2. Anatomy and Physiology of the Vagina
The vagina is located in women between the rectum, the urethra, and the bladder. It is a thin-walled fibromuscular tube that is extending from outside the body to the cervix
[2][3][4][2,3,4]. The dimensions of the vagina are crucial factors that affect drug administration and are characterized by an interindividual variability, which is modified in an age-related manner. Thus, its average length in women of reproductive age is 6–8 cm for the front wall and up to 14 cm for the back wall, including the length of the cervix
[5]. Moreover, the average vaginal surface area is calculated to be ca. 87.46 cm
2 (range: 65–107 cm
2)
[6] and is significant for the absorption of administered active substances
[7].
There are four distinct anatomical regions, which are observed in the lower part of the female genital tract: the introitus (covered by a keratinized epithelium), the vaginal epithelium (covered by a non-keratinized stratified squamous epithelium), the ectocervix, (covered by a mucosal layer), and the endocervix (columnar epithelium with numerous glands)
[2][3][4][2,3,4]. The physiological cervical stratified squamous epithelium is formed by distinct layers of epithelial cells, which can be classified into different classes based on the stage of maturation: basal, parabasal, intermediate, and superficial. Throughout maturation, various cells from the basal layer move gradually towards the superficial layer, obtaining a flatter shape. However, superficial layers of the cervix, which are closer to the vaginal lumen, are mainly characterized by tight junctions
[8].
Furthermore, the thickness of cervical squamous epithelium is variable (0.2–0.5 mm) and is directly related to age. After menopause, cytoplasmic volume condensation and epithelium atrophy is observed
[9]. It is essential that the structure of the epithelium is considered as the crucial site for the most effective and targeted drug delivery of the active substances, the permeability and solubility properties of which determine the final drug delivery efficacy (topical or systemic action) across these tissues and the toxicity profile
[8].
3. Vaginal Drug Delivery
The anatomy and physiology of the vagina can affect and provoke challenges in achieving local or systemic drug delivery
[8][10][8,10]. The most common drugs that are usually administered in the vagina are related to the treatment of vaginal infections (antimicrobials/antifungal), spermicides or contraceptive agents, and active ingredients related to hormone replacement therapy, induction of labour, and interruption of pregnancy
[11][12][11,12]. There is a plethora of formulations used for vaginal administration including solid dosage forms (suppositories and tablets), semisolids (creams and gels) and other forms such as intravaginal rings, films and foams
[13].
Several advantages are provided by vaginal (DDSs)
[2][12][14][15][2,12,14,15]. The vaginal route is easy and convenient due to the simple administration of the formulations. It is an accessible and non-invasive route, since it does not cause tissue damage and potential infections related with parenteral administration. Moreover, drugs which have a systemic action and are administered vaginally are easily absorbed due to vaginal high vascularity, which allows adequate blood supply and, consequently, they do not undergo from hepatic first pass metabolism
[8][16][8,16]. Vaginal administration also minimizes many side effects which can be provoked by oral and parenteral drugs, such as those affecting the gastrointestinal tract and liver
[16]. Other absorption pathways that can occur through this route are passive diffusion and active transportation, which are defined by permeability and absorption characteristics, such as the molecular weight (MW), the extent of ionization, the lipophilicity, and the dissolution properties of active substances
[10].
Another significant advantage of the vaginal route drug administration is the specialized local effect of the drug when treating infections or preventing sexually transmitted diseases of the female reproductive system.
4. Factors That Affect Drug Absorption in Vaginal Epithelium
Physiologically, the vagina generates several obstacles in drug delivery due to its variability in potential structural form, which can affect the acceptability and the administration of certain vaginal formulations
[10]. These variations are crucial to be considered from the pharmacological point of view, since drug administration and absorption are directly related with the physiology of the vagina. These factors are cervical mucus, vaginal epithelium thickness, fluid, microflora, enzymatic activity, and pH
[7] (
Figure 1).
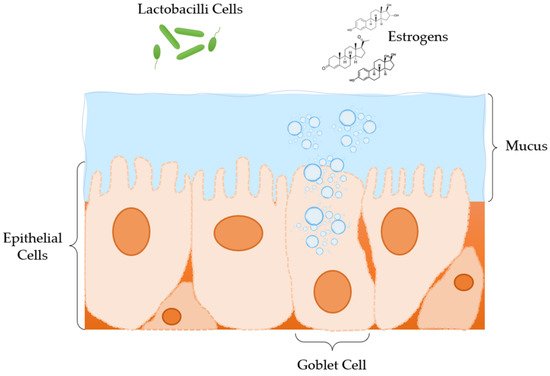
Figure 1.
