Self-management tools for people with chronic or persistent pain tend to focus on symptom reporting, treatment programmes or exercise and do not address barriers to work, facilitators of work ability, or workplace pain self-management strategies. Researchers developed the Pain at Work (PAW) toolkit, an evidence-based digital toolkit to provide advice on how employees can self-manage their pain at work. In a collaborative-participatory design, 4-step Agile methodology (N = 452) was used to co-create the toolkit with healthcare professionals, employers and people with chronic or persistent pain. Step 1: stakeholder consultation event (n = 27) established content and format; Step 2: online survey with employees who have persistent pain (n = 274) showed employees fear disclosing their condition, and commonly report discrimination and lack of line manager support. Step 3: online employer survey (n = 107) showed employers rarely provide self-management materials or education around managing pain at work, occupational health recommendations for reasonable adjustments are not always actioned, and pain-related stigma is common. Step 4: Toolkit development integrated findings and recommendations from Steps 1–3, and iterative expert peer review was conducted (n = 40). The PAW toolkit provides (a) evidence-based guidelines and signposting around work-capacity advice and support; (b) self-management strategies around working with chronic or persistent pain, (c) promotion of healthy lifestyles, and quality of life at work; (d) advice on adjustments to working environments and workplace solutions to facilitate work participation.
Citation:
Blake, H.; Somerset, S.; Greaves, S. The Pain at Work Toolkit for Employees with Chronic or Persistent Pain: A Collaborative-Participatory Study. Healthcare 2022, 10, 56. https://doi.org/10.3390/healthcare10010056
1. Introduction
Chronic or persistent pain affects between one-third and one-half of the population of the United Kingdom (UK), corresponding to just under 28 million adults [1]. There is unequivocal evidence that chronic pain reduces quality of life [2]. This negative impact on quality of life for people living with pain has been exacerbated by the recent coronavirus disease (COVID-19) outbreak due to changes in work-related activities, and physical inactivity during periods of confinement [3]. COVID-19 is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and was declared a pandemic in the UK by the World Health Organization (WHO) in March 2020. This pandemic has generated additional healthcare concerns for people with chronic pain due to postponed or cancelled elective surgical procedures, outpatient procedures and patient visits (including pain management services), resulting in delayed treatments, lack of continuity of care, and concerns about access to healthcare services and pain medications [4][5].
Chronic pain may impact on an individual’s ability to work [6][7][8]. Retention of people with chronic pain in the active workforce is important, since continued employment status is inversely related to pain severity [9], and extended absence from work impacts negatively on physical and mental health, as well as the economy [10][11][12]. Further, there is no conclusive evidence to support any specific tertiary-level (remedial) return to work intervention for workers with chronic pain who are already off sick [13], although it has been raised that managing pain, managing work relationships and making workplace adjustments are essential (but not straightforward) areas of a successful return for those with pain-related absence [14].
Chronic pain is considered a work-related stressor, since pain interference during the working day can impact on mood and lead to exhaustion, irrespective of pain severity [15]. For people with painful conditions, there are many employment challenges including physical limitations and ergonomics, work transitions or accommodations, stigma, the complexity of disclosure, social support at work, and the unpredictability of painful conditions or condition progression [16][17]. These are exacerbated by work-related factors such as high job demands (workload), low job control and decision authority, and low job support [18][19]. For employers, a particular challenge is not only absenteeism associated with pain [20], but the potential loss of productivity in people with chronic pain because of reduced ability at work (known as presenteeism) [21], which generates a financial burden [22][23].
There is a clear need for intervention to support people with chronic or persistent pain in the management of their condition at work for the benefit of individuals and organisations. Many organisations (particularly small to medium organisations) lack access to occupational health services for their employees. Those with access to services may lack knowledge about the impacts of chronic or persistent pain on working life. It has been proposed that occupational health and safety professionals do not necessarily have awareness, knowledge or training about chronic pain despite having involvement in the workplace management of chronic pain cases [24]. The provision of education and supportive materials for employees with chronic pain is therefore inconsistent or lacking across organisations and sectors. While educational intervention improves pain and disability in people with chronic pain of any aetiology [25][26][27], ‘patient’ targeted education tends to focus on neurophysiological aspects of pain and function and is less likely to focus on the management of the impacts of pain on working life. There is a current lack of interventions designed to assist with work-related chronic pain issues.
