The formulation of an ideal vaginal drug delivery system (DDS), with the requisite properties, with respect to safety, efficacy, patient compliance, aesthetics, harmonization with the regulatory requirements, and cost, requires a meticulous selection of the active ingredients and the excipients used. Novel excipients defined by diversity and multifunctionality are used in order to ameliorate drug delivery attributes. Synthetic and natural polymers are broadly used in pharmaceutical vaginal formulations (solid, semi-solid dosage forms, implantable devices, and nanomedicines) with a promising perspective in improving stability and compatibility issues when administered topically or systemically. Moreover, the use of biopolymers is aiming towards formulating novel bioactive, biocompatible, and biodegradable DDSs with a controllable drug release rate.
- novel vaginal excipients
- co-polymers
- mucoadhesive
- bio-adhesive
- thermosensitive
- vaginal drug delivery
- novel vaginal formulations
- vaginal films
- vaginal nanomedicines
- drug release
1. Introduction
2. Anatomy and Physiology of the Vagina
The vagina is located in women between the rectum, the urethra, and the bladder. It is a thin-walled fibromuscular tube that is extending from outside the body to the cervix [2][3][4]. The dimensions of the vagina are crucial factors that affect drug administration and are characterized by an interindividual variability, which is modified in an age-related manner. Thus, its average length in women of reproductive age is 6–8 cm for the front wall and up to 14 cm for the back wall, including the length of the cervix [5]. Moreover, the average vaginal surface area is calculated to be ca. 87.46 cm2 (range: 65–107 cm2) [6] and is significant for the absorption of administered active substances [7]. There are four distinct anatomical regions, which are observed in the lower part of the female genital tract: the introitus (covered by a keratinized epithelium), the vaginal epithelium (covered by a non-keratinized stratified squamous epithelium), the ectocervix, (covered by a mucosal layer), and the endocervix (columnar epithelium with numerous glands) [2][3][4]. The physiological cervical stratified squamous epithelium is formed by distinct layers of epithelial cells, which can be classified into different classes based on the stage of maturation: basal, parabasal, intermediate, and superficial. Throughout maturation, various cells from the basal layer move gradually towards the superficial layer, obtaining a flatter shape. However, superficial layers of the cervix, which are closer to the vaginal lumen, are mainly characterized by tight junctions [8]. Furthermore, the thickness of cervical squamous epithelium is variable (0.2–0.5 mm) and is directly related to age. After menopause, cytoplasmic volume condensation and epithelium atrophy is observed [9]. It is essential that the structure of the epithelium is considered as the crucial site for the most effective and targeted drug delivery of the active substances, the permeability and solubility properties of which determine the final drug delivery efficacy (topical or systemic action) across these tissues and the toxicity profile [8].3. Vaginal Drug Delivery
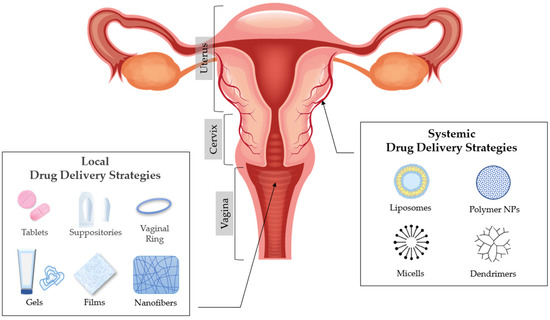
The anatomy and physiology of the vagina can affect and provoke challenges in achieving local or systemic drug delivery [8][10]. The most common drugs that are usually administered in the vagina are related to the treatment of vaginal infections (antimicrobials/antifungal), spermicides or contraceptive agents, and active ingredients related to hormone replacement therapy, induction of labour, and interruption of pregnancy [11][12]. There is a plethora of formulations used for vaginal administration including solid dosage forms (suppositories and tablets), semisolids (creams and gels) and other forms such as intravaginal rings, films and foams [13]. Several advantages are provided by vaginal (DDSs) [2][12][14][15]. The vaginal route is easy and convenient due to the simple administration of the formulations. It is an accessible and non-invasive route, since it does not cause tissue damage and potential infections related with parenteral administration. Moreover, drugs which have a systemic action and are administered vaginally are easily absorbed due to vaginal high vascularity, which allows adequate blood supply and, consequently, they do not undergo from hepatic first pass metabolism [8][16]. Vaginal administration also minimizes many side effects which can be provoked by oral and parenteral drugs, such as those affecting the gastrointestinal tract and liver [16]. Other absorption pathways that can occur through this route are passive diffusion and active transportation, which are defined by permeability and absorption characteristics, such as the molecular weight (MW), the extent of ionization, the lipophilicity, and the dissolution properties of active substances [10]. Another significant advantage of the vaginal route drug administration is the specialized local effect of the drug when treating infections or preventing sexually transmitted diseases of the female reproductive system.4. Factors That Affect Drug Absorption in Vaginal Epithelium
Physiologically, the vagina generates several obstacles in drug delivery due to its variability in potential structural form, which can affect the acceptability and the administration of certain vaginal formulations [10]. These variations are crucial to be considered from the pharmacological point of view, since drug administration and absorption are directly related with the physiology of the vagina. These factors are cervical mucus, vaginal epithelium thickness, fluid, microflora, enzymatic activity, and pH [7] (Figure 1).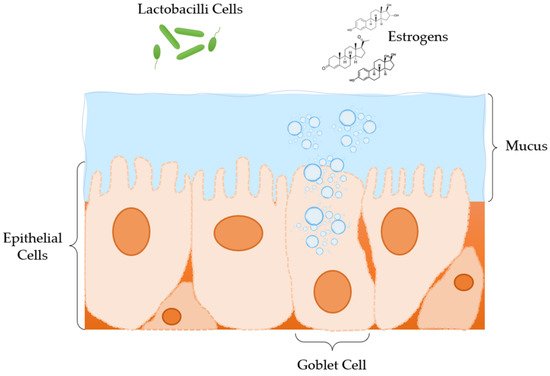
5. Excipients Used in Modified Drug Release Pharmaceutical Dosage Forms for Vaginal Administration
5.1. Excipients Used in Matrix Tablets for Vaginal Administration
5.2. Excipients Used in Solid Dosage Forms for Vaginal Administration: Ovules and Vaginal Suppositories
Scientists have also explored alternatives to vaginal tablets. Ovules and vaginal suppositories have been formulated for topical delivery. The formulation of such products requires a base (oily/emulsifying/aqueous), where the API will be placed in, and in some cases antioxidants and/or preservatives are also used [15]. The composition of the suppository base has an important role in drug release rate and extent.5.3. Excipients Used in Semi-Solid Dosage Forms for Vaginal Administration: Gels
Gels are semisolid systems that consist of two components (a liquid and a solid) [8]. When these components are homogenized, the solid component traps the liquid, creating a gelling effect and consequently producing a solid-liquid mixture. According to the polarity of the liquid component, gel systems are categorized in hydrogels, which contain a polar solvent (such as water) and organogels, where the liquid component is apolar (such as vegetable oils). Hydrogels are used in pharmaceutical industry for the administration of active substances on skin and/or mucous membranes. They are widely accepted by patients for being refreshing, hydrating, and easy in application and in removal. Therefore, their hydrophilicity creates a difficulty in drug release and consequently in absorption through the lipophilic skin barrier. As far as organogels are concerned, they outline a great ability to cross the skin barrier. However, they are not highly acceptable from patients, due to their greasy texture [35][36][37].5.4. Excipients Used in Films for Vaginal Administration