Anatomical and physiological features of the vagina microenvironment.
Changes in vaginal mucosa levels occur during puberty, along with adrenal and gonadal maturation, and reach a maximum in thickness and glycogen volume during ovulation. Mucus thickness and vaginal fluid secretion modifications are adapted during pregnancy, due to hormonal alterations. In menopause and postmenopause time periods, cervico-vaginal secretions diminish and become sparse
[17][18][18,19]. Thus, drug permeability, through the vaginal surface, can affect drug distribution and pharmacokinetics and, as a result, the drug’s efficacy and resulting toxicity levels
[8][12][14][8,12,14].
The vaginal epithelium is coated in a mucous layer, which consists of water, a matrix of mucins (glycoproteins with high MW), enzymes, plasma proteins, amino acids, lipids, cholesterol, and a number of inorganic ions
[19][20][21][20,21,22]. Mucous secretions (composition, quantity, and physical characteristics) depend on the menstrual cycle, as oestrogens affect their production. They are produced from goblet cells in the epithelium of the endocervix and Bartholin glands. However, the squamous epithelium of the vagina and ectocervix are not involved in the production of mucus. Furthermore, this mucus layer is structurally analogous to a complex net of tangled microfibers with multiple coarsened folds, which enhance the absorption surface. Specifically, during ovulation, the amount of mucus secretion is augmented, creating larger, thicker, and more viscous pores, leading to an increase in the total volume of vaginal fluid, a higher pH, and mucin content. Hence, mechanical, and structural features of vaginal mucus have a significant impact on drug targeting and release rate, affecting the pharmacodynamics of certain drugs
[10].
Another significant factor to drug delivery is the vaginal fluid, which is produced by the mucous membranes of the endometrium and then accumulates inside the vagina covering the vaginal epithelium
[7]. The major function of this fluid is to coat the vaginal mucosa and to shelter the deeper tissues against a possible entry of pathogens
[8]. The fluid layer on the epithelium and the enzyme activity in the vaginal fluid has been identified as a significant barrier to drug delivery and absorption and plays a significant role in ensuring that the active substance reaches its target
[8]. Moreover, the release rate profile of drugs administered by this route and the residence time and bio-adhesion of the formulation can be modified by dynamic changes in the volume and composition of the vaginal fluid
[8][10][8,10].
One more aspect that influences drug delivery in the vaginal fluid is its pH. The normal pH value in an adult woman is ~3.5–5.0, due to commensal Lactobacillus sp., which produces lactic acid from the glycogen from the sloughed epithelial cells of the mucosa. The deposition of glycogen on the vaginal epithelium depends on the presence of oestrogens. Nevertheless, glycogen reduction is observed in postmenopausal women.
5. Excipients Used in Modified Drug Release Pharmaceutical Dosage Forms for Vaginal Administration
A proper pharmaceutical formulation has to be described by quality characteristics, such as safety, efficacy, stability, and acceptability. However, many considerations have to be taken into account when developing a drug product for vaginal administration
[8]. The choice of the dosage form depends on the physical and chemical characteristics of the drug, its mechanism of action, the target of the formulation and last but not least patient comfort
[8][22][8,31]. Many pharmaceutical formulations have been used for drug delivery to the vagina. Despite the fact that traditional formulations, such as vaginal creams
[23][24][32,33], gels
[25][26][27][34,35,36], tablets/capsules
[28][29][37,38] and suppositories
[30][39] have a prevalence, there are other more novel dosage forms such as films
[31][40] intravaginal rings
[32][33][34][41,42,43] and nanomedicines
[14] (
Figure 2).
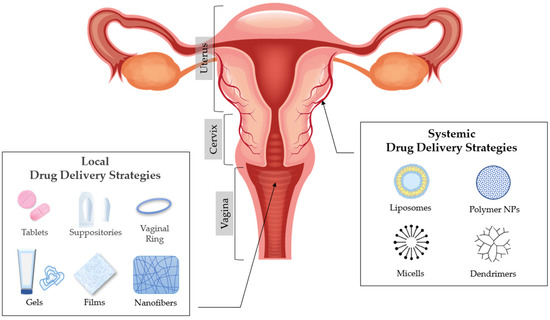
Figure 2.
