Swallowing is a physiological process that transports ingested foods, liquids, and saliva from the oral cavity into the stomach. Difficulty in the oropharyngeal swallowing process or oropharyngeal dysphagia is a major health problem. There is no established pharmacological therapy for the management of oropharyngeal dysphagia. Studies have suggested that the current clinical management of oropharyngeal dysphagia has limited effectiveness for recovering swallowing physiology and for promoting neuroplasticity in swallowing-related neuronal networks. The peripheral chemical neurostimulation strategy is one of the innovative strategies, and targets chemosensory ion channels expressed in peripheral swallowing-related regions. A considerable number of animal and human studies, including randomized clinical trials in patients with oropharyngeal dysphagia, have reported improvements in the efficacy, safety, and physiology of swallowing using this strategy. There is also evidence that neuroplasticity is promoted in swallowing-related neuronal networks with this strategy. The targeting of chemosensory ion channels in peripheral swallowing-related regions may therefore be a promising pharmacological treatment strategy for the management of oropharyngeal dysphagia.
- oropharyngeal dysphagia
- chemosensory ion channels
- peripheral chemical neurostimulation strategy
Dear author, the following contents are excerpts from your papers. They are editable.
1. Introduction
(Due to the lack of relevant professional knowledge, our editors cannot complete a complete entry by summarizing your paper, so if you are interested in this work. you may need to write some contents by yourself. A good entry will better present your ideas, research and results to other scholars. Readers will also be able to access your paper directly through entries.)
1. Introduction
Difficulties inifficulties in the process of swallowing are termed dysphagia. Swallowing difficulties often lead to severe complications, such as pulmonary aspiration, malnutrition, dehydration, and pneumonia, which have high mortality rates [1][2][3][4][5][6][7]. Generally, dysphagia is divided into oropharyngeal and esophageal subtypes based on the location of the swallowing difficulty [8][9][10]. In oropharyngeal dysphagia, difficulty arises when transporting the food bolus or liquid from the oral cavity to the esophagus, while in esophageal dysphagia, the impedance occurs in the esophagus itself [7][8][9][10]. Oropharyngeal dysphagia is more prevalent and more severe than esophageal dysphagia [11]. In oropharyngeal dysphagia, patients have difficulties with evoking swallowing. Triggering of the swallow is often delayed, leading to impaired safety of swallowing. If the swallow response is not evoked at the correct time, the airways may remain open during swallowing. This can allow the entry of food particles or liquids into the laryngeal vestibule above the vocal folds (termed penetration,) or even deep into the airway below the vocal folds (termed aspiration), and may lead to aspiration pneumonia[12][13]. Airway penetration and aspiration are caused by a delayed laryngeal vestibule closure time and slow hyoid motion [1][14]. Impaired safety of swallowing with bolus penetration occurs in more than half of all patients with oropharyngeal dysphagia, and approximately 20–25% of these patients present aspiration into the airway [1][15][16]. The inability to swallow efficiently can also lead to the presence of bolus residues in the oropharyngeal region (termed oropharyngeal residues), which causes the sensation of having food stuck in the oral cavity or throat regions [17][18]. Oropharyngeal residues occur because of weak bolus propulsion forces and impaired pharyngeal clearance [1][14].
There are many causes of oropharyngeal dysphagia, including neurovascular accidents (e.g., stroke or head injury), neurodegenerative diseases (e.g., Parkinson’s disease, dementia, amyotrophic lateral sclerosis, multiple sclerosis, or Alzheimer’s disease), neuromuscular problems (e.g., polymyositis/dermatomyositis or myasthenia gravis), and local lesions (e.g., head and neck tumors, surgical resection of the oropharynx/larynx, or radiation injury) [17][18][19]. More than half of all stroke patients and around 30% of traumatic brain injury patients develop some kind of swallowing dysfunction. In addition, approximately 50–80% of patients with Parkinson’s disease, Alzheimer’s disease, and dementia have oropharyngeal dysphagia [7][13][20][21][22]. Many older people also develop oropharyngeal dysphagia [17][18][23][24][25][26]. The prevalence of oropharyngeal dysphagia among institutionalized aged patients is more than 50%, while it is approximately 30% among the general older population [3][4][5][6][7][27][28][29][30].