Further, workplace interventions for people with chronic pain tend to focus on the delivery of single approaches to self-management (e.g., exercise: [28]; strength training: [29][30]; mindfulness: [31][32][33]) and/or focus on specific painful conditions (e.g., neck pain: [34][35]; back pain: [36][37]) rather than offering comprehensive advice across a range of areas, which is suitable for employees with any pain condition. Digital technologies are increasingly used to support the self-management of chronic or persistent pain in various modalities (e.g., e-Health, m-Health, virtual reality: [38]; web-based: [39]) and have been used to improve pain or disability in a range of conditions (e.g., chronic low back pain: [40][41]; persistent musculoskeletal pain: [42]; headache: [43]. Digital interventions have potential for wide geographical reach and flexibility of access, which is particularly important given the increase in remote working and/or changes in working patterns that have occurred for many employees during (and likely following) the COVID-19 pandemic. However, existing digital interventions for people with chronic or persistent pain do not tend to address barriers to work, facilitators of work ability, or pain self-management in the context of work.
2. Research
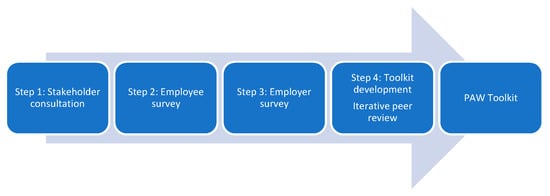
Rigorous development processes and engagement of stakeholders is essential for development of a high-quality intervention. In a collaborative-participatory design [44], we used an Agile Methodology approach as used in other published evaluations of workplace digital interventions [45][46][47], to develop a digital intervention to support people at work with chronic or persistent pain. The study took place at a higher education institution in England. Development followed a 4-step process (N = 450, FiBackgrournd : Chronic or persistent pain affects between one-third and one-half of the population of the United Kingdom (UK), corresponding to just under 28 million adults. The aim of the study was to develop an evidence-based online toolkit to provide advice on how employees with any chronic or persistent pain condition can self-manage their condition at work. Toolkit development involved co-creation activities together with an interdisciplinary stakeholder group and expert review panel with members from the public, private and third sector. To achieve the aim, the objectives of the study were to (i) consult with a wider range of stakeholders to establish content and format of the toolkit; (ii) identify employer provisions and challenges relating to supporting employees with chronic or persistent pain; (iii) identify key challenges and support needs of employees with chronic or persistent pain; (iv) conduct iterative expert peer review to complete co-creation of a final toolkit which would be appropriate for use by any employee across all organisation types and size.
Me 1
): (Step 1) a stakeholder consultation event (
thods: Rigorous development processes and engagement of stakeholders is essential for development of a high-quality intervention. In a collaborative-participatory design, we used an Agile Methodology approach as used in other published evaluations of workplace digital interventions, to develop a digital intervention to support people at work with chronic or persistent pain. The study took place at a higher education institution in England. Development followed a 4-step process (N = 450): (Step 1) a stakeholder consultation event (
= 27); (Step 2) an online survey with employees who have persistent pain (
= 274, 18–65 years); (Step 3) an online survey with employers (
= 107; 45 SMEs (Small to Medium Enterprises), 62 large organisations); (Step 4) toolkit development with iterative expert peer review (
n = 40, 13M; 27F). The 4 steps involved stakeholders from academia, healthcare and industry, as well as people with lived experience of chronic or persistent pain. Consultation activities and online survey questions were developed by the research team and were intended to inform toolkit development. Our Agile approach utilised principles of Kanban methodology [48] in which steps 1–3 produced lists of toolkit and development tasks (allowing us to draw from a backlog) and the product (the Pain at Work (PAW) toolkit) was released to reviewers with each update, enabling iterative review. The description of the toolkit aligns with the Template for Intervention Description and Replication (TIDieR) Checklist [49] (Supplementary File S1). The project team had expertise in participatory approaches for digital intervention development and Agile methodology. The study was conducted according to the guidelines of the Declaration of Helsinki and was classed as educational development and evaluation by the Research Ethics Committee of the University of Nottingham Faculty of Medicine and Health Sciences (Ref: FMHS 358-0921).
