Pancreatic cancer is one of the most aggressive malignant neoplastic diseases. The incidence and mortality rates of this disease vary depending on geographical area, which might be explained by the different exposure to risk factors. Currently, the risk factors for pancreatic cancer fall into two broad categories, namely extrinsic and intrinsic factors. Extrinsic factors include alcohol consumption, smoking, a diet rich in saturated fats, and viral infections such as chronic infection with hepatitis B and C viruses. The pathophysiological mechanisms explaining how these hepatotropic viruses contribute to the development of pancreatic cancer are not fully elucidated. The common origin of hepatocytes and pancreatic cells in the multipotent endodermal cells, the common origin of the blood vessels and biliary ducts of the pancreas and the liver, or chronic inflammatory changes may be involved in this interaction.
- ancreatic cancer
- hepatitis B virus
- hepatitis C virus
- risk factors
- early diagnosis
1. Introduction
- BRCA2, STK11, CDKN2A, PALB2;
| Intrinsic Risk Factors | Extrinsic Risk Factors |
|---|---|
| Hereditary | Diet |
| AB0 blood group | Obesity |
| Chronic pancreatitis | Tobacco |
| Cystic fibrosis | Coffee and alcohol consumption |
| Pancreatic cysts | Helicobacter pylori infection |
| Diabetes mellitus and insulin resistance | Infection with hepatitis B virus (HBV) and hepatitis C virus (HCV) |
-
High-penetrance genes:
-
Patients with genetic syndromes at risk of developing malignancies, including pancreatic cancer (e.g., Li-Fraumeni syndrome, ataxia-telangiectasia syndrome, Peutz-Jeghers syndrome, Lynch II syndrome, etc.);
2. Viral Hepatitis: Virology and Epidemiology
Viral hepatitis is a worldwide public health problem because of the large number of affected individuals and the morbidity and mortality rates associated with these infectious disorders. Among viruses responsible for hepatitis, the most important are the hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis D (delta) virus (HDV), and hepatitis E virus (HEV) [53][18]. Of these, the only one that does not lead to chronic hepatitis is HAV, while HBV, HCV, HDV, and occasionally HEV may be responsible for long-term forms of viral liver infection [53][18]. HBV is a DNA virus, belonging to the Orthohepadnavirus genus, and is classified into 10 genotypes, A–J [56][19]. This virus can be transmitted sexually, by blood, and vertically, from the mother to the fetus [56][19]. HBV genotypes have several peculiarities in terms of geographical distribution, route of transmission, and organ damage [57][20].3. Hepatotropic Viruses and Pancreatic Cancer-Pathophysiological Links
HBV and HCV are hepatotropic viruses with oncogenic properties. These viruses can induce persistent liver injury, with subsequent progression to cirrhosis and hepatocellular carcinoma [62,63][21][22]. There are also data suggesting the involvement of these viruses in the development of other neoplasms, such as pancreatic cancer, intrahepatic and extrahepatic duct bile carcinoma, gastric cancer, oesophageal cancer, certain forms of non-Hodgkin’s lymphoma, and leukemia [64,65,66,67][23][24][25][26]. Anatomically, the pancreas is situated in the proximity of the liver. The common origin of the blood vessels and bile ducts of these organs makes possible the microorganisms’ migration [52][27]. Antigens and replicative sequences of these two viruses have also been identified in extrahepatic tissues (e.g., the pancreas, the kidneys, and the skin) [68,69][28][29]. Figure 21 summarizes the pathophysiological mechanisms by which hepatotropic viruses may contribute to the development of pancreatic cancer.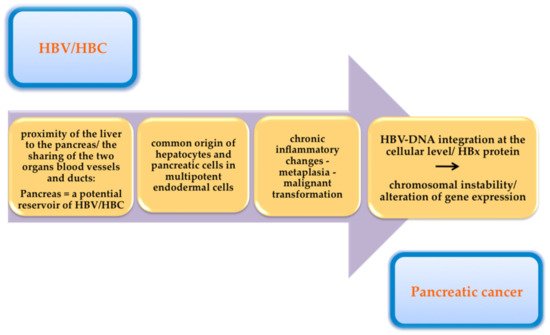
4. Conclusions
References
- Mizrahi, J.D.; Surana, R.; Valle, J.W.; Shroff, R.T. Pancreatic cancer. Lancet 2020, 395, 2008–2020.
