Augmented, Virtual and Mixed Reality can represent a useful aids for Dentistry. Augmented Reality can be used to add digital data to real life clinical data. Clinicians can apply Virtual Reality for a digital wax-up that provides a pre-visualization of the final post treatment result. In addition, both these technologies may also be employed to eradicate dental phobia in patients and further enhance patient’s education. Similarly, they can be used to enhance communication between the dentist, patient, and technician. Artificial Intelligence and Robotics can also improve clinical practice. Artificial Intelligence is currently developed to improve dental diagnosis and provide more precise prognoses of dental diseases, whereas Robotics may be used to assist in daily practice.
1. Introduction
Currently, dentistry is benefiting from the development of modern digital transformation. Three-dimensional (3D) digital technology as well as computer-aided design and computer-aided manufacturing represent modern-day dentistry
[1]. Nevertheless, innovations have been introduced in the dental field to improve dental education and clinical activity. Augmented Reality (AR) and Virtual Reality (VR) represent some of these innovations (
Figure 1) and are part of the reality–virtuality continuum
[2]. Commonly, traditional digital technologies in dentistry are structured into a three-step procedure which can be summarized as follows: (1) the digital image is acquired by a scanning device; (2) the operator can modify or change different dental aspect digitally, such as position or orientation of teeth; (3) the new information is transferred back to solid state or remain digital as a wax-up. With the introduction of AR and VR, these steps are simplified and implemented
[3][4][3,4]. Although AR and VR possess many common aspects, the outcomes and the users’ experience are completely different.
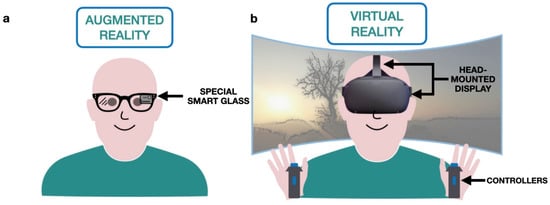
Figure 1. Illustrations of two examples of Augmented Reality (AR) and Virtual Reality (VR). (a) AR: the user sees the digital information superimposed with the reality by special smart glass (black arrow). (b) VR: the user is completely immersed in a virtual environment by head-mounted display (black arrows) and can interact with it using specific controllers (black arrow).
AR and VR systems require essential functionalities such as real and virtual data sources, tracking, registration techniques, visualization processing, perception locations, display types, and feedback mechanisms
[5]. Instead of VR, AR generates an interaction between the real environment and virtual objects with the aim to combine virtual and real objects in a single real environment, to run interactively, and to register virtual and real objects reciprocally
[6].
Monitor-based interfaces, monocular systems, head-mounted displays and other combined technologies are the instruments commonly used in AR systems. AR is mainly devoted to clinical practice in the medical field and improves the clinical procedure because it can allow clinical information to be visualized directly on the patient, overlapping the digital information and the real world
[7]. In dentistry, the principal application of AR is related to overlapping digital information on the real world, basically “improving the reality” and live communication systems between patients and collaborators through the sharing of images, videos, and 3D models.
Conversely, VR uses customized and advanced software and hardware to create a digital 3D reality in which all user’s senses are stimulated with computer-generated sensations and feedbacks. VR, therefore, allows participants to experience simulated digital realities similar to those of physical reality, thus creating scenarios that are impossible to experience in the real world
[8]. VR differs from AR in three basic systems: scene generator, a display device, and tracking and sensing. In VR, the display and scene generator is employed to simulate the real world; thus, the resolution of the monitor becomes vital for real-time interaction with the virtual world, allowing the user to be immersed in a digital-built reality
[9]. Moreover, the user can use a specific device to interact with the virtual reality as a joystick and complex haptic systems (force feedback). VR applications are already in use in the dental field and mainly concern dental training: they allow students to simulate procedures in a virtual mouth, providing direct and immediate feedback.
In addition to AR and VR, Mixed Reality (MR) represents an innovative tool for use in dentistry. Despite MR being often confused with AR, it is a combination of AR and VR. In MR, users can interact with both virtual and real objects in real-time, while simultaneously, these objects can interact with each other. This “environment awareness” implies that not only do virtual objects act in the real environment, but real objects can also modify the virtual elements, regardless of where the experience is taking place
[2]. For instance, in pure MR, users would not be able to see a virtual instrument inside a drawer, unless they open it to look inside; in AR, the instrument would be overlaid, and it would be unnecessary to open the drawer.