= 40, 13M; 27F). The 4 steps involved stakeholders from academia, healthcare and industry, as well as people with lived experience of chronic or persistent pain. Consultation activities and online survey questions were developed by the research team and were intended to inform toolkit development. Our Agile approach utilised principles of Kanban methodology in which steps 1–3 produced lists of toolkit and development tasks (allowing us to draw from a backlog) and the product (the Pain at Work (PAW) toolkit) was released to reviewers with each update, enabling iterative review. The description of the toolkit aligns with the Template for Intervention Description and Replication (TIDieR) Checklist). The project team had expertise in participatory approaches for digital intervention development and Agile methodology. The study was conducted according to the guidelines of the Declaration of Helsinki and was classed as educational development and evaluation by the Research Ethics Committee of the University of Nottingham Faculty of Medicine and Health Sciences (Ref: FMHS 358-0921).
Discussigon: To our knowledge, the PAW toolkit is the first accessible, digital resource to support employees at work who have chronic or persistent pain. It is publicly accessible, free to use and was developed through a rigorous, participatory design process involving surveys, consultations and peer review, engaging employees who live with chronic or persistent pain, employers and stakeholders with expertise in workplace issues and/or the management of pain. The toolkit is perceived to be relevant to employees from any size or type of organisation and addresses a clear need identified through review of evidence, stakeholder consultation and surveys with employees and employers.
Conclure 1.
Four-step Agile development process.
2.1. Step 1: Stakeholder Consultation Event
A two-hour face-to-face consultation workshop was held in February 2020, in a university medical school based within an acute hospital trust in England. Participants were identified through professional networks and purposively invited to include people with a wide range of chronic or persistent pain conditions, healthcare professionals, academics, employment advisors (including HR and occupational health), welfare and wellbeing officers, local councils, line managers, trade unions and workplace health champions. The event included a 15-min presentation delivered by a health psychologist on ‘Chronic or persistent pain at work’, including the project rationale and methodology. The facilitator had subject expertise, and prior experience of participatory design and Agile methodology. This was followed by three group activities that were based on discussion around (i) determining which groups should be consulted with regards content development and/or package dissemination, (ii) routes to technical and content development support, (iii) what format the package should take. Finally, the group were asked to review draft items developed by the project team for a brief employee and employer survey.
2.2. Step 2: Employee Survey
An online employee survey was distributed between March–April 2020, via public notices, pain charities and social media. This coincided with WHO’s declaration of COVID-19 as a pandemic in March 2020, which was followed by major pandemic-related impacts for the global workforce including a transition to remote working for a significant proportion of working-age adults. A repeat survey was released in October 2020 and left open for four months to maximise response rate (during the continuing pandemic) and capture additional workforce challenges that may have arisen during this unprecedented time. The survey platform was Jisc Online Surveys, a platform selected that meets UK accessibility requirements and is compliant with UK data protection laws. Data were collected on age, gender and employment status (employed, long-term absence from work, unemployed, retired, student). Employees were then asked to respond to three open-ended questions:
Question 1: ‘In your line of work, as someone with chronic or persistent pain, what are the biggest challenges for you in meeting your work requirements?’,
Question 2: ‘What could be done to make your work situation better? (or alternatively if you are fully satisfied, what has been done to ensure your work situation meets your needs)’,
Question 3: ‘How could/are these changes at work best provided?’.
Free-text comments were analysed using thematic analysis employing an inductive approach in which coding and theme development were driven by the content of the comments. This involved analysis of semantic content of the entire free-text data and whether comments were of a positive or negative nature. A coding taxonomy was produced for sorting qualitative data into categories of participant experience, including concerns and challenges, impacts of a global pandemic on work and pain, and employee solutions.