- Huang, J.; Lok, V.; Ngai, C.H.; Zhang, L.; Yuan, J.; Lao, X.Q.; Ng, K.; Chong, C.; Zheng, Z.-J.; Wong, M.C. Worldwide Burden of, Risk Factors for, and Trends in Pancreatic Cancer. Gastroenterology 2021, 160, 744–754.
- Naudin, S.; Viallon, V.; Hashim, D.; Freisling, H.; Jenab, M.; Weiderpass, E.; Perrier, F.; McKenzie, F.; Bueno-De-Mesquita, H.B.; Olsen, A.; et al. Healthy lifestyle and the risk of pancreatic cancer in the EPIC study. Eur. J. Epidemiol. 2020, 35, 975–986.
- Klein, A.P. Pancreatic cancer epidemiology: Understanding the role of lifestyle and inherited risk factors. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 493–502.
- Gheorghe, G.; Bungau, S.; Ilie, M.; Behl, T.; Vesa, C.M.; Brisc, C.; Bacalbasa, N.; Turi, V.; Costache, R.S.; Diaconu, C.C. Early Diagnosis of Pancreatic Cancer: The Key for Survival. Diagnostics 2020, 10, 869.
- Ghiorzo, P. Genetic predisposition to pancreatic cancer. World J. Gastroenterol. 2014, 20, 10778–10789.
- Vincent, A.; Herman, J.; Schulick, R.; Hruban, R.H.; Goggins, M. Pancreatic cancer. Lancet 2011, 378, 607–620.
- Solomon, S.; Das, S.; Brand, R.; Whitcomb, D.C. Inherited pancreatic cancer syndromes. Cancer J. 2012, 18, 485–491.
- Olson, S.H.; Kurtz, R.C. Epidemiology of pancreatic cancer and the role of family history. J. Surg. Oncol. 2013, 107, 1.
- Shindo, K.; Yu, J.; Suenaga, M.; Fesharakizadeh, S.; Cho, C.; Macgregor-Das, A.; Siddiqui, A.; Witmer, P.D.; Tamura, K.; Song, T.J.; et al. Deleterious Germline Mutations in Patients With Apparently Sporadic Pancreatic Adenocarcinoma. J. Clin. Oncol. 2017, 35, 3382.
- Duell, E.J.; Lucenteforte, E.; Olson, S.H.; Bracci, P.M.; Li, D.; Risch, H.A.; Silverman, D.T.; Ji, B.T.; Gallinger, S.; Holly, E.A.; et al. Pancreatitis and pancreatic cancer risk: A pooled analysis in the International Pancreatic Cancer Case-Control Consortium (PanC4). Ann. Oncol. 2012, 23, 2964.
- Bang, U.C.; Benfield, T.; Hyldstrup, L.; Bendtsen, L.; Beck, J.F. Mortality, cancer, and comorbidities associated with chronic pancreatitis: A Danish nationwide matched-cohort study. Gastroenterology 2014, 146, 989.
- Ekbom, A.; McLaughlin, J.K.; Karlsson, B.M.; Nyren, O.; Gridley, G.; Adami, H.O.; Fraumeni, J.F. Pancreatitis and pancreatic cancer: A population-based study. J. Natl. Cancer Inst. 1994, 86, 625.
- Liu, Q.; Guo, L.; Zhang, S.; Wang, J.; Lin, X.; Gao, F. PRSS1 mutation:a possible pathomechanism of pancreatic carcinogenesis and pancreatic cancer. Mol. Med. 2019, 24, 44.
- Shi, Z.; Wei, J.; Na, R.; Resurreccion, W.K.; Zheng, S.L.; Hulick, P.J.; Helfand, B.T.; Talamonti, M.S.; Xu, J. Cystic fibrosis F508del carriers and cancer risk: Results from the UK Biobank. Int. J. Cancer 2021, 148, 1658–1664.