Innovations such as AI and Robotics are being introduced in the dental field. Whilst AR, VR and MR enhance and create new realities, AI and Robotics perform and replicate human tasks. Artificial Intelligence (AI) revolves around its own intelligence, concerned in algorithm, to solve problems based on learning a specific set of data. Robotics focuses on the reproducibility of different clinical procedures. The use of these new systems could improve the way to perform the clinical training at dental schools and improve clinical practice, increasing the possibility of achieving better reproducible results in less time. At the best of authors’ knowledge, there is no literature review that summarizes these novelties and their potential dental applications.
2. Applications in Teaching Dental Morphology
The study of anatomy is commonly performed by using static two-dimensional (2D) images such as lecture slides, textbooks and flashcards
[10][12]. Since anatomical structures are in three-dimensions (3D), the comprehension of spatial relationships using such static 2D images may be difficult.
Through 3D virtual models, different anatomical structures may be visualized, making the learning experience more immersive than the traditional 2D and 3D methods
[11][13]. The exploration of a virtual environment may help to develop spatial knowledge, reducing the gap between students who struggle to visualize spatial structures and those confident in their spatial ability
[12][14]. In addition, Küçük et al. highlighted that dental students appear more interested in learning anatomical structures through a 3D model than through traditional 2D methods
[13][15].
AR and VR may also be used to learn dental morphology and tooth features such as exterior shape, position, size and internal structure. Basing on software programs with interactive data set, the tooth can be selected, moved and visualized from different directions and angulations. Moreover, specific tooth structures can be made transparent such that the users can see beyond them or even navigate through the root canal. Reymus et al. tested the use of VR in teaching root canal anatomy and found that VR appears to be a valuable instrument suitable for training a student
[14][16]. Thus, both VR and AR may be considered valuable platforms for teaching anatomy and promoting benefits such as increased learner immersion, even if there are no statistically significant differences regarding the amount of knowledge acquired by VR/AR and the traditional method
[14][16].
3. Applications in Pre-Clinical Education
A significant proportion of dental education is dedicated to teaching clinical psychomotor skills, and often, the dentist trains directly on the patient
[15][17]. Currently, dental schools use realistic patient simulators with dental models incorporated to simulate a dental treatment
[16][18]. These simulators allow the instructors to demonstrate techniques aimed at improving the hand-eye coordination and manual dexterity of students. Moreover, during the activities on the simulators, dental students require constant tutor feedback on their work for understanding better the procedures before moving on to the subsequent procedures.
During the COVID-19 pandemic, limitations in pre-clinical education have been highlighted, as many dental students could not be trained at their university and lacked the direct support of the tutor. In this COVID-19 era, the most important issue for pre-clinical and clinical education is achieving the balance between the training of dental students and limiting the spread of infected cases
[17][18][19,20]. It is for this reason, because of the development of innovative instruments to train and teach the basic clinical procedures to the dental students, that replicating dental reality as much as possible became of paramount importance.
Considering these aspects, AR, VR and MR represent innovative educational tools which allow self-education of the student. While the description of the tactile sensation of clinical procedures by the tutor may be difficult to explain using the traditional simulator, the presence of direct feedback and pressure sensors may be useful to overcome this problem by using VR or MR
[19][21]. In a previous study by Eve et al., the performance on a simulated caries removal of undergraduate dental students was compared to prosthodontics residents using a novel haptic VR simulator
[20][22]. Their results showed that efficiency, defined as percentage of carious lesion removed over drilling time, improved significantly over the experiment for both novice and experienced operators
[20][22]. In addition, De Boer et al. examined the use of VR in dental education and highlighted a significant positive effect on the student performance and the appreciation of the 3D environment compared to 2D
[21][23].
Similar to traditional simulators, VR or MR simulators provide digital teeth models, digital handpieces equipped with an air and water in-and-out system and different types of digital burs. In addition, these simulators may provide instant feedback for the students making full use of the lab training time and improving students’ manual dexterity skills before confidently moving onto clinical setting with patients.
Table 1 summarizes and compares different dental simulators currently used
[19][21].