2.3. Step 3: Employer Survey
An online employer survey was set up using the same platform and distributed in March–April 2020, via professional networks, and social media. Data were collected on organisation size, type and sector and the primary job role of the responding individual. Participants were asked to select which supports were in place at their organisation for people who have chronic or persistent pain, such as: policies (e.g., disability), pain self-management support, education or training sessions, employee assistance programme (EAP), counselling service, mental health awareness, physical exercise, physiotherapy, occupational health service, health check-ups or medical assessments, or private healthcare. Employers were then asked to respond to three open-ended questions:
Question 1: ‘In your line of work, what are the main barriers to meeting work requirements for people with chronic or persistent pain?’,
Question 2: ‘In your line of work, what are the main ways to support people with chronic or persistent pain?’,
Question 3: ‘Can you recommend any useful resources or materials that we can use to support people with chronic or persistent pain at work?’.
Analysis of free text comments was undertaken using thematic analysis as reported in Section 2.2. For employers, comments were coded into concerns and challenges, and employer solutions.
2.4. Step 4: Toolkit Development and Expert Peer Review
Development processes included content development, a virtual peer review panel, and technical development. These processes were all undertaken virtually due to the timing of the study which occurred during the global coronavirus disease (COVID-19) pandemic. Content was compiled by the project team, which included a psychologist with expertise in health and work, a welfare officer, and a workplace health researcher. The initial draft was informed by the stakeholder consultation and findings from the employee and employer surveys. A prototype toolkit was developed as an interactive portable document format (PDF). This was considered to be the ‘minimal viable product (MVP)’ [48] and was used in the agile development process. Forty people engaged in an expert peer review panel representing academic, health care, industry and community partners. Peer reviewers were purposively selected through direct approaches from the project team to relevant departments and individuals with appropriate professional expertise, and invitation sent via pain networks, pain charities supporting people with a range of chronic pain conditions and Nottingham Pain Centre Versus Arthritis, a regional pain research centre. Panel members reviewed the toolkit content and provided feedback using a peer review form containing items adapted from the HELM Open RLO-CETL Evaluation Toolkit for Reusable Learning Objects and Deployment of E-Learning Resources (Supplementary File S2). Adopting an agile approach allowed for the provision of an MVP each time a reviewer was asked for feedback [50], e.g., after verbal or written feedback from a reviewer, revisions were made, and an updated version of the toolkit was sent to the next reviewers. The peer review form contained 10 question items, including consideration of pedagogy, format, usability, navigation, interactivity, delivery, ease of updating, distribution, and access [51]. Once peer review of content was complete, the PAW toolkit materials were transferred into Xerte, an open-source software for authoring learning objects that does not require any specific technical or programme skills. Xerte is free to download from the Xerte Community website [52].
3. Discussion
To our knowledge, the PAW toolkit is the first accessible, digital resource to support employees at work who have chronic or persistent pain. It is publicly accessible, free to use and was developed through a rigorous, participatory design process involving surveys, consultations and peer review, engaging employees who live with chronic or persistent pain, employers and stakeholders with expertise in workplace issues and/or the management of pain. The toolkit is perceived to be relevant to employees from any size or type of organisation and addresses a clear need identified through review of evidence, stakeholder consultation and surveys with employees and employers.
The development process highlighted key concerns and challenges experienced by people with pain that were recognised by employers. Many of their concerns could be modifiable with intervention or appropriate support. First, there is a clear need for awareness raising in the workplace regarding the experience of pain for some employees, their pain-related concerns, the impacts of pain on physical and mental wellbeing, and quality of working life (as well as leisure time activities). Our study highlights the need to raise awareness among managers and the working population. However, prior research has also shown the importance of continuing education on chronic pain amongst occupational safety and health professionals [24] to whom employees might turn for advice. The negative impact of chronic pain on the quality of social and working lives is already well established [2][6][7][8]. Our findings suggest that lack of knowledge and awareness of pain and disability among employers markedly increases the inequity experienced by people working with chronic pain in terms of work experiences, opportunities, career progression and work-life balance. Such issues have been discussed elsewhere [53][54][55].
