Multiple myeloma (MM) accounts for 10–15% of all hematologic malignancies, as well as 20% of deaths related to hematologic malignant tumors, predominantly affecting bone and bone marrow. Positron emission tomography/computed tomography with 18F-fluorodeoxyglucose (FDG-PET/CT) is an important method to assess the tumor burden of these patients. It is often challenging to classify the extent of disease involvement in the PET scans for many of these patients because both focal and diffuse bone lesions may coexist, with varying degrees of FDG uptake. Different metrics involving volumetric parameters and texture features have been proposed to objectively assess these images.
- multiple myeloma
- 18F-fluorodeoxyglucose
- positron emission tomography
- metabolic tumor volume
- total lesion glycolysis
- intensity of bone involvement
1. Introduction
Multiple myeloma (MM) is a hematological malignancy caused by the clonal expansion of plasma cells. It is one of the most frequent hematologic malignancies worldwide, accounting for 10–15% of them, as well as 20% of deaths related to hematologic neoplasms [1,2,3][1][2][3]. MM presents a heterogeneous distribution of tumor mass throughout the skeleton and may also exhibit extra-osseous foci.
Three-dimensional imaging techniques, such as whole-body computed tomography (CT), positron emission tomography/computed tomography (PET/CT) with 18F-fluorodeoxyglucose (FDG) and magnetic resonance imaging (MRI), are currently replacing whole body radiographs (WBR) for bone evaluation of these patients [7][4]. FDG-PET/CT detects the metabolic response early before morphological changes can be detected by conventional imaging or MRI [8] [5]. Therefore, it is useful for assessing response to induction chemotherapy and autologous or allogeneic stem cell transplantation [8,9] [5][6].
FDG-PET/CT visual interpretation presently relies on semi-quantitative measures, such as the Deauville score, which was prospectively validated only for lymphomas [14,15][7][8]. The definition of FDG-PET positivity is currently defined by visual criteria that can be biased by inter-observer variability [12][9]. Recently, an attempt to better classify the amount of tumor mass was made by Nanni et al. [16,17][10][11] using an extensive stratified scoring system, which does not completely eliminate the subjectivity of interpretation.
Quantitative metrics are less operator-dependent than visual methods and can facilitate inter and multi-center clinical discussions [18][12]. Attempts have been made to standardize quantitative interpretations of FDG-PET/CT in MM, especially using parameters that refer to active metabolic disease [12,19,20,21,22][9][13][14][15][16]. However, the main limitation of FDG-PET/CT to measure the metabolic tumor volume in MM is to standardize the criteria for delimiting the areas affected by the disease. This impacts the reproducibility of interpretations, especially when assessing response to therapy. Therefore, there is a need for standardized and reproducible methods for quantifying the tumor burden using FDG-PET/CT.
2. Methods to quantify Multiple Myeloma tumor burden using FDG-PET/CT images
Quantitative parameters to assess FDG-PET/CT images, includes standardized uptake value (SUV) and its derivatives, metabolic tumor volume (MTV), total lesion glycolysis (TLG), percentage of bone involvement (PBI) and intensity of bone involvement (IBI).
SUV is a dimensionless parameter which is the activity concentration within a region, normalized by the injected activity and patient weight [24][17]. Maximum SUV (SUVmax) is the highest SUV value found in an area of interest, which can be a single lesion or a set of lesions or even the whole-body. SUV derivations, as SUVpeak, mean SUV (SUVmean) and standard deviation of SUV (SDSUV) are less affected by image noise than SUVmax, since they are based on radiotracer uptake in a specific region and outliers end up being softened.
MTV and TLG are volumetric parameters used to quantify the tumor burden of cancer patients. MTV is usually expressed in milliliters (ml) or cubic centimeters (cm3) [39][18]. MTV segmentation can be made manually, automatically or using a hybrid method (semi-automatic) [40][19]. TGL is derived from MTV. It is calculated by multiplying the MTV by its SUVmean. For this reason, in addition to the volumetric factor, TLG takes into account the intensity of radiotracer uptake [22][16].
