The term Metabolic Obesity in People with Normal Body Weight (MONW) is used to describe people who, despite having a healthy body weight - usually defined by the body index (BMI), and more and more often also the percentage of adipose tissue - show metabolic disorders characteristic of obese people. Otyłość metaboliczną u osób z prawidłową masą ciała (MON W) po raz pierwszy zaobserwowano w 1981 roku Neil Ruderman, opisując przypadek pacjenta z objawami wskazującymi na zespoły metaboliczne — obniżoną insulinowrażliwością, nadciśnieniem, T2DM i hipertriglicerydemią — pomimo prawidłowego wskaźnik masy ciała (BMI). Podstawowe kryteria diagnostyczne były złożone i wymagały użycia testów, które nie są rutynowo stosowane u zdrowych osób. W późniejszych latach diagnozę oparto na kryteriach klasycznego zespołu metabolicznego (MetS). Obecnie poszukuje się nowych kryteriów, które pozwolą na szybką i trafną diagnozę MONW.
1. Wstęp
Współczesny styl życia człowieka nie sprzyja zachowaniu zdrowia. Siedząca praca, mała aktywność fizyczna, niewłaściwa dieta, nieregularne posiłki i podjadanie między nimi oraz przejadanie się wieczorem sprzyjają otyłości [ 1 ]. Zgodnie z definicją podaną przez Światową Organizację Zdrowia (WHO) nadwaga i otyłość definiowane są jako nieprawidłowa lub nadmierna akumulacja tkanki tłuszczowej, stanowiąca zagrożenie dla zdrowia [ 2 ]. Statystyki dotyczące odsetka osób z nadmierną tkanką tłuszczową nie są optymistyczne. Global Burden of Disease Grupa którzy przeanalizowali dane z 68,5 mln osób z 195 krajów odnotowano w 2017 roku, że w latach 1980 i 2015, częstość występowania otyłości u dzieci i dorosłych podwoiła się w 73 krajach i wykazuje stały wzrost w większości innych krajów [ 3]. Ponadto wyniki Warda i wsp. sugerują, że do 2030 r. co druga dorosła osoba będzie miała otyłość, a co czwarta dorosła osoba będzie miała otyłość ciężką [ 4 ].
Otyłość jest zwykle spowodowana dostarczaniem organizmowi zbyt wielu składników odżywczych w stosunku do potrzebnej ilości. Nadmiar ten jest magazynowany w organizmie w postaci trójglicerydów, powszechnie znanych jako tłuszcz, a adipocyty, w których przechowywane są trójglicerydy, nazywane są komórkami tłuszczowymi. Zwiększona masa tkanki tłuszczowej może objawiać się zwiększeniem wielkości komórek adipocytów (hipertrofia) i proliferacją (hiperplazja). Gdy adipocyty nie mogą wchłonąć nadmiaru trójglicerydów, prowadzi to do adipogenezy, tworząc dodatkową przestrzeń do przechowywania dużych ilości tłuszczu [ 5 ].
Nadmiar tkanki tłuszczowej sprzyja rozwojowi wielu chorób, m.in.: zespołu metabolicznego (MetS), cukrzycy typu 2 (T2DM), nadciśnienia tętniczego, che oroby niedokrwiennej serca, miażdżycy, hiperlipidemii, niealkoholowego stłuszczenia wątroby, a także powikłań związanych z układ kostno-stawowy, mięśniowo-szkieletowy i oddechowy. Ponadto otyłość jest jednym z czynników ryzyka raka piersi, macicy, przełyku i nerek [ 1 , 6 , 7 ].