Personal adjustments and workplace interventions are reported to be important determinants for staying at work [56]. However, employees are not always aware of the support they can access or approaches to help them self-manage a painful condition. The PAW toolkit addresses this gap with provision of information and supportive resources. With relation to self-management, we advocate promotion of physical and mental health at work in line with the call to action to increase awareness of effective nonpharmacologic treatments for pain [57]. These are wide-ranging, but examples include physical activity [58][59], exercise training [60], Tai Chi [61], yoga [62], pilates [63][64], nutrition and supplements [65], mindfulness meditation [31][32][66], massage therapy [67], acupuncture [68] and psychological therapies [69][70][71][72][73].
Concerns that are specific to job types or roles, or the working environment warrant discussion between employee and employer. Such concerns may be actionable but rely on disability disclosure and employee help-seeking. The PAW toolkit encourages disability disclosure and advocates help-seeking by empowering employees with knowledge about likely options and routes to support. Nevertheless, help-seeking and disability disclosure can be influenced by factors other than knowledge. There are socioeconomic, racial, ethnic and cultural discrepancies in pain beliefs, cognitions and behaviours that may impact on both disability disclosure and help-seeking behaviour [74], and this warrants further exploration.
Employees in our study reported a range of practical issues associated with specific job roles or environments, that could be addressed to some extent with appropriate assessment and intervention. For example, through modifications to activity, work or work patterns to accommodate difficulties related to function and pain while reducing activity “avoidance” (e.g., assistive technology, ergonomic assessment, regular breaks, change in scheduling, modified duties, flexible hours to attend rehabilitation or treatment). Some participants reported positive experiences of reasonable adjustments, and ergonomic assessment or occupational health referrals can be beneficial for employees with long-term conditions. However, our participants strongly advocated that occupational assessment is only meaningful to employees if recommendations are then acted upon and followed up in a timely way, which unfortunately was not common practice. Even more notable is the high proportion of employees that have no access to any form of workplace support. For example, SMEs constitute 99.9% of the UK business population [75] but smaller organisations often have less access to, or less advanced occupational health and safety services for their staff [76].
One of the most significant barriers for employees (which was recognised by employers), was a broad lack of compassion and understanding of line managers towards employees with chronic or persistent pain. While some managers struggled with managing the practical aspect of employees requiring support or periods of absence, others simply held negative attitudes towards employees with disabilities and made stigmatising or discriminatory remarks. This was perceived to be the most challenging aspect of working with long-term pain for many employees, since it fostered a negative workplace culture, and created a psychologically unsafe work environment. Psychological safety is a condition in which human beings feel (1) included, (2) safe to learn, (3) safe to contribute, and (4) safe to challenge the status quo–all without fear of being embarrassed, marginalised, or punished in some way [77]. Without psychological safety, disability disclosure is less likely. Paradoxically, employers completing our survey advocated for early disclosure, but the workplace culture and management behaviours often prohibited this. This aligns with prior research in which people with chronic pain were hesitant to disclose for fear of negative outcomes, yet employers indicate a preference for early disclosure [78].
Many participants who had disclosed their condition perceived that they were then discriminated against in the workplace, or their concerns were dismissed. Both employers and employees indicated that line managers often created obstacles for employees with long-term pain, ignored occupational health recommendations or even belittled employees for requests made. This not only has serious implications for work ability in people with chronic or persistent pain, but it exacerbates inequality in the workplace, and poses risks to career progression, as well as the physical and mental wellbeing of employees. A relationship between workplace discrimination and chronic pain has been identified previously [79][80]. In healthcare, the Institute of Medicine called for ‘a cultural transformation in the way in which pain is perceived, judged and treated’ [81] and this ethos should be transferable to the workplace setting; similarly, others advocate that stigmatisation of chronic pain, and its consequences, can only be addressed at a policy and practice (rather than individual cognitive) level [82].