Solid and semisolid conventional vaginal dosage forms usually show a short residence time on the vaginal mucosa especially in disease condition due to added vaginal secretions. Therefore, the therapeutic effect is available only for a short period of time requiring frequent dosing and resulting in poor patient compliance. A method to overcome this, is the in situ gel forming films. Polymeric films are safe and effective and can be used for vaginal administration of various drug candidates. Vaginal film formulations require excipients such as a film former plasticizer (polymer), humectant(s), and a solvent [38].5.6. Excipients Used in Nanomedicine for Vaginal Administration
Nanoparticles (NPs) have been used as advanced DDSs due to their capability to protect therapeutic agents, their versatility to control drug release profiles and their tunable surface properties. NP encapsulation is being investigated for therapeutic applications in oral, nasal, transdermal, brain, and cardio-vascular systems as their sub-micron size allows them to penetrate into the tissue through interstitial spaces to be readily taken up by the cells. Their other advantages (modified drug release, non-toxic for the vaginal physiological environment) render them unique carriers for vaginal drug delivery [17].6. Conclusions
Topical drug delivery is site specific, leading to better patients’ compliance and to the diminution of side effects. Efficient drug delivery at the vaginal cavity is often complicated, due to its discrete physiological features. Thus, researchers have sought to develop formulation strategies using novel excipients for the successful drug delivery. Biomaterials that are biocompatible and biodegradable are suitable for the formulation of novel targeted DDSs; thus, ameliorating drug-tissue compatibility issues and drug therapeutic levels. Biomaterials have gained ground in fabricating DDSs, enhancing and optimizing drug release rate, by targeting to controlled-release or time-dependent release rate. Materials that show a diversity in pH response, swelling and bioadhesive properties, similar to vaginal epithelium, along with low toxicity effects, have a significant impact on the design of multifunctional pharmaceutical formulations. To this end, several biocompatible polymers, such as chitosan, hydroxypropylmethylcellulose, methacrylic acid co-polymers, polyethylene oxide, polylactic-co-glycolide, etc., have been employed to promote mucoadhesiveness, and therefore drug release, with very promising results.References
- Kar, M.; Chourasiya, Y.; Maheshwari, R.; Tekade, R.K. Current Developments in Excipient Science: Implication of Quantitative Selection of Each Excipient in Product Development. In Advances in Pharmaceutical Product Development and Research, Basic Fundamentals of Drug Delivery; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 29–83.
- Alexander, N.J.; Baker, E.; Kaptein, M.; Karck, U.; Miller, L.; Zampaglione, E. Why consider vaginal drug administration? Fertil. Steril. 2004, 82, 1–12.
- Forsberg, J.G. A morphologist’s approach to the vagina. Acta Obstet. Gynecol. Scand. Suppl. 1996, 163, 3–10.
- Sjoberg, I. The vagina: Morphological, functional and ecological aspects. Acta Obstet. Gynecol. Scand. Suppl. 1992, 71, 84–85.
- Pendergrass, P.B.; Reeves, C.A.; Belovicz, M.W.; Molter, D.J.; White, J.H. The shape and dimensions of the human vagina as seen in three-dimensional vinyl polysiloxane casts. Gynecol. Obstet. Investig. 1996, 42, 178–182.
- Pendergrass, P.B.; Belovicz, M.W.; Reeves, C.A. Surface area of the human vagina as measured from vinyl polysiloxane casts. Gynecol. Obstet. Investig. 2003, 55, 110–113.
- Veiga, M.; Ruiz-Caro, R.; Mart, A. Polymer Gels in Vaginal Drug Delivery Systems. In Polymer Gels, Gels Horizons: From Science to Smart Materials; Thakur, V.K., Ed.; Springer: Singapore, 2018; pp. 197–246.
- Rohan, L.C.; Sassi, A.B. Vaginal drug delivery systems for HIV prevention. AAPS J. 2009, 11, 78–87.
- Walker, D.C.; Brown, B.H.; Blackett, A.D.; Tidy, J.; Smallwood, R.H. A study of the morphological parameters of cervical squamous epithelium. Physiol. Meas. 2003, 24, 121–135.