PBI and IBI were proposed by Takahashi et al [38][20] to quantify the total bone and bone marrow involvement in MM patients. A total segmentation of FDG uptake in bone tissue is needed to calculate PBI and IBI. PBI is similar to an MTV normalized by the total skeletal volume of each patient. This normalization makes PBI less dependent on the patient's height and gender. IBI is calculated as PBI multiplied by its SUVmean. Thus, IBI also takes into account the intensity of radiotracer uptake by the lesions. If PBI is similar to MTV, then the IBI is similar to TLG normalized by the bone and bone marrow volume of the patient.
Other indirect parameters obtained from FDG-PET/CT images, such as visceral adipose tissue glucose uptake and subcutaneous adipose tissue radiodensity, may also be useful to evaluate the prognosis of MM patients.
3. Artificial Intelligence for Estimating Total Metabolic Tumor Volume in Multiple Myeloma
Artificial intelligence (AI) can simulate intellectual work, and its use in nuclear medicine is becoming more and more relevant [63,64][21][22]. AI embraces executing tasks, such as understanding language and pattern recognition, recognizing objects and sounds or problem-solving. Machine learning is a part of AI and is related to the ability to learn from large amounts of data (a set of lessons) [65][23]. Recently, Yan et al. [66][24] demonstrated that machine learning models derived from routine laboratory results can accurately diagnose MM and can increase the rate of early diagnosis.
Deep learning is another important part of AI and refers to any neural network with more than one hidden layer (not a primarily input set of data). Hidden layers ultimately generate an output layer, which can perform standard classification/regression tasks. Convolutional neural networks (CNN) can work with visual data and process imaging information in much more detail than human capacity. CNN-based approaches have been demonstrated to effectively diagnose MM based exclusively on mass spectrometry data from peripheral blood [67][25].
Total tumor burden evaluation is not easily implemented in clinical practice because the exact identification and segmentation of each tumoral lesion to measure these indexes is time-consuming and is sometimes very challenging (multiple and disseminated lesions). The use of AI in PET images of patients with MM is still in its first steps. Morvan et al. [69] [26] demonstrated that random survival forest radiomics analysis in MM patients reduced the errors of the predicted progression, increasing the predictive value of FDG-PET/CT in this scenario. Future studies are necessary to demonstrate in MM patients whether Al will be used as an aide for the interpreting physician by removing tedious and repetitive tasks of identification and classification of all lesions suspicious for malignancy while providing potentially accurate measurement of whole-body tumor burden [70][27].
4. Other Radiotracers Used for Multiple Myeloma
Most of the molecular imaging data currently available in MM is based on studies using FDG, a glucose analog. Therefore, all quantitative methods used to evaluate FDG-PET/CT are, of course, exclusively quantifying glucose metabolism. However, several other radiopharmaceuticals have been proposed to study MM.
Single-photon emission computed tomography (SPECT)/CT using 99mTc-sestamibi (MIBI)—which is related to mitochondrial activity—has been demonstrated to be more efficient than FDG-PET/CT for detecting the diffuse involvement of bone marrow in MM [71] [28]. 68Ga-labeled prostate-specific membrane antigen (PSMA) PET/CT can also detect MM lesions, probably by evidencing neoangiogenesis in the lesions [72,73][29][30] (Figure 71).