Otyłość jest zaburzeniem niejednorodnym. Osoby z otyłością charakteryzują się międzyosobniczą zmiennością pod względem rozmieszczenia tkanki tłuszczowej, profilu metabolicznego orst recoaz stopnia ryzyka sercowo-naczyniowego i metabolicznego. Magazynowanie tłuszczu w jamie brzusznej znacznie bards oziej sprzyja rozwojowi T2DM i chorób wieńcowych niż otyłość obwodowa lub pośladkowo-udowa. Istotne różnice anatomiczne, komórkowe, molekularne, fizjologiczne, kliniczne i prognostyczne obserwuje się również między podskórną tkanką tłuszczową (SAT) a trzewną tkanką tłuszczową (VAT) [ 8 ]. Chociaż wykazano, że oba typy tkanki tłuszczowej są odpowiedzialne za rozwój insulinooporności [ 9], nadmiar zapasów trzewnych może okazać się szkodliwy dla zdrowia człowieka. Trzewna tkanka tłuszczowa jest znacznie bardziej aktywna metabolicznie i hormonalnie w porównaniu do jej podskórnego odpowiednika, wykazuje również właściwości prozapalne i jest podatna na lipolizę. Poza wspomnianą wcześniej insulinoopornością, trzewna tkanka tłuszczowa odgrywa istotną rolę w rozwoju T2DM, nietolerancji glukozy, nadciśnienia tętniczego i chorób układu krążenia [ 10 , 11 ]. Obserwacje długoterminowe wykazały istotny pozytywny związek między podwyższonym poziomem VAT a zwiększonym ryzykiem chorób sercowo-naczyniowych. Takiej zależności nie zaobserwowano w przypadku SAT [ 12 ].
2. Mechanizmy biologiczne MONW
Metabolically obese normal weight (MONW) was first described in the 1980s, when Ruderman et al. [1] described a case of patients with symptoms indicative of the metabolic syndromes—reduced insulin sensitivity, hypertension, T2DM, and hypertriglyceridemia—despite normal body mass index (BMI). In 1989 Ruderman et al. [2] proposed a scoring system that assessed 22 features (Table 1) that were assigned a specific number of points. Obtaining at least 7 points was equivalent to the diagnosis of MONW.
Tabl
Based on the research carried out so far in the MONW group (women and men, in different age groups and different ethnic groups), it can be concluded that the excessive accumulation of fat, mainly visceral, adversely affects the lipid profile [13,14,15], blood pressure [13,14], intensifies inflammatory and thrombotic processes [16], as well as oxidative stress [17]. On the other hand, in other studies in non-obese patients with an excessive accumulation of fat, no atherogenic lipid profile, differences in blood pressure values [18,19] or in the concentration of adipocytokines [14,15] were observed.
The central parts of the complex and still insufficiently recognized pathogenesis of MONW are the increased amount of visceral and subcutaneous fat in the abdominal area, insulin resistance and hyperinsulinemia, which are recognized as key disorders in MONW [14,19]. The increase in the mass of visceral adipose tissue causes increased lipolytic activity and the excess release of free fatty acids, which are accumulated in the liver and skeletal muscles. In the liver, increased very-low-density lipoprotein (VLDL) biosynthesis and reduced degradation, thereof, translate into an increase in the concentration of triglycerides in the blood plasma, and as a result of the action of lipoprotein lipase (LPL), cholesterol ester transfer protein (CEPT) and hepatic lipase (HL), LDL particles of high atherogenic potential are formed from VLDL particles. In addition, CETP-mediated multiplied lipid transport generates HDL particles of larger sizes. Hepatic insulin resistance is also manifested by increased glycogenolysis and gluconeogenesis, which increases endogenous glucose production and is associated with the development of non-alcoholic fatty liver disease (NAFLD) [20]. On the other hand, in skeletal muscles, the accumulation of biologically active lipids (long-chain acyl-CoA, diacylglycerols, ceramides) negatively affects the operation of the insulin pathway, inducing muscle insulin resistance, which is associated with impaired translocation of GLUT4 to the cell membrane and reduced transport of glucose to the interior myocytes, thus preventing glucose uptake [21]. This partially explains the complex relationships between obesity, insulin resistance, hyperglycemia and dyslipidemia.