2. Management of Oropharyngeal Dysphagia
2.1 Compensatory Strategies and Swallowing Exercises/Maneuvers
There is no established pharmacological therapy for the management of oropharyngeal dysphagia [31][32]. Currently, its clinical management is mainly focused on compensatory strategies and swallowing exercises/maneuvers [23][33][34][35]. Common compensatory strategies include modification of the properties of the bolus to be swallowed (e.g., changing the volume, viscosity, or texture of the bolus), and the adoption of different postures before swallowing (e.g., chin tuck or head tilt) [23][33][34][35][36][37][38]. Such compensatory strategies are short-term adjustments that aim to compensate for the swallowing difficulty, but they do not usually change the impaired swallowing physiology or promote the recovery of swallowing function in patients with oropharyngeal dysphagia [33][34][37][38][39]. Thickeners are often used to increase the viscosity of the bolus, to reduce penetration or aspiration [14][16][40]. Although, increasing the viscosity of the bolus using thickeners can improve swallowing safety, studies have reported that it also increases the amount of oropharyngeal residue [14][16][41][42][43]. Thickeners also have poor palatability, leading to poor compliance by patients [16][41]. Increasing the bolus volume has been reported to increase penetration and aspiration, along with increased amounts of oral [44] and pharyngeal residues, during swallowing in neurogenic oropharyngeal dysphagia patients [14][44]. Some common swallowing exercises/maneuvers include tongue exercises, jaw exercises, effortful swallow exercises, and Mendelsohn maneuvers (voluntarily holding the larynx in an elevated position). The aims of these exercises/maneuvers are to improve the efficacy of swallowing-related muscles, improve the motion of the bolus, and promote modest neuroplastic changes (i.e., the reorganization of neural connections) [34][36][37][38]. Although both compensatory strategies and swallowing exercises/maneuvers are widely used in clinical practice, the evidence to support their effectiveness is often limited [14][16][34][36][37][38][40][45][46][47][48].
2.2 Neurostimulation or Sensory Stimulation Strategies
In addition to compensatory strategies and swallowing exercises/maneuvers, neurostimulation or sensory stimulation strategies have also been investigated for the management of oropharyngeal dysphagia, although they have not yet become part of mainstream clinical practice [34][36][45][46][47][48][49]. In these strategies, stimuli are applied to central (cortical) or peripheral swallowing-related regions. In central neurostimulation strategies, transcranial magnetic stimulation, or transcranial direct current stimulation is applied to the brain to activate the swallowing-related motor cortex and corticobulbar pathways [34][50][51][52][53][54]. These strategies have shown promising results in stroke patients with oropharyngeal dysphagia [50][51][52][53][55][56]; however, to conduct these therapies (especially transcranial magnetic stimulation), specific and expensive equipment and well-trained professionals are required [57][58]. In peripheral neurostimulation/sensory stimulation strategies, various types of sensory stimuli (e.g., mechanical, thermal, electrical, or chemical) are applied to the oropharyngeal regions. These stimuli increase the sensory inputs to the swallowing center of the brainstem, as well as to the swallowing-related sensory cortex via the sensory nerves that innervate these regions, and thus improve swallowing function [34][49][59][60][61].
3.Targeting Chemosensory Ion Channels to Improve Swallowing Function
Table 1. Animal studies investigating the effects of targeting chemosensory ion channels on swallowing.