- Ferguson, L.M.; Rohan, L.C. The importance of the vaginal delivery route for antiretrovirals in HIV prevention. Ther. Deliv. 2011, 2, 1535–1550.
- Garg, S.; Vermani, K.; Kohli, G.; Kandarapu, R.; Tambwekar, K.R.; Garg, A.; Waller, D.P.; Zaneveld, L.J. Survey of vaginal formulations available on the Indian market: Physicochemical characterization of selected products. Int. J. Pharmaceut. Med. 2002, 16, 141–152.
- Vermani, K.; Garg, S. The scope and potential of vaginal drug delivery. Pharm. Sci. Technol. Today 2000, 3, 359–364.
- Garg, S.; Tambwekar, K.R.; Vermani, K.; Kandarapu, R.; Garg, A.; Waller, D.P.; Zaneveld, L.J. Development pharmaceutics of microbicide formulations. Part II: Formulation, evaluation, and challenges. AIDS Patient Care STDs 2003, 17, 377–399.
- Woolfson, A.D.; Malcolm, R.K.; Gallagher, R. Drug delivery by the intravaginal route. Crit. Rev. Ther. Drug Carr. Syst. 2000, 17, 509–555.
- Baloglu, E.; Senyigit, Z.A.; Karavana, S.Y.; Bernkop-Schnurch, A. Strategies to prolong the intravaginal residence time of drug delivery systems. J. Pharm. Pharm. Sci. 2009, 12, 312–336.
- Ozyazici, M.; Gökçe, E.; Hizarcioglu, S.Y.; Taner, M.S.; Köseoglu, K.; Ertan, G. Dissolution and vaginal absorption characteristics of metronidazole and ornidazole. Pharmazie 2006, 61, 855–861.
- Wong, T.W.; Dhanawat, M.; Rathbone, M.J. Vaginal drug delivery: Strategies and concerns in polymeric nanoparticle development. Expert Opin. Drug Deliv. 2014, 11, 1419–1434.
- Farage, M.; Maibach, H. Lifetime changes in the vulva and vagina. Arch. Gynecol. Obs. 2006, 273, 195–202.
- Burruano, B.T.; Schnaare, R.L.; Malamud, D. Synthetic cervical mucus formulation. Contraception 2002, 66, 137–140.
- Katz, D.F. Human cervical mucus: Research update. Am. J. Obstet. Gynecol. 1986, 165, 1984–1986.
- Zavos, P.M.; Cohen, M.R. The pH of cervical mucus and the postcoital test. Fertil. Steril. 1980, 34, 234–238.
- Buckheit, R.W.; Watson, K.M.; Morrow, K.M.; Ham, A.S. Development of topical microbicides to prevent the sexual transmission of HIV. Antivir. Res. 2010, 85, 142–158.
- Khanna, N.; Dalby, R.; Tan, M.; Arnold, S.; Stern, J.; Frazer, N. Phase I/II clinical safety studies of terameprocol vaginal ointment. Gynecol. Oncol. 2007, 107, 554–562.
- Khanna, N.; Dalby, R.; Connor, A.; Church, A.; Stern, J.; Frazer, N. Phase I clinical trial of repeat dose terameprocol vaginal ointment in healthy female volunteers. Sex. Transm. Dis. 2008, 35, 577–582.
- Burns, R.N.; Hendrix, C.W.; Chaturvedula, A. Population pharmacokinetics of tenofovir and tenofovir-diphosphate in healthy women. J. Clin. Pharmacol. 2015, 55, 629–638.
- Laeyendecker, O.; Redd, A.D.; Nason, M.; Longosz, A.F.; Karim, Q.A.; Naranbhai, V.; Garrett, N.; Eshleman, S.H.; Abdool Karim, S.S.; Quinn, T.C. Antibody maturation in women who acquire HIV infection while using antiretroviral preexposure prophylaxis. J. Infect. Dis. 2015, 212, 754–759.