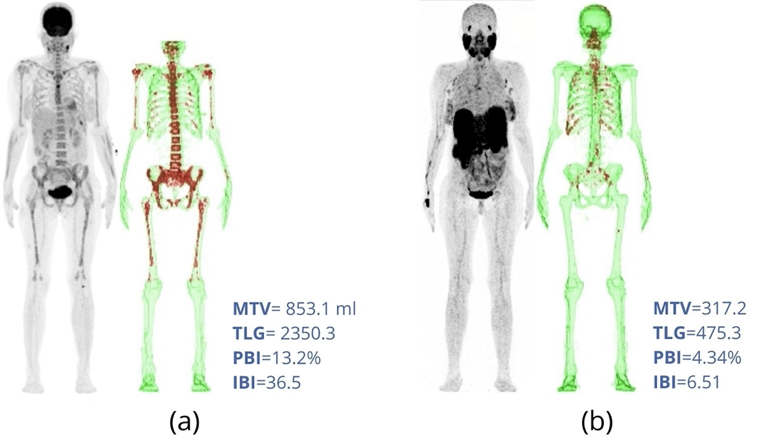
Figure 71. FDG-PET/CT (a) and 68Ga-PSMA PET/CT (b) of a 47-year-old female patient with bone involvement by multiple myeloma. The time interval between the exams was three days. The volumes of interest (VOIs) used for bone segmentation are highlighted in green. For FDG-PET/CT, the fixed threshold used for lesion segmentation was the mean hepatic uptake plus two standard deviations (SUV = 2.00). For PSMA-PET/CT, it was the mean uptake of the left atrium (blood pool) plus two standard deviations (SUV = 1.08). The bone and bone marrow areas in which radiotracer uptake is above the fixed threshold are highlighted in red. The quantitative parameters MTV, TLG, PBI and IBI are shown on the right of the images. Note that diffuse FDG uptake in bone tissue (a) was not detected by PSMA examination (b). However, a higher number of rib lesions were detected by PSMA (b) than by FDG (a) image. Moreover, note that it is not necessary to exclude the skull region for automatic contour of the VOI in the bone tissue for PSMA-PET/CT (b) because there is no physiological uptake of this tracer in the brain.
68Ga-Pentixafor is a new PET tracer with a high affinity for the chemokine receptor-4 (CXCR4), which is highly expressed in several hematologic malignancies. It seems to have greater positivity than FDG in MM [74][31]. Old PET tracers such as 11C-choline and 11C-methionine have also been used to study MM [75][32].
Choline is a component of phosphatidylcholine; therefore, 11C-choline is an indicator of plasma membrane synthesis. The radiolabeled amino acid methionine is supposed to be rapidly incorporated into newly synthesized immunoglobulins in MM lesions [75][32].
3′-Deoxy-3′-[18F]-fluorothymidine (FLT) is used to image DNA synthesis and indirectly evaluate cell proliferation. FLT-PET/CT has been proposed as a possible adjunct in the prognostic evaluation of MM patients. PET/CT using a somatostatin receptor expression marker—68Ga-DOTATATE—has also been shown to detect MM with an efficacy similar to that of FDG-PET/CT in a lesion-based analysis [76][33].
CD38 is a glycoprotein highly specific for MM, and anti-CD38 antibodies (e.g., daratumumab) have been successfully used to treat the disease [77][34]. Currently, CD38-based radiotracers for PET/CT imaging are also under evaluation [78,79,80][35][36][37].
It is interesting and intriguing that radiopharmaceuticals that represent such diverse metabolic aspects can identify the same disease. Generally, different tracers present different uptake intensities in different lesions of the same MM patient [71,74,75] [28][31][32]. The entirely distinct uptake mechanisms of these radiopharmaceuticals suggest that this is related to the very heterogeneous biological behavior of this disease. Cytogenetic analyses have shown that MM is not a single disease, but has unique characteristics at the molecular level in each patient [81] [38]. Therefore, the same volumetric quantitative methods described here for FDG-PET/CT can potentially be used for several other radiopharmaceuticals. Comparison of metabolic volumes of various tracers that represent different metabolic aspects of the disease could have clinical and prognostic implications. Possibly, this would contribute to the understanding of the already demonstrated expressive inter-patient and intra-lesion heterogeneity of MM [82][39].
References
- Laubach, J.; Richardson, P.; Anderson, K. Multiple myeloma. Annu Rev. Med. 2011, 62, 249–264.
- Hungria, V.; Maiolino, A.; Martinez, G.; Colleoni, G.; Coelho, E.; Rocha, L.; Nunes, R.; Bittencourt, R.; Oliveira, L.; Faria, R.; et al. Confirmation of the utility of the International Staging System and identification of a unique pattern of disease in Brazilian patients with multiple myeloma. Haematologica 2008, 93, 791–792.
