2449.
- Palomba, S.; Falbo, A.; Russo, T.; Battista, L.; Tolino, A.; Orio, F.; Zullo, F. Uterine blood flow in pregnant patients with polycystic ovary syndrome: Relationships with clinical outcomes. BJOG 2010, 117, 711–721.
- Maccani, M.A.; Marsit, C.J. Epigenetics in the Placenta. Am. J. Reprod. Immunol. 2009, 62, 78–89.
- Maheshwari, A.; Hamilton, M.; Bhattacharya, S. Should we be promoting embryo transfer at blastocyst stage? Reprod. Biomed. Online 2016, 32, 142–146.
- Katari, S.; Turan, N.; Bibikova, M.; Erinle, O.; Chalian, R.; Foster, M.; Gaughan, J.P.; Coutifaris, C.; Sapienza, C. DNA methylation and gene expression differences in children conceived in vitro or in vivo. Hum. Mol. Genet. 2009, 18, 3769–3778.
- Nelissen, E.C.; van Montfoort, A.P.; Dumoulin, J.C.; Evers, J.L. Epigenetics and the placenta. Hum. Reprod. Update 2011, 17, 397–417.
- Robins, J.C.; Marsit, C.J.; Padbury, J.F.; Sharma, S.S. Endocrine disruptors, environmental oxygen, epigenetics and pregnancy. Front. Biosci. 2011, 3, 690–700.
- Novakovic, B.; Rakyan, V.; Ng, H.K.; Manuelpillai, U.; Dewi, C.; Wong, N.C.; Morley, R.; Down, T.; Beck, S.; Craig, J.M.; et al. Specific tumour-associated methylation in normal human term placenta and first-trimester cytotrophoblasts. Hum. Reprod. 2008, 14, 547–554.
- de Waal, E.; Mak, W.; Calhoun, S.; Stein, P.; Ord, T.; Krapp, C.; Coutifaris, C.; Schultz, R.M.; Bartolomei, M.S. In vitro culture increases the frequency of stochastic epigenetic errors at imprinted genes in placental tissues from mouse concepti produced through assisted reproductive technologies. Biol. Reprod. 2014, 90, 22.
- Li, B.; Chen, S.; Tang, N.; Xiao, X.; Huang, J.; Jiang, F.; Huang, X.; Sun, F.; Wang, X. Assisted reproduction causes reduced fetal growth associated with downregulation of paternally expressed imprinted genes that enhance fetal growth in mice. Biol. Reprod. 2016, 94, 45.
- Xiang, M.; Ma, Y.; Lei, H.; Wen, L.; Chen, S.; Wang, X. In vitro fertilization placenta overgrowth in mice is associated with downregulation of the paternal imprinting gene H19. Mol. Reprod. Dev. 2019, 86, 1940–1950.
- Chen, S.; Sun, F.Z.; Huang, X.; Wang, X.; Tang, N.; Zhu, B.; Li, B. Assisted reproduction causes placental maldevelopment and dysfunction linked to reduced fetal weight in mice. Sci. Rep. 2015, 5, 10596.
- Lee, B.; Kroener, L.L.; Xu, N.; Wang, E.T.; Banks, A.; Williams, J.; Goodarzi, M.O.; Chen, Y.I.; Tang, J.; Wang, Y.; et al. Function and Hormonal Regulation of GATA3 in Human First Trimester Placentation. Biol. Reprod. 2016, 95, 113.
- Gundogan, F.; Bianchi, D.W.; Scherjon, S.A.; Roberts, D.J. Placental pathology in egg donor pregnancies. Fertil. Steril. 2010, 93, 397–404.
- Rizzo, G.; Aiello, E.; Pietrolucci, M.E.; Arduini, D. Placental volume and uterine artery Doppler evaluation at 11 + 0 to 13 + 6 weeks’ gestation in pregnancies conceived with in-vitro fertilization: Comparison between autologous and donor oocyte recipients. Ultrasound Obstet. Gynecol. 2016, 47, 726–731.
- Munne, S. Status of preimplantation genetic testing and embryo selection. Reprod. Biomed. Online 2018, 37, 393–396.
- Rexhaj, E.; Paoloni-Giacobino, A.; Rimoldi, S.F.; Fuster, D.G.; Anderegg, M.; Somm, E.; Bouillet, E.; Allemann, Y.; Sartori, C.; Scherrer, U. Mice generated by in vitro fertilization exhibit vascular dysfunction and shortened life span. J. Clin. Investig. 2013, 123, 5052–5060.
- Jayet, P.Y.; Rimoldi, S.F.; Stuber, T.; Salmòn, C.S.; Hutter, D.; Rexhaj, E.; Thalmann, S.; Schwab, M.; Turini, P.; Sartori-Cucchia, C.; et al. Pulmonary and systemic vascular dysfunction in young offspring of mothers with preeclampsia. Circulation. 2010, 122, 488–494.