Based on our findings through this rigorous PAW toolkit development process, we make recommendations for supporting employees with chronic or persistent pain. Many of these recommendations require input from the employer, such as disclosure, and seeking reasonable adjustments (e.g., line manager or work performance appraiser). Therefore, we particularly advocate for education and training of line managers to raise awareness about long-term pain and disability, reduce stigma for employees, enhance compassion and communication about pain-related needs in the workplace, and ultimately increase the likelihood of appropriate supports being put in place for individuals with pain. This is becoming increasingly pertinent in the light of the long-lasting global COVID-19 pandemic, during which new chronic pain, or exacerbations of pre-existing chronic pain is predicted [83], and the delivery of chronic pain care has been severely impacted [4][5][84].
Study Limitations and Future Research
The online surveys were intentionally brief to maximise completion and provide only information that was required for the corresponding toolkit development step. We therefore collected details of age, gender and employment status (employees), and level of seniority, sector, and organisation type (employers). We did not collect data on the occupation, race/ethnicity or socio-economic status of employees completing surveys, or the occupation of employer representatives, although these factors may impact on perceptions of pain, help-seeking (or support-giving) behaviours. Specific beliefs about the nature of pain and disability play an important role; for example, a cultural group may hold expectations and acceptance of pain as part of normal life, and this may determine whether pain is viewed as a ‘problem’ that requires management and solutions. Some cultural groups may be resistant to disclosure of chronic conditions and help-seeking or may not accept individual responsibility for self-management of health conditions. Although an exploration of cultural influence on pain and self-management are beyond the scope of this study, there is a need to further explore the applicability of the PAW toolkit in different cultural groups and identify any potential cultural differences in pain perceptions, challenges and solutions that would allow for adaptation of the existing toolkit for different settings and contexts.
The PAW toolkit is intended for use by employees with chronic or persistent pain rather than managers or organisational leaders, although we recommend that employers familiarise themselves with the toolkit content to be aware of the self-management advice provided for employees and we reiterate the value of awareness-raising, education and training for both employees and line managers. It should be noted that through the collaborative-participatory approach taken, concerns of managers and organisational leaders were raised that the PAW toolkit (as an individual employee-level resource) cannot address. These not only included concerns of managers (e.g., processes, knowledge of supportive services) but also fundamental issues relating to workplace culture (e.g., the need to decrease pain-related stigma, and create a psychologically safe work environment to encourage disclose and help-seeking). There are many examples, but transferable knowledge from studies of stigma in healthcare settings suggests that stigma is best addressed by empowering individuals, targeting all levels and occupational groups, addressing multiple stigmas at once, and simultaneously targeting multiple ecological levels, such as targeting both individual attitudes and practices as well as policies and environment within the particular setting [85]. Vocational rehabilitation research focusing on specific conditions advocates that organisational responses to disclosure need to demonstrate trust and inclusive decision making, focus on employee ‘abilities’, and enhance perceptions of psychological safety at work (e.g., multiple sclerosis [86]).
Overall, individual-level interventions need to be delivered alongside organisational-level interventions to maximise the potential for positive outcomes. Explicitly, people who have chronic or persistent pain may do their best to gain the knowledge, confidence and skills required to self-manage, but effective self-management and help-seeking will only be possible with the right opportunities, support, and autonomy.
sions: Efforts to support self-management of chronic or persistent pain are increasingly important, particularly due to the global work impacts of the COVID-19 pandemic. Employers do not currently routinely provide guidance or support for staff with chronic or persistent pain. The PAW toolkit is a new resource to support employees with managing chronic pain at work, co-created with healthcare professionals, employers, and people with persistent pain. The PAW toolkit can be widely implemented to support employees with chronic or persistent pain in the workplace. Disability policies alongside line manager education and training are recommended to foster a psychological safe work environment, maximise employee support and facilitate appropriate actions. Further research could explore the impact of the PAW toolkit on employee pain, wellbeing and support, and organisational outcomes.
The Pain at Work Toolkit can be accessed here: https://www.nottingham.ac.uk/toolkits/play_24452
For more details about the study, visit: https://doi.org/10.3390/healthcare10010056