- Kyle, R.; Child, J.; Anderson, K.; Barlogie, B.; Bataille, R.; Bensinger, W.; Blade, J.; Boccadoro, M.; Dalton, W.; Dimopoulos, M.; et al. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: A report of the International Myeloma Working Group. Br. J. Haematol. 2003, 121, 749–757.
- Hillengass, J.; Usmani, S.; Rajkumar, S.V.; Durie, B.G.M.; Mateos, M.-V.; Lonial, S.; Joao, C.; Anderson, K.C.; García-Sanz, R.; Riva, E. International myeloma working group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019, 20, e302–e312.
- Spinnato, P.; Bazzocchi, A.; Brioli, A.; Nanni, C.; Zamagni, E.; Albisinni, U.; Cavo, M.; Fanti, S.; Battista, G.; Salizzoni, E. Contrast enhanced MRI and 18F-FDG PET-CT in the assessment of multiple myeloma: A comparison of results in different phases of the disease. Eur. J. Radiol. 2012, 81, 4013–4018.
- Derlin, T.; Weber, C.; Habermann, C.R.; Herrmann, J.; Wisotzki, C.; Ayuk, F.; Wolschke, C.; Klutmann, S.; Kröger, N. 18 F-FDG PET/CT for detection and localization of residual or recurrent disease in patients with multiple myeloma after stem cell transplantation. Eur. J. Nucl. Med. Mol. Imaging 2012, 39, 493–500.
- Bertamini, L.; D’Agostino, M.; Gay, F. MRD Assessment in Multiple Myeloma: Progress and Challenges. Curr. Hematol. Malig. Rep. 2021, 16, 162–171.
- Zamagni, E.; Nanni, C.; Dozza, L.; Carlier, T.; Bailly, C.; Tacchetti, P.; Versari, A.; Chauvie, S.; Gallamini, A.; Gamberi, B. Standardization of 18F-FDG–PET/CT According to Deauville Criteria for Metabolic Complete Response Definition in Newly Diagnosed Multiple Myeloma. J. Clin. Oncol. 2021, 39, 116–125.
- Zamagni, E.; Patriarca, F.; Nanni, C.; Zannetti, B.; Englaro, E.; Pezzi, A.; Tacchetti, P.; Buttignol, S.; Perrone, G.; Brioli, A. Prognostic relevance of 18-F FDG PET/CT in newly diagnosed multiple myeloma patients treated with up-front autologous transplantation. Blood J. Am. Soc. Hematol. 2011, 118, 5989–5995.
- Nanni, C.; Versari, A.; Chauvie, S.; Bertone, E.; Bianchi, A.; Rensi, M.; Bellò, M.; Gallamini, A.; Patriarca, F.; Gay, F. Interpretation criteria for FDG PET/CT in multiple myeloma (IMPeTUs): Final results. IMPeTUs (Italian myeloma criteria for PET USe). Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 712–719.
- Nanni, C.; Zamagni, E.; Versari, A.; Chauvie, S.; Bianchi, A.; Rensi, M.; Bellò, M.; Rambaldi, I.; Gallamini, A.; Patriarca, F.; et al. Image interpretation criteria for FDG PET/CT in multiple myeloma: A new proposal from an Italian expert panel. IMPeTUs (Italian Myeloma criteria for PET USe). Eur J. Nucl Med. Mol. Imaging 2016, 43, 414–421.
- Sollini, M.; Bandera, F.; Kirienko, M. Quantitative imaging biomarkers in nuclear medicine: From SUV to image mining studies. Highlights from annals of nuclear medicine 2018. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2737–2745.
- Stolzenburg, A.; Lückerath, K.; Samnick, S.; Speer, M.; Kneer, K.; Schmid, J.-S.; Grigoleit, G.U.; Hofmann, S.; Beer, A.J.; Bunjes, D. Prognostic value of FDG-PET/CT in multiple myeloma patients before and after allogeneic hematopoietic cell transplantation. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 1694–1704.
- Fonti, R.; Larobina, M.; Del Vecchio, S.; De Luca, S.; Fabbricini, R.; Catalano, L.; Pane, F.; Salvatore, M.; Pace, L. Metabolic tumor volume assessed by 18F-FDG PET/CT for the prediction of outcome in patients with multiple myeloma. J. Nucl. Med. 2012, 53, 1829–1835.