Anatomy of the vagina and drug delivery strategies.
5.1. Excipients Used in Matrix Tablets for Vaginal Administration
The most common type of vaginal DDSs are matrix tablets
[29][38], in which the active substance is uniformly distributed in a matrix of hydrophilic polymers. When hydrophilic polymers interact with the vaginal fluid, they create an
in situ gelling effect, through which the drug diffuses. The release rate of the active substance from matrix type tablets depends on the type, ratio, particle size, and solubility of the polymer, the solubility and particle size of the drug, and the geometry of the matrix. The mechanisms of erosion and diffusion take place simultaneously in the dissolution of matrix type tablets and determine the release of the active ingredient. The dominant release rate mechanism is determined by the solubility properties of the drug
[7].
5.2. Excipients Used in Solid Dosage Forms for Vaginal Administration: Ovules and Vaginal Suppositories
Scientists have also explored alternatives to vaginal tablets. Ovules and vaginal suppositories have been formulated for topical delivery. The formulation of such products requires a base (oily/emulsifying/aqueous), where the API will be placed in, and in some cases antioxidants and/or preservatives are also used
[15]. The composition of the suppository base has an important role in drug release rate and extent.
5.3. Excipients Used in Semi-Solid Dosage Forms for Vaginal Administration: Gels
Gels are semisolid systems that consist of two components (a liquid and a solid)
[8]. When these components are homogenized, the solid component traps the liquid, creating a gelling effect and consequently producing a solid-liquid mixture. According to the polarity of the liquid component, gel systems are categorized in hydrogels, which contain a polar solvent (such as water) and organogels, where the liquid component is apolar (such as vegetable oils). Hydrogels are used in pharmaceutical industry for the administration of active substances on skin and/or mucous membranes. They are widely accepted by patients for being refreshing, hydrating, and easy in application and in removal. Therefore, their hydrophilicity creates a difficulty in drug release and consequently in absorption through the lipophilic skin barrier. As far as organogels are concerned, they outline a great ability to cross the skin barrier. However, they are not highly acceptable from patients, due to their greasy texture
[35][36][37][54,55,56].
5.4. Excipients Used in Films for Vaginal Administration
Solid and semisolid conventional vaginal dosage forms usually show a short residence time on the vaginal mucosa especially in disease condition due to added vaginal secretions. Therefore, the therapeutic effect is available only for a short period of time requiring frequent dosing and resulting in poor patient compliance. A method to overcome this, is the
in situ gel forming films. Polymeric films are safe and effective and can be used for vaginal administration of various drug candidates. Vaginal film formulations require excipients such as a film former plasticizer (polymer), humectant(s), and a solvent
[38][49].
5.6. Excipients Used in Nanomedicine for Vaginal Administration
Nanoparticles (NPs) have been used as advanced DDSs due to their capability to protect therapeutic agents, their versatility to control drug release profiles and their tunable surface properties. NP encapsulation is being investigated for therapeutic applications in oral, nasal, transdermal, brain, and cardio-vascular systems as their sub-micron size allows them to penetrate into the tissue through interstitial spaces to be readily taken up by the cells. Their other advantages (modified drug release, non-toxic for the vaginal physiological environment) render them unique carriers for vaginal drug delivery
[17][18].
6. Conclusions
Topical drug delivery is site specific, leading to better patients’ compliance and to the diminution of side effects. Efficient drug delivery at the vaginal cavity is often complicated, due to its discrete physiological features. Thus, researchers have sought to develop formulation strategies using novel excipients for the successful drug delivery. Biomaterials that are biocompatible and biodegradable are suitable for the formulation of novel targeted DDSs; thus, ameliorating drug-tissue compatibility issues and drug therapeutic levels. Biomaterials have gained ground in fabricating DDSs, enhancing and optimizing drug release rate, by targeting to controlled-release or time-dependent release rate. Materials that show a diversity in pH response, swelling and bioadhesive properties, similar to vaginal epithelium, along with low toxicity effects, have a significant impact on the design of multifunctional pharmaceutical formulations. To this end, several biocompatible polymers, such as chitosan, hydroxypropylmethylcellulose, methacrylic acid co-polymers, polyethylene oxide, polylactic-co-glycolide, etc., have been employed to promote mucoadhesiveness, and therefore drug release, with very promising results.