Table 1. Comparison of different dental simulators.
| |
PerioSim | ® |
Dentsim™ |
IDEA |
Simodont | ® |
Voxel Man |
CDS |
| Teeth Used |
Animated |
Plastic teeth |
Animated |
Animated |
Animated |
Animated |
| Right And Left |
| Operation |
Available |
Available |
Available |
Available |
Available |
Available |
| Reported Real Life |
| Experience |
Tactile
sensation is
realistic for
teeth but not for gingiva |
Realistic
experience
using plastic
teeth on a real
manikin |
Tactile
sensation still
needs to be
tuned to
simulate a
genuine
sensation |
3D images are
realistic. However,
the texture of healthy
decayed and restored
tooth structure still
needs improvement |
/ |
/ |
| Ergonomic Postures |
No |
Yes |
No |
Yes |
No |
Yes |
| Direct Transfer of Data to Program Instructor/Tutor |
Not available |
Yes
Run time control. Application enables the instructor to control run time grades. |
Yes
The software
contains a
replay mode.
Upon
completion of a specified task, it
can be watched
in full by the
student or the
instructor. |
Yes
Allows the instructor to
watch six simulators
live at once and
record all
preparations for
evaluation in order to give
feedback later. |
Not available |
Yes
Operating procedures are recorded and can be reviewed to facilitate in training, grading and verifying. |
| Instant Feed Back |
No |
Yes |
Yes |
Yes |
Yes |
Yes |
| Exam Simulation |
Yes |
Yes |
No |
Yes |
Yes |
Yes |
4. Applications in Clinical Practice
The medical applications of AR are currently concentrated on different surgery types, including neurosurgery, laparoscopic surgery, and plastic surgery. In dentistry, AR is primary used in oral and maxillofacial surgery, dental implant placement and orthognathic surgery
[22][24]. The development of AR devices allows the user to combine the medical information, medical data, and images to the reality. In contrast to conventional image-guided surgery, where a surgeon often looks away from the operative field to view the informative data, AR guidance systems provide real-time intraoperative information directly on the surgical fields and this may decrease the surgical risk
[23][25].
In dental implant placement, AR has been shown to substantially improve a wide range of procedures. A dental implant positioning system with a graphically superimposed suggested position on the patient was introduced as early as 1995. The AR surgical navigation systems for implant placement were introduced using retinal imaging display such that the surgeon maintains the view of the operative field without looking away
[24][26]. During implant placement, AR can act as automatic information filters that selectively display only the most relevant information to surgeons, thereby helping them concentrate fully on the implant placement thereby reducing time and additional costs
[25][27].
Orthognathic surgery is one of the most widely used fields of AR applications in dentistry. The most important advantage of AR-based navigation systems for orthognathic surgery is the possibility to provide overlaid images of real surgical views and virtual surgical plans for guidance. The systems overlay these models onto real-time streaming video images to provide surgeons with preoperative planning and anatomical information. Different AR-based systems were introduced for the simulation of the reduction of mandibular angle and the simulation of the mandibular reconstructive surgery
[26][27][28][28,29,30]. Innovative systems were also developed to simulate mandibulectomy and fibular transplant to the mandibular defect site using 3D patient mesh models. In addition, it allowed surgeons to test and find configurations of vessels and skin paddles
[29][31]. Kim et al. used an AR-system to display overlaid images to allow surgeons to follow virtual surgical plans when repositioning patient bones after maxillofacial osteotomies
[30][32].
Even VR was applied in orthognathic surgery in order to train different procedures of orthognathic maxillofacial surgery. To better simulate the surgical procedures the VR system can include and replicate different functions such as bone sawing, drilling, and place fixation with haptic force feedback
[26][31][28,33]. Moreover, in another VR-based simulation platform, the surgeon can interact with the virtual world naturally using his or her hands by means of a tracked hand-held controller
[32][34].