- McDonald, J.E.; Kessler, M.M.; Gardner, M.W.; Buros, A.F.; Ntambi, J.A.; Waheed, S.; van Rhee, F.; Zangari, M.; Heuck, C.J.; Petty, N. Assessment of total lesion glycolysis by 18F FDG PET/CT significantly improves prognostic value of GEP and ISS in myeloma. Clin. Cancer Res. 2017, 23, 1981–1987.
- Terao, T.; Machida, Y.; Tsushima, T.; Miura, D.; Narita, K.; Kitadate, A.; Takeuchi, M.; Matsue, K. Pre-treatment metabolic tumour volume and total lesion glycolysis are superior to conventional positron-emission tomography/computed tomography variables for outcome prediction in patients with newly diagnosed multiple myeloma in clinical practice. Br. J. Haematol. 2020, 191, 223–230.
- Bailly, C.; Carlier, T.; Jamet, B.; Eugene, T.; Touzeau, C.; Attal, M.; Hulin, C.; Facon, T.; Leleu, X.; Perrot, A. Interim PET analysis in first-line therapy of multiple myeloma: Prognostic value of δSUVmax in the FDG-avid patients of the IMAJEM study. Clin. Cancer Res. 2018, 24, 5219–5224.
- Starmans, M.P.A.; van der Voort, S.R.; Tovar, J.M.C.; Veenland, J.F.; Klein, S.; Niessen, W.J. Radiomics: Data mining using quantitative medical image features. In Handbook of Medical Image Computing and Computer Assisted Intervention; Elsevier: Amsterdam, The Netherlands, 2020; pp. 429–456.
- Foster, B.; Bagci, U.; Mansoor, A.; Xu, Z.; Mollura, D.J. A review on segmentation of positron emission tomography images. Comput. Biol. Med. 2014, 50, 76–96.
- Duarte, P.S.; Sapienza, M.T. Letter to the Editor: It is time for the nuclear medicine community to define a unit for the total lesion glycolysis (TLG) and similar metrics. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2312–2313.
- Currie, G.M. Intelligent imaging: Artificial intelligence augmented nuclear medicine. J. Nucl. Med. Technol. 2019, 47, 217–222.
- Seifert, R.; Weber, M.; Kocakavuk, E.; Rischpler, C.; Kersting, D. Artificial intelligence and machine learning in nuclear medicine: Future perspectives. Semin. Nucl. Med. 2021, 51, 170–177.
- de Souza-Filho, E.M.; de Amorim Fernandes, F. Deep Learning and Artificial Intelligence in Nuclear Cardiology. In Nuclear Cardiology: Basic and Advanced Concepts in Clinical Practice; Mesquita, C.T., Rezende, M.F., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2021; pp. 741–762.
- Yan, W.; Shi, H.; He, T.; Chen, J.; Wang, C.; Liao, A.; Yang, W.; Wang, H. Employment of Artificial Intelligence Based on Routine Laboratory Results for the Early Diagnosis of Multiple Myeloma. Front. Oncol. 2021, 11, 608191.
- Deulofeu, M.; Kolarova, L.; Salvado, V.; Pena-Mendez, E.; Almasi, M.; Stork, M.; Pour, L.; Boadas-Vaello, P.; Sevcikova, S.; Havel, J.; et al. Rapid discrimination of multiple myeloma patients by artificial neural networks coupled with mass spectrometry of peripheral blood plasma. Sci. Rep. 2019, 9, 7975.
- Jamet, B.; Morvan, L.; Nanni, C.; Michaud, A.; Bailly, C.; Chauvie, S.; Moreau, P.; Touzeau, C.; Zamagni, E.; Bodet-Milin, C.; et al. Random survival forest to predict transplant-eligible newly diagnosed multiple myeloma outcome including FDG-PET radiomics: A combined analysis of two independent prospective European trials. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1005–1015.
- Froelich, J.; Salavati, A. Artificial Intelligence in PET/CT Is about to Make Whole-Body Tumor Burden Measurements a Clinical Reality. Radiology 2020, 294, 453–454.