|
Targeting Channels |
Agonists and Its Application |
Animals |
Mode of Application |
Effects on Swallowing |
Ref. |
|
TRPV1 |
Capsaicin solution (25 μM) into the laryngopharynx and associated laryngeal regions |
Rats |
Acute |
1. Capsaicin triggered a greater number of swallowing reflexes compared to distilled water/saline/vehicle; 2. Capsaicin shortened the intervals between the evoked swallowing reflexes compared to distilled water/saline/vehicle; 3. Prior topical application of a TRPV1 antagonist significantly reduced the number of capsaicin-induced swallowing reflexes and lengthened the intervals between the |
[62] |
|
Capsaicin solution (10 μM) into the larynx |
Guinea pigs |
Acute |
Capsaicin triggered a greater number of swallowing reflexes compared to saline. |
[63] |
|
|
Capsaicin solution (10 μM) on the vocal folds |
Rats |
Acute |
Capsaicin triggered a considerable number of swallowing reflexes. |
||
|
Capsaicin solution (600 nM) into the pharyngolaryngeal region |
Rats (a |
Acute |
Capsaicin improved the triggering of swallowing reflexes compared to that of distilled water. |
[66] |
|
|
TRPM8 |
Menthol solution (50 mM) into the laryngopharynx and associated laryngeal regions |
Rats |
Acute |
1. Menthol triggered a greater number of swallowing reflexes compared to distilled water/saline/vehicle; 2. Menthol shortened the intervals between the evoked reflexes compared to distilled water/saline/vehicle; 3. Prior topical application of a TRPM8 antagonist significantly reduced the number of menthol-induced swallowing reflexes and lengthened the intervals between the evoked reflexes. |
[62] |
|
ASIC3 |
Guanidine-4-methylquinazoline (GMQ) solution (0.5 to 10 mM) into the laryngopharynx and associated |
Rats |
Acute |
1. GMQ dose-dependently facilitated the triggering of swallowing reflex; 2. Prior topical application of an ASIC3 antagonist significantly reduced the number of GMQ-induced swallowing reflexes and lengthened the intervals between the evoked reflexes. |
[67] |
|
Agmatine (50 mM to 2 M) solutions into the laryngopharynx and associated |
Rats |
Acute |
1. Agmatine dose-dependently facilitated the triggering of swallowing reflex; 2. Prior topical application of an ASIC3 antagonist significantly reduced the number of agmatine-induced swallowing reflexes and lengthened the intervals between the |
[67] |
|
|
ASICs and TRPV1 |
Acetic acid (5 to 30 mM), citric acid (5 to 30 mM) solutions into the pharyngolaryngeal region |
Rats |
Acute |
Acetic acid and citric acid evoked a greater number of swallowing reflexes compared to distilled water. |
[68] |
|
Citric acid solution (10 mM) into the pharyngolaryngeal region |
Rats (a |
Acute |
Citric acid solution improved the triggering swallowing reflexes compared to that of distilled water. |
[66] |
Table 2. Human studies investigating the effects of targeting chemosensory ion channels on swallowing.
|
Targeting Channels |
Agonists and Its Application |
Patients/Participants |
Mode of Application |
Effects on Swallowing |
Ref. |
|
TRPV1 |
Capsaicin (1 nM to 1 μM) solution into the pharyngeal region |
Aged patients with cerebrovascular diseases or dementia presenting oropharyngeal dysphagia |
Acute |
Capsaicin solution dose-dependently reduced the latency to trigger a swallow response. |
[69] |
|
Capsaicinoid (150 μM) containing nectar |
Aged patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Upper esophageal sphincter opening time during swallowing reduced; 3. Time for maximal vertical movement of the hyoid bone and larynx during 4. Prevalence of laryngeal penetration during 5. Prevalence of pharyngeal residue of bolus during swallowing reduced. |