Hypertrophic adipocytes are also a source of pro-inflammatory cytokines that enhance insulin resistance both in the fat cells themselves and in other tissues. Activated by inflammatory mediators (TNF-α, interleukin 1), nuclear factor kappa B (NF-kB) and c-Jun N-terminal kinase (JNK) pathways are the link between chronic inflammation and insulin resistance [22]. Obesity is accompanied by a subclinical chronic inflammation in which, in addition to activating pro-inflammatory signal transduction pathways, there is also an overexpression of pro-inflammatory cytokines in adipose tissue. Among the adipokines, whose activity may contribute to the development of metabolic disorders observed in MONW, the most frequently mentioned are resistin, leptin, adiponectin, TNF-α and IL-6 [17,23]. The pro-inflammatory and prothrombotic states are important components of the metabolic disorders associated with the excessive accumulation of adipose tissue, especially of the visceral type. The pro-inflammatory state is characterized by an increased concentration of cytokines such as TNF-α and IL-6, as well as an increased concentration of acute phase proteins—fibrinogen and CRP protein. The prothrombotic state is diagnosed on the basis of elevated levels of fibrinogen, PAI-1 and other coagulation factors. Increased biosynthesis of the above-mentioned cytokines by lipid-laden adipocytes causes not only tissue resistance to insulin but also pro-inflammatory state, endothelial dysfunction and disorders of coagulation and fibrinolysis.
There is evidence from experimental and clinical studies for a causal relationship between the amount of body fat and insulin resistance and the development and maintenance of elevated blood pressure. The increase in the prevalence of arterial hypertension especially concerns visceral obesity [24]. The etiological factors of arterial hypertension include: hemodynamic disorders accompanying obesity and an increase in peripheral vascular resistance associated with endothelial dysfunction, insulin resistance and the influence of adipokines released from adipose tissue [25].
The excess of energy substrates flowing into the cell in the form of free fatty acids and glucose causes the formation of an increased amount of acetyl-CoA and, thus, NADP in the mitochondria and, as a result, an increase in the biosynthesis of reactive oxygen species (ROS) and the development of oxidative stress [26].
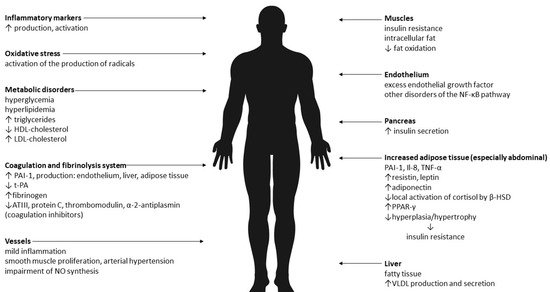
Therefore, it seems that the results of research on the pathogenesis of MONW to date are not unequivocal. The dominant causes are insulin resistance and abdominal obesity. It is believed that the cause of the changes is the increased mass of adipose tissue and its pro-inflammatory activity. Adipose tissue is an active endocrine and paracrine endocrine organ, and the secreted pro-inflammatory substances (adipokines) are an important link between excess body weight, insulin resistance, atherosclerosis and type 2 diabetes. In addition, there is oxidative stress. The effects of abdominal obesity and insulin resistance are summarized in Figure 1. A point scale to identify people with MONW [2].
.
Rycina 1. Skutki otyłości brzusznej i insulinooporności [ 13 , 14 , 15 , 16 , 17 , 18 , 19 , 20 , 21 , 22 , 23 , 24 , 25 , 26]. Legenda: VLDL—lipoproteina o bardzo małej gęstości, NO—tlenek azotu, PAI-1—inhibitor aktywatora plazminogenu-1, t-PA—tkankowy aktywator plazminogenu, ATIII—antytrombina III, NF-κB—Il-8—interleukina-8 , TNF-α – czynnik martwicy nowotworu α, β-HSD – dehydrogenaza beta-hydroksysteroidowa, PPAR-γ – receptor gamma aktywowany przez proliferatory peroksysomów, HDL – lipoproteina o dużej gęstości, LDL – lipoproteina o niskiej gęstości.