- Marrazzo, J.M.; Ramjee, G.; Richardson, B.A.; Gomez, K.; Mgodi, N.; Nair, G.; Palanee, T.; Nakabiito, C.; van der Straten, A.; Noguchi, L.; et al. Tenofovir-based preexposure prophylaxis for HIV infection among African women. N. Engl. J. Med. 2015, 372, 509–518.
- Clark, M.R.; Peet, M.M.; Davis, S.; Doncel, G.F.; Friend, D.R. Evaluation of rapidly disintegrating vaginal tablets of Tenofovir, Emtricitabine and their combination for HIV-1 prevention. Pharmaceutics 2014, 6, 616–631.
- Sánchez-Sánchez, M.P.; Martín-Illana, A.; Ruiz-Caro, R.; Bermejo, P.; Abad, M.J.; Carro, R.; Bedoya, L.M.; Tamayo, A.; Rubio, J.; Fernández-Ferreiro, A.; et al. Chitosan and Kappa-Carrageenan vaginal acyclovir formulations for prevention of genital herpes. In vitro and ex vivo evaluation. Mar. Drugs 2015, 13, 5976–5992.
- Melnyk, G.; Yarnykh, T.; Herasymova, I. Analytical review of the modern range of suppository bases. Syst. Rev. Pharm. 2020, 11, 503–508.
- Akil, A.; Agashe, H.; Dezzutti, C.S.; Moncla, B.J.; Hillier, S.L.; Devlin, B.; Shi, Y.; Uranker, K.; Rohan, L.C. Formulation and characterization of polymeric films containing combinations of antiretrovirals (ARVs) for HIV prevention. Pharm. Res. 2015, 32, 458–468.
- Johnson, T.J.; Gupta, K.M.; Fabian, J.; Albright, T.H.; Kiser, P.F. Segmented polyurethane intravaginal rings for the sustained combined delivery of antiretroviral agents dapivirine and tenofovir. Eur. J. Pharm. Sci. 2010, 39, 203–212.
- Smith, J.M.; Srinivasan, P.; Teller, R.S.; Lo, Y.; Dinh, C.T.; Kiser, P.F.; Herold, B.C. Tenofovir disoproxil fumarate intravaginal ring protects high-dose depot medroxyprogesterone acetate- treated macaques from multiple SHIV exposures. J. Acquir. Immune Defic. Syndr. 2015, 68, 1–5.
- Srinivasan, P.; Dinh, C.; Zhang, J.; Pau, C.P.; McNicholl, J.M.; Lo, Y.; Herold, B.C.; Teller, R.; Kiser, P.; Smith, J.M. Pharmacokinetic evaluation of tenofovir disoproxil fumarate released from an intravaginal ring in pigtailed macaques after 6 months of continuous use. J. Med. Primatol. 2014, 43, 364–369.
- Rehman, K.; Mohd Amin, M.C.; Zulfakar, M.H. Development and physical characterization of polymer-fish oil bigel (hydrogel/oleogel) system as a transdermal drug delivery vehicle. J. Oleo Sci. 2014, 63, 961–970.
- Sagiri, S.S.; Singh, V.K.; Kulanthaivel, S.; Banerjee, I.; Basak, P.; Battachrya, M.K.; Pal, K. Stearate organogel-gelatin hydrogel based bigels: Physicochemical, thermal, mechanical characterizations and in vitro drug delivery applications. J. Mech. Behav. Biomed. Mater. 2015, 43, 1–17.
- Singh, V.K.; Anis, A.; Banerjee, I.; Pramanik, K.; Bhattacharya, M.K.; Pal, K. Preparation and characterization of novel carbopol based bigels for topical delivery of metronidazole for the treatment of bacterial vaginosis. Mater. Sci. Eng. C Mater. Biol. Appl. 2014, 44, 151–158.
- Acarturk, F. Mucoadhesive Vaginal Drug Delivery Systems. Recent Pat. Drug Deliv. 2009, 3, 193–205.