[39] |
|
|
Capsaicinoid (150 μM) containing nectar |
Aged/stroke/neurodegenerative disease patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Prevalence of laryngeal penetration during 3. Prevalence of pharyngeal residue of bolus during swallowing reduced; 4. Bolus propulsion velocity during swallowing increased. |
[43] |
|
|
Capsiate (1–100 nM) into the pharyngeal region |
Patients with history of aspiration pneumonia presenting oropharyngeal dysphagia |
Acute |
Capsiate dose-dependently reduced the latency to trigger a |
[70] |
|
|
Capsaicinoid (10 μM) containing nectar bolus ingestion |
Aged patients presenting oropharyngeal dysphagia |
Chronic (three times/day, before meals for |
1. Laryngeal vestibule closure time during swallowing reduced; 2. Score of the penetration-aspiration scale lowered; 3. Amplitude of cortical sensorial response to pharyngeal electrical stimulation increased; 4. Latency to evoke cortical sensorial response to pharyngeal electrical stimulation decreased. |
[71] |
|
|
Capsaicin containing pickled cabbage (1.5 μg/10 g) ingestion |
Healthy participants |
Chronic (before every major meal/day for 20 days) |
Latency to trigger a swallow response reduced |
[72] |
|
|
Capsaicin containing lozenges (1.5 μg/lozenge) |
Aged patients with cerebrovascular diseases presenting |
Chronic (before every major meal/day for 4 weeks) |
Latency to trigger a swallow response reduced. |
[73] |
|
|
Capsaicin containing thin film food (0.75 μg/film) ingestion |
Aged patients presenting oropharyngeal dysphagia |
Chronic (before every major meal/day for 1 week) |
1. Duration of cervical esophageal opening during 2. Symptoms of oropharyngeal dysphagia reduced; 3. Substance P concentration in saliva increased in patients who showed improvement |
[74] |
|
|
Capsaicin (150 μM) containing nectar bolus ingestion along with cold thermal tactile stimulation |
Aged patients with history of stroke presenting oropharyngeal dysphagia |
Chronic (three times/day, before meals for |
Swallowing function improved assessed by swallowing |
[75] |
|
|
Capsaicinoid (10 μM) containing nectar bolus ingestion |
Aged patients presenting oropharyngeal dysphagia |
Chronic (three times/day, before meals for |
The swallowing safety improved evidenced by reduction of the prevalence of aspiration and lowering the score in |
[76] |
|
|
Capsaicin (0.5 g of 0.025%) containing ointment into the |
Aged patients presenting oropharyngeal dysphagia |
Acute and chronic (once daily for 7 days) |
Swallowing function improved. |
[77] |
|
|
TRPM8 |
Menthol solution (100 μm to 10 mM) into the pharyngeal region |
Aged patients presenting oropharyngeal dysphagia |
Acute |
Menthol dose-dependently reduced the latency to trigger a |
[78] |
|
Menthol (1 and 10 mM) containing nectar |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Prevalence of laryngeal penetration during |
[43] |
|
|
TRPA1 |
Cinnamaldehyde (756.6 μM) and zinc (70 μM) containing nectar bolus ingestion |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Upper esophageal opening time during 3. Score in penetration-aspiration scale lowered; 4. Frequency of safe 5. Latency of evoking cortical response to pharyngeal electrical stimulation shortened. |
[79] |
|
Citral (1.6 mM) containing nectar bolus ingestion |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Upper esophageal opening time during |
[79] |
|
|
TRPV1 and TRPA1 |
Piperine (150 μM and 1 mM) containing nectar |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Time required for maximum anterior extension of hyoid bone during 3. Score in penetration aspiration scale lowered; 4. Prevalence of laryngeal penetration during |