Wiadomo, że na występowanie MONW mają wpływ zarówno czynniki środowiskowe – brak aktywności fizycznej, niezdrowa dieta, palenie tytoniu, spożywanie alkoholu – jak i czynniki genetyczne. Podczas porównywania nawyków żywieniowych, kontrolowane badania wykazały, że kobiety z MONW spożywały więcej tłuszczów nasyconych i mniej błonnika niż kobiety zdrowe metabolicznie [ 27 ]. Efekt palenia potwierdzili Tilaki i Heidari [ 28 ]. Palenie było statystycznie istotnie ( p = 0,005) związane z fenotypem MONW u 170 mężczyzn i kobiet pochodzenia irańskiego. Badania w populacji koreańskiej wykazały, że istnieje związek między występowaniem MONW i umiarkowanym spożyciem alkoholu oraz niewielką ilością czasu na aktywność fizyczną o umiarkowanej intensywności [ 29].]. Palenie i spożywanie alkoholu jako czynniki ryzyka zostały potwierdzone w metaanalizie przeprowadzonej przez Wanga i in. [ 30 ]. Pewne jest, że na występowanie MONW mają również wpływ czynniki genetyczne. Jednak dane dotyczące konkretnych genów są dość ograniczone. Li i in. [ 31 ] wykazali, że CDKAL1 rs2206734 jest związany z ochroną przed fenotypem MONW. CDKAL1, należący do rodziny metylotiotransferaz, zwiększa wydajność translacji i jest szeroko eksprymowany w tkankach metabolicznych, w tym w tkance tłuszczowej i komórkach β trzustki. Z kolei Park i in. [ 32 ] znaleźli powiązania między genami GCKR, ABCB11, CDKAL1, CDKN2B, NT5C2 i APOC1 a zaburzeniami metabolicznymi u osób z prawidłową masą ciała.
|
|
type 2 diabetes mellitus |
|
|
impaired glucose tolerance |
|
| polycystic ovaries
|
3. Kryteria podstawowe dla MONW
This system had its drawbacks, requiring the performance of biochemical tests not routinely performed in healthy people (including uric acid concentration). For this reason, the search for much simpler and more accessible diagnostic criteria was started.
Autorem pierwszych kryteriów diagnostycznych MONW jest Ruderman i in. [ 34 ], którzy w 1989 roku zaproponowali system punktacji oceniający 22 cechy ( tabela 1 ), którym przypisano określoną liczbę punktów. Uzyskanie co najmniej 7 punktów było równoznaczne z rozpoznaniem MONW.
2. A contemporary look at MONW
Tabela 1. Skala punktowa do identyfikacji osób z MONW [ 34 ].
| Zwrotnica |
Objawy |
| 1 |
stężenie triglicerydów > 100–150 mg/dl
ciśnienie krwi 125–140/85–90 mmHg
przyrost masy ciała: >4 po 18 latach dla kobiet i 21 lat dla mężczyzn
BMI: 23–25 kg/m 2
talia: 71,1–76,2 dla kobiet i 86,3-91,4 dla mężczyzn
pochodzenie etniczne: czarne kobiety, Amerykanie pochodzenia japońskiego, Latynosi,
Melanezyjczycy, Polinezyjczycy, Maorysi z Nowej Zelandii |
| 2 |
nieprawidłowa glikemia na czczo (110–125 mg/dl)
stężenie triglicerydów > 150 mg/dl
ciśnienie krwi > 140/90 mmHg
samoistne nadciśnienie tętnicze (poniżej 60 lat)
przedwczesna choroba wieńcowa (poniżej 60 lat)
niska masa urodzeniowa (<2,5 kg) )
brak aktywności (<90 min ćwiczeń aerobowych/tydzień)
przyrost masy ciała: >8 po 18 latach dla kobiet i 21 lat dla mężczyzn
BMI: 25–27 kg/m 2
talia: >76,2 dla kobiet i >91,4 dla mężczyzn
kwas moczowy (> 8 mg/dl)
pochodzenie etniczne: Indianie, australijscy Aborygeni, Mikronezyjczycy, Naruanie |
| 3 |
cukrzyca ciążowa
stężenie triglicerydów > 150 mg/dl i HDL cholesterol < 35 mg/dl
cukrzyca typu 2 lub upośledzona tolerancja glukozy
hipertriglicerydemia
przyrost masy ciała: >12 po 18 latach u kobiet i 21 lat u mężczyzn
przedwczesna choroba wieńcowa serca (poniżej 60 lat )
pochodzenie etniczne: niektóre plemiona Indian amerykańskich |
| 4 |
cukrzyca typu 2
upośledzona tolerancja glukozy
policystyczne jajniki |
|
Points
|
Symptoms
|
|
1
|
triglycerides level > 100—150 mg/dL
blood presure 125—140/85—90 mmHg
weight gain: > 4 after 18 years for women and 21 years for men
BMI: 23—25 kg/m2
waist: 71.1—76.2 for women and 86.3—91.4 for men
ethnicity: black women, Japanese-Americans, Latinos,