- Sundheimer, L.; Pisarska, M. Abnormal Placentation Associated with Infertility as a Marker of Overall Health. Semin. Reprod. Med. 2017, 35, 205–216.
- Brosens, I.A.; Robertson, W.B.; Dixon, H.G. The role of the spiral arteries in the pathogenesis of preeclampsia. Obstet. Gynecol. Annu. 1972, 1, 177–191.
- Cunningham, F.G.; Leveno, K.J. Childbearing among older women—The message is cautiously optimistic. N. Engl. J. Med. 1995, 333, 1002–1004.
- Kenny, L.C.; Lavender, T.; McNamee, R.; O’Neill, S.M.; Mills, T.; Khashan, A.S. Advanced maternal age and adverse pregnancy outcome: Evidence from a large contemporary cohort. PLoS ONE 2013, 8, e56583.
- Jackson, S.; Hong, C.; Wang, E.T.; Alexander, C.; Gregory, K.D.; Pisarska, M.D. Pregnancy outcomes in very advanced maternal age pregnancies: The impact of assisted reproductive technology. Fertil. Steril. 2015, 103, 76–80.
- Briana, D.D.; Germanou, K.; Boutsikou, M.; Boutsikou, T.; Athanasopoulos, N.; Marmarinos, A.; Gourgiotis, D.; Malamitsi-Puchner, A. Potential prognostic biomarkers of cardiovascular disease in fetal macrosomia: The impact of gestational diabetes. J. Matern.-Fetal Neonatal. Med. 2018, 31, 895–900.
- Barker, D.J. The developmental origins of chronic adult disease. Acta Paediatr. Suppl. 2004, 93, 26–33.
- Männistö, T.; Mendola, P.; Vääräsmäki, M.; Järvelin, M.R.; Hartikainen, A.L.; Pouta, A.; Suvanto, E. Elevated blood pressure in pregnancy and subsequent chronic disease risk. Circulation 2013, 127, 681–690.
- Brown, M.C.; Best, K.E.; Pearce, M.S.; Waugh, J.; Robson, S.C.; Bell, R. Cardiovascular disease risk in women with pre-eclampsia: Systematic review and meta-analysis. Eur. J. Epidemiol. 2013, 28, 1–19.
- Kvehaugen, A.S.; Dechend, R.; Ramstad, H.B.; Troisi, R.; Fugelseth, D.; Staff, A.C. Endothelial function and circulating biomarkers are disturbed in women and children after PE. Hypertension 2011, 58, 63–69.
- Rimoldi, S.F.; Sartori, C.; Rexhaj, E.; Bailey, D.M.; de Marchi, S.F.; McEneny, J.; von Arx, R.; Cerny, D.; Duplain, H.; Germond, M.; et al. Antioxidants improve vascular function in children conceived by assisted reproductive technologies: A randomized double-blind placebo-controlled trial. Eur. J. Prev. Cardiol. 2015, 22, 1399–1407.
- Song, S.; Ghosh, J.; Mainigi, M.; Turan, N.; Weinerman, R.; Truongcao, M.; Coutifaris, C.; Sapienza, C. DNA methylation differences between in vitro- and in vivo-conceived children are associated with ART procedures rather than infertility. Clin. Epigenet. 2015, 7, 41.
- Wale, P.L.; Gardner, D.K. The effects of chemical and physical factors on mammalian embryo culture and their importance for the practice of assisted human reproduction. Hum. Reprod. Update 2016, 22, 2–22.
- Chen, J.Z.; Sheehan, P.M.; Brennecke, S.P.; Keogh, R.J. Vessel remodelling, pregnancy hormones and extravillous trophoblast function. Mol. Cell Endocrinol. 2012, 349, 138–144.
- Imudia, A.N.; Awonuga, A.O.; Doyle, J.O.; Kaimal, A.J.; Wright, D.L.; Toth, T.L.; Styer, A.K. Peak serum estradiol level during controlled ovarian hyperstimulation is associated with increased risk of small for gestational age and PE in singleton pregnancies after in vitro fertilization. Fertil. Steril. 2012, 97, 1374–1379.
- Jones, M.L.; Mark, P.J.; Mori, T.A.; Keelan, J.A.; Waddell, B.J. Maternal dietary omega-3 fatty acid supplementation reduces placental oxidative stress and increases fetal and placental growth in the rat. Biol. Reprod. 2013, 88, 37.
- Myatt, L. Review: Reactive oxygen and nitrogen species and functional adaptation of the placenta. Placenta 2010, 31, S66–S69.
- Berntsen, S.; Söderström-Anttila, V.; Wennerholm, U.B.; Laivuori, H.; Loft, A.; Oldereid, N.B.; Romundstad, L.B.; Bergh, C.; Pinborg, A. The health of children conceived by ART: “The chicken or the egg?”. Hum. Reprod. Update 2019, 25, 137–158.