[80] |
|
Black pepper oil (a volatile compound) (100 μL for 1 min) to the nostrils with a paper stick |
Aged patients with cerebrovascular diseases presenting |
Acute |
Latency to trigger a swallow response for distilled water reduced. |
[81] |
|
|
Piperine (150 μM and 1 mM) containing nectar |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Prevalence of penetration during swallowing reduced; 3. Bolus propulsion velocity during swallowing increased. |
[43] |
|
|
Black pepper oil (a volatile compound) (100 μL for 1 min) to the nostrils with a paper stick |
Aged patients with cerebrovascular diseases presenting oropharyngeal dysphagia |
Chronic (three times/day, before meals for |
1. Latency to trigger a swallow response for distilled 2. Serum substance P 3. Regional cerebral blood flow in right orbitofrontal and left insular cortex increased. |
[81] |
|
|
Black pepper oil (a volatile compound) (100 μL for 1 min) to the nostrils with a paper stick |
Pediatric patients with severe neurological disorders often receiving tube feeding |
Chronic (three times/day, before meals for 3 months) |
1. The amount of oral intake of foods by the patients increased; 2. Swallowing-related movements increased. |
[82] |
|
|
TRPV1, TRPA1 |
Vanillin (a volatile compound), (flow rate 7 L/min for 200 ms) delivered ortho-and retro-nasally |
Healthy participants |
Acute |
The frequency of swallowing for continuous intraoral sweet stimuli (glucose) increased in case of retro-nasal delivery. |
[83] |
|
TRPA1 and TRPM8 |
Citral (1.6 mM) and isopulegol (1.3 mM) containing nectar |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
Upper esophageal opening time during swallowing reduced. |
[79] |
|
ASICs and TRPV1 |
Citric acid (2.7% or 128 mM) containing liquid bolus ingestion |
Aged patients with neurological diseases presenting |
Acute |
Prevalence of aspiration and penetration during |
[84] |
|
Lemon juice containing barium liquid bolus (1:1) ingestion |
Patients with strokes and neurological diseases presenting oropharyngeal dysphagia |
Acute |
1. Swallow onset time reduced; 2. Time required to trigger the pharyngeal swallow (pharyngeal delay 3. Frequency of 4. Oropharyngeal swallow efficiency increased. |
[44] |
|
|
Lemon juice containing barium liquid bolus (1:1) ingestion |
Healthy participants and head and neck cancer patients |
Acute |
Pharyngeal transit time reduced. |
[85] |
|
|
Citric acid (80 mM) delivered on the tongue |
Healthy participants |
Acute |
1. Frequency of 2. Hemodynamic responses in the cortical swallowing-related areas prolonged. |
[86] |
|
|
Lemon juice application on the tongue along with nasal inhalation of lemon juice odor |
Healthy participants |
Acute |
Motor evoked potential from the submental muscles increased during volitional swallowing induced by transcranial magnetic stimulation. |
[87] |
|
|
Citric acid solution |
Healthy participants |
Acute |
Activity of submental muscle during swallowing increased. |
[88] |
|
|
Citric acid solution (2.7% or 128 mM) ingestion |
Healthy participants |
Acute |
1. Amplitude of anterior tongue-palate pressure during swallowing increased; 2. Activity of submental muscles during swallowing increased. |
[89] |
|
|
Lemon juice (10%) solution ingestion (4°C before delivery) |
Healthy participants and stroke patients with and without oropharyngeal dysphagia |
Acute |
1. Inter-swallow interval shortened in healthy participants of <60 years of age; 2. Inter-swallow interval unaffected in stroke patients; 3. Velocity and capacity of swallowing reduced both in healthy individuals and |