5. Applications in Dental Phobia
It is estimated that 50–60% of individuals suffer from a specific fear of dental procedures and dental-related stimuli, or from a mild to severe grade of dental anxiety
[33][34][35,36]. Fear-related behaviours are considered the most difficult aspect of dental patient management and may interfere with good dental care since the patient with dental phobia (named “odonto-phobia”) goes to the dentist when the clinical situation is severe. The therapeutic techniques, considered most effective in the treatment of phobias and fears, are the In Vivo Exposure Therapy (IVET) and the Virtual Reality Exposure Therapy (VRET). IVET is a technique based on direct patient confrontation with an object or series of anxious situations to reduce the consequent anxious reaction. This exposure therapy is considered the gold standard therapy in the treatment of specific fears related to the dental care situation
[35][37]. Recently, VRET has become a viable alternative to IVET in the treatment of specific phobias
[36][38]. Using computer-generated VR environments, the patient is gradually exposed to situations which are potentially sources of anxiety
[37][39]. Compared to IVET, VRET is safer because the patients face the virtual representation of their threat more gradually in a controlled manner
[38][40]. VRET is known to elicit a feeling of being “present” in the virtual environment, and this represents the main factor for the effectiveness of VRET
[39][41]. Clinically, techniques such as cognitive–behavioural treatments, nitrous oxide, and intravenous sedatives administered during dental treatments have been found to minimize patient pain and discomfort during dental care
[40][41][42,43]. In addition to these invasive methods, distracting patients with a movie has been shown to help reduce pain in some medical procedures and during laboratory studies of pain
[42][44]. Following the same concept, VR can serve as an effective non-pharmacologic analgesic for dental pain
[43][45]. Several studies reported that VR reduced their awareness of dental pain and that they were so absorbed in the VR that they did not think often about their pain
[44][45][46][46,47,48]. The patient’s inability to see the dental practitioner and instruments may be one advantage of VR. The effectiveness of VR distraction treatment may depend on how patients feel in the virtual environment
[47][49]. For this reason, video stimulation and audio simulation may be detrimental in making the users’ experience more immersive and by trying to decrease the dental pain
[8]. For VR application, it is advisable to produce sound in three dimensions, specifically in the binaural format.
The audio in three dimensions allows the users to hear the sound of objects according to their position in the virtual space. The use of the binaural format, which reproduces the immersive audio with simple headphones, without the aid of a complex hardware set up, will create a greater reality of the VR environment
[8]. Consequently, the effectiveness of VR in distracting the patient from medical treatment will be greater. Hendrix et al. confirmed that 3D sound increases people’s sense of immersion in virtual reality
[48][50]. The study showed that people felt more immersed in virtual realities with spatial sound than in virtual realities with non-spatial sound
[48][49][50,51]. Moreover, the soundtrack in an immersive audio, more than the stereo format, increases the possibility of modifying the patient’s state of mind. Therefore, an adequate sonorization of the VR environment will favour a state of calm and relaxation.
6. Applications in Patient Education
Educational and motivational methods play an important role in informing individuals about their oral health status, including oral pathologies that affect oral tissues, thus helping to enhance their compliance with oral care at home. In particular, oral health education is effective in improving patient’s attitude and practice of oral hygiene, providing useful devices and techniques for dental plaque control, which may promote gingival health and decrease caries occurrence
[50][51][52,53].
AR and VR can be considered important tools to educate old and young patients. The expected outcome in using VR and AR for oral home care is to provide a digital instrument to improve oral hygiene practice in children and adults, motivating the prevention of oral diseases and making educational practices attractive. Moreover, by using games or educational interfaces, VR and AR may become important accessories in the process of teaching and learning. Although few articles reported the application of VR in patient education, it seems to be an engaging learning tool, and patients who participated in the studies perceived it to be beneficial in understanding their health status
[52][53][54,55]. Mainly in children, the advantage in using a game consists on: whenever the player executes the brushing technique incorrectly, the system provides a visual response which allows the patient to correct the brushing technique. However, further efforts to investigate the role of VR in education and oral health care should be explored in the future.
7. Dentist–Patient Communication Tools
Clinicians use several tools to collect different data in order to formulate the correct functional and aesthetic treatment plan such as
[54][56]: physical examination, radiographs, study models, intraoral and extraoral photographs. Once the diagnosis has been made, the patient must be informed of the chosen therapeutic modalities, based on his clinical situation and on evaluating psychological and socio-economic aspects. Nevertheless, many patients may not have the necessary knowledge to understand the concepts illustrated for the treatment plan and the condition of their oral cavity; thus, it may be difficult for the dentist to persuade the patient to accept the proposed therapeutic option.