Melanesians, Polynesians, New Zealand Maoris
|
|
2
|
impaired fasting glucose (110—125 mg/dL)
triglycerides level > 150 mg/dL
blood presure > 140/90 mmHg
essential hypertension (under age 60 years)
premature coronary heart disease (under age 60 years)
low birth weight (< 2.5 kg)
inactivity (< 90 min aerobic exercise/week)
weight gain: > 8 after 18 years for women and 21 years for men
BMI: 25—27 kg/m2
waist: > 76.2 for women and > 91.4 for men
uric acid (> 8 mg/dL)
ethnicity: Indians, Australian aborigines, Micronesians, Naruans
|
|
3
|
gestational diabetes
triglycerides level > 150 mg/dL and HDL cholesterol < 35 mg/dL
type 2 diabetes mellitus or impaired glucose tolerance
hypertriglyceridemia
weight gain: > 12 after 18 years for women and 21 years for men
premature coronary heart disease (under age 60 years)
ethnicity: some American Indian tribes
|
|
4
|
It is now known that in addition to metabolic disorders people with MONW are characterized by an increased content of adipose tissue—in particular, its visceral deposit [3]. The assessment of the fat depot is possible after measuring the body composition. This test allows for precise and accurate measurement of individual body components including muscle mass, lean mass and, most importantly, the percentage of adipose tissue (PBF,% BF), the knowledge of which, together with the BMI value, can be used as a screening tool. Among body compositions methods of body composition analysis, dual-energy X-ray absorptiometry (DXA) is considered the “gold standard”.
System ten miał swoje wady, wymagał wykonywania testów biochemicznych, które nie są rutynowo wykonywane u zdrowych ludzi (w tym badania stężenia kwasu moczowego). Z tego powodu rozpoczęto poszukiwania znacznie prostszych i bardziej dostępnych kryteriów diagnostycznych.
Currently, the authors of the MONW diagnostics use the developed indicators:
1. the visceral adiposity index (VAI) - which is based on BMI, WC, triglycerides and HDL cholesterol:


2. the triglycerides–glucose index (TyG) - which is the product of fasting blood glucose and triglycerides:

3. lipid accumulation product (LAP) - which is based on the combination of waist circumference measurements and fasting triglycerides:


4. the cardiometabolic index (CMI) - which is based on the combination of triglycerides, HDL cholesterol and waist-to-height ratio:
5. metabolic syndrome (MetS) criteria according to the criteria of the National Cholesterol Education Program Adult Treatment Panel III (NCEPATP III) or proposed by the International Diabetes Federation (IDF):
Table 2. Diagnostic criteria for the Metabolic Syndrome.
|
Measure
|
NCEPATP III [4]
|
IDF [5]
|
|
WC
|
> 102 cm for men
> 88 for women
|
≥ 94 cm for men
≥ 80 cm for women *
|
|
TG
|
> 1.7 mmol/L
|
> 1.7 mmol/L
or treating
hypertriglyceridemia
|
|
High-density lipoprotein (HDL) concentration
|
< 1.3 mmol/L for men
< 1.03 mmol/L for women
|
< 1.0 mmol/L for men
< 1.3 mmol/L for women
or treating said lipid disorder
|
|
BP
|
> 130/80 mm Hg
|
≥ 130 mm Hg systolic or
≥ 85 mm Hg diastolic
or treatment of previously
diagnosed arterial
hypertension;
|
|
FG
|
> 6.1 mmol/L
|
≥ 5.6 mmol/L
or drug treatment of
type 2 diabetes
|
Legend: WC—waist circumference; TG—concentration of triglycerides; BP—blood pressure; FG—fasting glucose; * in the European population.
3. Conclusions
MONW is undoubtedly a growing problem that should be the focus of further research. Due to the fact that it is a disease that does not show phenotypic signs, screening tests should be carried out, mainly including body composition analysis among young, theoretically healthy people. This will allow for early detection of MONW and appropriate reactions before the occurrence of undesirable consequences—including atherosclerosis or coronary artery disease.