[90] |
|
|
Lemon juice delivered on tongue |
Healthy participants |
Acute |
1. Number of 2. Salivation increased; 3. Amount of salivation correlated with the number |
[91] |
|
|
Acetic acid (10 and 100 mM) applied on the posterior part of the tongue |
Healthy participants |
Acute |
Latency to trigger swallowing prolonged compared to that |
[92] |
|
|
Citric acid (2.7%) |
Healthy participants |
Acute |
Lingual pressure during |
[93] |
|
|
Citric acid (10%) |
Healthy participants |
Acute |
Speed of swallowing reduced compared to that of water. |
[94] |
|
|
Citric acid containing gelatin cubes (4.4 g of citric acid in 200 ml of gelatin) chewing |
Healthy participants |
Acute |
1. Oral preparation time during swallowing accelerated; 2. Amplitude of submental muscle activity during swallowing increased; 3. Duration of submental muscle activity during |
[95] |
|
|
Lemon water (50%) |
Healthy participants |
Acute |
1. Activity of submental muscles during swallowing increased; 2. Onset time of activation of the submental muscles |
[96] |
|
|
Lemon juice (a drop of 100% lemon juice in the anterior faucial pillar) + cold mechanical stimuli using a probe (around 8–9 °C) before swallowing of water |
Healthy participants |
Acute |
Latency to trigger |
[97] |
|
|
Lemon juice (1:16, mixed with water) ingestion |
Healthy participants |
Acute |
Onset time of activation of the submental and infrahyoid |
[98] |
4. Neurophysiological and Molecular Mechanisms of Improving Swallowing Function via the Activation of Chemosensory Ion Channels by Chemical Stimuli
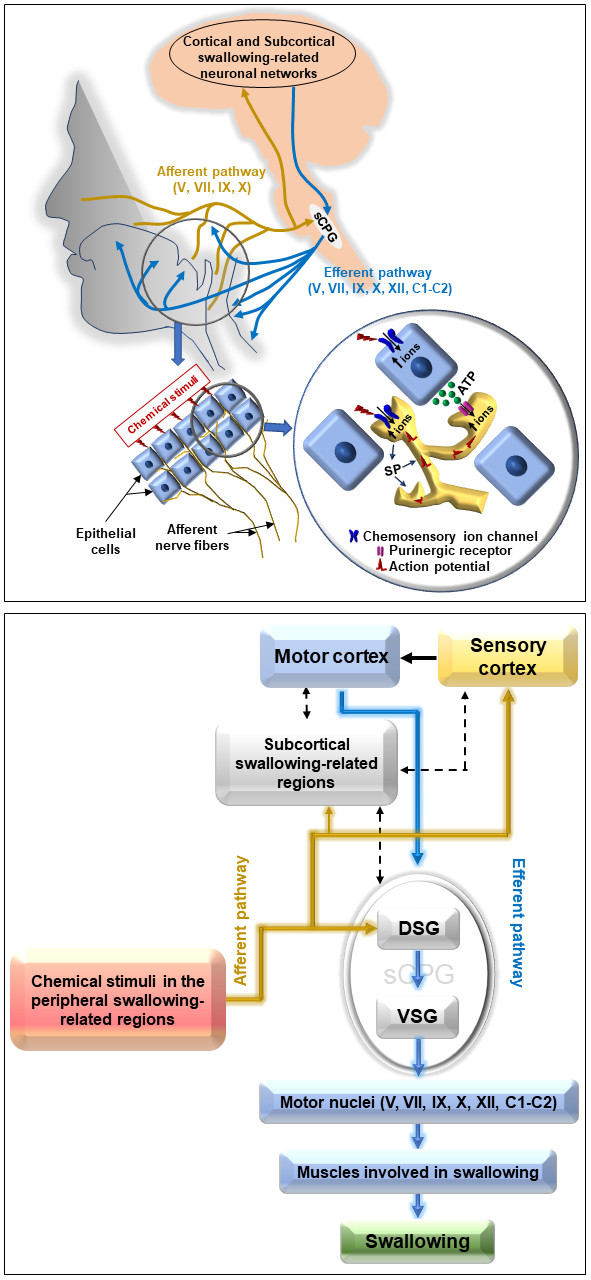
Figure 1. Possible transduction mechanisms and neurophysiological pathways of improving swallowing function via the actions of chemical stimuli applied to peripheral swallowing-related regions. Chemical stimuli applied to peripheral swallowing-related regions can activate chemosensory ion channels expressed in the epithelial cells and nerve fibers in these regions, causing the entry of ions into these structures. The epithelial cells may then release ATP, which can activate purinergic receptors expressed on nearby intra- or sub-epithelial afferent nerve fibers, thus causing the entry of ions into the nerve fibers, leading to the generation of action potentials. Action potentials in the nerve fibers may also be generated by direct ion entry into the nerves through the activation of chemosensory ion channels by chemical stimuli. The action potentials (sensory inputs) then travel via afferent pathways (the V, VII, IX, and X nerves) to the DSG of the sCPG, as well as to the sensory cortex and subcortical swallowing-related regions of the brain. Sensory inputs are then processed by the cortical and subcortical swallowing-related neuronal networks and the sCPG to execute the motor drive for swallowing. The motor output is conveyed to the peripheral swallowing-related muscles through the motor nuclei of the V, VII, IX, X, XII, and C1–C2 nerves. ATP: adenosine triphosphate; DSG: Dorsal swallowing group; SP: Substance P; sCPG: Swallowing central pattern generator; VSG: Ventral swallowing group; V: Trigeminal nerve; VII: Facial nerve; IX: Glossopharyngeal nerve; X: Vagus nerve; XII: Hypoglossal nerve; C1–C2: Cervical nerves 1–2. In the lower part of the figure: Yellow-colored solid lines indicate afferent pathways. Blue-colored solid lines indicate efferent pathways. Black-colored solid line indicates connection between sensory and motor cortex. Black-colored broken lines indicate interconnection among the regions.