- Mosci, C.; Pericole, F.; Oliveira, G.; Delamain, M.; Takahashi, M.; Carvalheira, J.; Etchebehere, E.; Santos, A.; Miranda, E.; Lima, M.; et al. Tc-99m-sestamibi SPECT/CT and(18)F-FDG-PET/CT have similar performance but different imaging patterns in newly diagnosed multiple myeloma. Nucl. Med. Commun. 2020, 41, 1081–1088.
- Biggi Mattiolli, A.; Lima, M.C.L.; Camacho, M.; Ramos, C.D.; Santos, A.O.; Etchebehere, E. 68Ga-PSMA PET/CT whole-body tumor burden in patients with biochemical recurrence of prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, S307.
- Takahashi, M.E.S.; De Souza, S.; Frasson, F.C.; Pericole, F.; Ramos, C.D. Skeletal MTV Comparison of 68Ga-PSMA PET-CT with 18F-FDG PET-CT for Multiple Myeloma Patients. In Proceedings of the International Conference on Clinical PET-CT and Molecular Imaging in the Era of Theranostics (IPET-2020), Virtual, 24–26 November 2020; pp. 72–73.
- Kuyumcu, S.; Isik, E.G.; Tiryaki, T.O.; Has-Simsek, D.; Sanli, Y.; Buyukkaya, F.; Özkan, Z.G.; Kalayoglu-Besisik, S.; Unal, S.N. Prognostic significance of 68Ga-Pentixafor PET/CT in multiple myeloma recurrence: A comparison to 18F-FDG PET/CT and laboratory results. Ann. Nucl. Med. 2021, 35, 1147–1156.
- Matteucci, F.; Paganelli, G.; Martinelli, G.; Cerchione, C. PET/CT in Multiple Myeloma: Beyond FDG. Front. Oncol. 2021, 10.
- Sonmezoglu, K.; Vatankulu, B.; Elverdi, T.; Akyel, R.; Erkan, M.E.; Halac, M.; Ocak, M.; Demirci, E.; Aydin, Y. The role of 68Ga-DOTA-TATE PET/CT scanning in the evaluation of patients with multiple myeloma: Preliminary results. Nucl. Med. Commun. 2017, 38, 76–83.
- Nooka, A.K.; Kaufman, J.L.; Hofmeister, C.C.; Joseph, N.S.; Heffner, T.L.; Gupta, V.A.; Sullivan, H.C.; Neish, A.S.; Dhodapkar, M.V.; Lonial, S. Daratumumab in multiple myeloma. Cancer 2019, 125, 2364–2382.
- Ulaner, G.A.; Sobol, N.B.; O’Donoghue, J.A.; Kirov, A.S.; Riedl, C.C.; Min, R.; Smith, E.; Carter, L.M.; Lyashchenko, S.K.; Lewis, J.S. CD38-targeted immuno-PET of multiple myeloma: From xenograft models to first-in-human imaging. Radiology 2020, 295, 606–615.
- Krishnan, A.; Adhikarla, V.; Poku, E.K.; Palmer, J.; Chaudhry, A.; Biglang-awa, V.E.; Bowles, N.; Nathwani, N.; Rosenzweig, M.; Sahebi, F. Identifying CD38+ cells in patients with multiple myeloma: First-in-human imaging using copper-64–labeled daratumumab. Blood Adv. 2020, 4, 5194–5202.
- Wang, C.; Chen, Y.; Hou, Y.N.; Liu, Q.; Zhang, D.; Zhao, H.; Zhang, Y.; An, S.; Li, L.; Hou, J. ImmunoPET imaging of multiple myeloma with Ga-NOTA-Nb1053. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 2749–2760.
- Sawyer, J.R. The prognostic significance of cytogenetics and molecular profiling in multiple myeloma. Cancer Genet. 2011, 204, 3–12.
- Rasche, L.; Kortüm, K.M.; Raab, M.S.; Weinhold, N. The impact of tumor heterogeneity on diagnostics and novel therapeutic strategies in multiple myeloma. Int. J. Mol. Sci. 2019, 20, 1248.