- Pergolini, I.; Sahora, K.; Ferrone, C.R.; Morales-Oyarvide, V.; Wolpin, B.M.; Mucci, L.A.; Brugge, W.R.; Mino-Kenudson, M.; Patino, M.; Dushyant, V.S.; et al. Long-term Risk of Pancreatic Malignancy in Patients With Branch Duct Intraductal Papillary Mucinous Neoplasm in a Referral Center. Gastroenterology 2017, 153, 1284.
- Pereira, S.P.; Oldfield, L.; Ney, A.; Hart, P.A.; Keane, M.G.; Pandol, S.J.; Li, D.; Greenhalf, W.; Jeon, C.Y.; Koay, E.J.; et al. Early detection of pancreatic cancer. Lancet Gastroenterol. Hepatol. 2020, 1253, 30416–30419.
- Lanini, S.; Ustianowski, A.; Pisapia, R.; Zumla, A.; Ippolito, G. Viral Hepatitis: Etiology, Epidemiology, Transmission, Diagnostics, Treatment, and Prevention. Infect. Dis. Clin. N. Am. 2019, 33, 1045–1062.
- Lin, C.L.; Kao, J.H. Natural history of acute and chronic hepatitis B: The role of HBV genotypes and mutants. Best Pract. Res. Clin. Gastroenterol. 2017, 31, 289–294.
- Mikulska, M.; Lanini, S.; Gudiol, C.; Drgona, L.; Ippolito, G.; Fernandez-Ruiz, M.; Salzberger, B. ESCMID Study Group for Infections in Compromised Hosts (ESGICH) Consensus Document on the safety of targeted and biological therapies: An infectious diseases perspective (Agents targeting lymphoid cells surface antigens : CD19, CD20 and CD52). Clin. Microbiol. Infect. 2018, 24, S71–S82.
- Dandri, M.; Locarnini, S. New insight in the pathobiology of hepatitis B virus infection. Gut 2012, 61, i6–i17.
- Poynard, T.; Ratziu, V.; Charlotte, F.; Goodman, Z.; McHutchison, J.; Albrecht, J. Rates and risk factors of liver fibrosis progression in patients with chronic hepatitis C. J. Hepatol. 2001, 34, 730–739.
- Zhou, Y.; Zhao, Y.; Li, B.; Huang, J.; Wu, L.; Xu, D.; Yang, J.; He, J. Hepatitis viruses infection and risk of intrahepatic cholangiocarcinoma: Evidence from a meta-analysis. BMC Cancer 2012, 12, 289.
- Jeong, S.H. HBV infection as a risk factor for non-Hodgkin lymphoma. Lancet Oncol. 2010, 11, 806.
- Fiorilli, M.; Mecucci, C.; Farci, P.; Casato, M. HCV-associated lymphomas. Rev. Clin. Exp. Hematol. 2003, 7, 406–423.
- Tian, T.; Song, C.; Jiang, L.; Dai, J.; Lin, Y.; Xu, X.; Yu, C.; Ge, Z.; Ding, Y.; Wen, Y.; et al. Hepatitis B virus infection and the risk of cancer among the Chinese population. Int. J. Cancer 2020, 147, 3075–3084.
- Xu, J.H.; Fu, J.J.; Wang, X.L.; Zhu, J.Y.; Ye, X.H.; Chen, S.D. Hepatitis B or C viral infection and risk of pancreatic cancer: A meta-analysis of observational studies. World J. Gastroenterol. 2013, 19, 4234–4341.
- Yan, F.M.; Chen, A.S.; Hao, F.; Zhao, X.P.; Gu, C.H.; Bin Zhao, L.; Yang, D.L.; Hao, L.J. Hepatitis C virus may infect extrahepatic tissues in patients with hepatitis C. World J. Gastroenterol. 2000, 6, 805–811.
- Mason, A.; Wick, M.; White, H.; Perrillo, R. Hepatitis B virus replication in diverse cell types during chronic hepatitis B virus infection. Hepatology 1993, 18, 781–789.