In this light, digital dentistry has led to the development of many innovative technologies that can aid the dentist in communicating with the patient; for example, the spread of digital technology has simplified the step of creating a set of facial and intraoral photographs, both in the production phase of the images and in their archiving. In addition to communication purposes, this allows the dentist to analyse the patient even after the actual visit, exchanging information with the dental laboratory and with colleagues who may participate in the execution of the therapies
[55][57]. Currently, different devices can be used to improve such patient–operator communication, as diagnostic and virtual wax-up allow for the visualization of the possible prosthetic treatment.
Predicting outcomes of the therapy offers many advantages in terms of communication, design and economics. Providing an image in which the result is represented may improve the relationship of trust with the patient and simplify the transmission of the necessary data to the dental technician.
8. Artificial Intelligence and Robotics
In addition to AR and VR, new technologies, such as AI and Robotics, have been applied in dentistry to improve the clinical practice
[56][58]. AI is the ability of a machine to perform human tasks and revolves around its own intelligence to solve problems based on the learning of a specific set of data. AI refers to any machine or technology that can mimic human cognitive skills such as problem solving. The foundation of AI is to increase the ability of machines or its intelligence components to perform tasks with speed, low resources, accuracy, and precision. Machine learning is part of AI, which depends on algorithms to predict outcomes based on a dataset
[57][59]. Algorithms are artificial neural networks, highly interconnected networks of computer processors inspired by biological nervous systems that function similarly to the human brain
[58][60].
The most active areas of medical AI are diagnostics and prediction of prognoses. AI in the medical sector contributes significantly to helping decision making related to medical practice, while presenting a considerable level of potential for sound diagnosis and prediction
[59][60][61,62]. It was proven that machine learning, based on data derived from the decisions of dental professionals, achieved significant performance
[61][63]. For example, different studies intended to generate caries prediction models to facilitate the likelihood calculation of an individual developing dental caries based on clinical findings or demographic and lifestyle factors
[61][62][63,64]. Another important feature is data mining, whose strength lies in the ability of finding causal relationships and comparisons that are innate in existing data
[63][65]. The observations were obtained by data mining analysis, while the only role of dental professional was to collect and tabulate the data.
All the above studies proved the application of AI in the current dental field to diagnose and make prognoses through extrication of useful information from large amounts of medical records
[63][65]. Again, data mining analysis performed on a bulk of restorative data of patients revealed that differences in the material of dental restorations serve as important factors determining the lifespan of a restoration
[64][66]. Currently, studies applying machine learning based on artificial neural networks to dental treatment through analysis of dental magnetic resonance imaging, computed tomography, and cephalometric radiography are actively underway. AI-based systems are often used for designing software programs that try to simplify data management and diagnosis in dentistry. Mostly, they are clinical decision support systems that assist and guide experts to make better decisions
[65][67] and aesthetic mock-up
[66][68].
AI-based systems have been used for better diagnosis, treatment planning and for prognosis prediction. AI in dentistry started procuring its role with emergence of data computation and availability of large amounts of patient data. For instance, the information acquired by radiological exam can be analysed by an algorithm which may improve and help the diagnosis and treatment phases of oral pathology and disease in an automatic way
[63][65]. Additionally, AI technology has demonstrated excellent results in the detection of dental caries
[67][68][69,70], diagnosing oral squamous cell carcinoma
[69][71], and evaluation of the correct working length in endodontics
[70][71][72][72,73,74].
In adjunct to AI, robotics can represent the next frontier of dentistry. Robotics has been added to medicine since 1992, but only in 2001, a human-controlled robot, remotely located, was able to remove a dental caries, perform an endodontic treatment and execute a crown and bridge preparation
[73][75].
In 2017, Yuan et al. demonstrated that robots’ tooth preparation skills, such as laminate veneer and crowns preparations, are as accurate as those of human dentists
[74][76]. Recently, a mobile wire-bending machine was introduced, which is capable of creating a fixed orthodontic retainer wire by means of intraoral scan data in only four minutes
[75][77]. Another remarkable opportunity enabled by robotics is computer-assisted surgery. Using this approach, a navigation system may track the position of a surgical device in real time. The guidance to the dentist is realized by the device position projecting onto the digital image of the anatomic area of interest, providing help in real-time to follow the anticipated pathways and allowing the doctor to recognize possible interference with the neighbouring tissues. Currently, the most commonly used optical tracking systems are based on capturing the position of a series of light-emitting diodes mounted on a surgical device
[75][77]. In the future, virtual robotic surgery will allow surgeons to operate patients in a different location.