5. Conclusion
The advantages of the peripheral chemical neurostimulation strategy are that it does not require specific costly equipment and is relatively cheap and easy to conduct, and patient compliance may also be good. Patients are not required to swallow tablets or capsules; rather, the channel agonists can be mixed with ingestible boluses. Because patients with oropharyngeal dysphagia often face difficulties in swallowing tablets or capsules [3169][9970], this advantage may provide added benefits in terms of patient compliance. In a considerable number of human studies, low concentrations of natural agonists of some TRPs (e.g., capsaicin and piperine) have been mixed with ingestible boluses to improve swallowing functions (Table 2). These natural agonists are phytochemicals found in culinary herbs and spices, and are advantageous because they may not have serious side effects at low concentrations. Many phytochemicals and active compounds of various botanicals can activate TRPs [10071], and therefore have the potential to facilitate swallowing. In future studies, phytochemicals of various botanicals should be investigated in animal and human trials to investigate their potency, specificity, and dose of action to improve swallowing functions. The TRP family has many members, but only TRPV1, TRPA1, and TRPM8 channels have so far been targeted in studies of dysphagia management. The expression of other TRPs (e.g., TRPV2, TRPV4, and TRPM3) has been reported in swallowing-related regions and ganglia [10172][10273][10374][10475]. Thus, the functional roles of these TRPs in swallowing processes need to be investigated in future research, as well as whether they can be targeted for dysphagia management. Along with TRPs, other chemosensory ion channels (e.g., ASICs and purinergic channels) can also be targeted. Highly potent synthetic agonists of these channels can be considered in basic research; however, their safety needs to be assured before they can be used in clinical trials.
Currently, the effect of long-term use of peripheral chemical neurostimulation strategy is unknown. Therefore, whether efficacy is retained in long-term agonist supplementation, and the possible development of adaptation or desensitization, needs to be studied in long-term randomized, controlled, multi-center trials of large numbers of patients with oropharyngeal dysphagia. Understanding the maintenance capability of neuroplasticity over time with short- or mid-term supplementation is also important. Furthermore, patient phenotype is another important issue to be considered. The etiology of oropharyngeal dysphagia and its accompanying health conditions can vary among patients; therefore, same treatment strategy may not be effective for every patient phenotype [36][4976][7677]. Although patient recruitment may be challenging, clinical trials with large numbers of patients with the same phenotypes need to be conducted, to understand the effectiveness of different treatment strategies within the same patient phenotype. Studies combining the peripheral chemosensory ion channel activation strategy with other promising treatment strategies (e.g., cortical neurostimulation or pharyngeal electrical stimulation) may also need to be conducted.
Table 2. Human studies investigating the effects of targeting chemosensory ion channels on swallowing.
|
Targeting Channels |
Agonists and Its Application |
Patients/Participants |
Mode of Application |
Effects on Swallowing |
Ref. |
|
TRPV1 |
Capsaicin (1 nM to 1 μM) solution into the pharyngeal region |
Aged patients with cerebrovascular diseases or dementia presenting oropharyngeal dysphagia |
Acute |
Capsaicin solution dose-dependently reduced the latency to trigger a swallow response. |
[78] |
|
Capsaicinoid (150 μM) containing nectar |
Aged patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Upper esophageal sphincter opening time during swallowing reduced; 3. Time for maximal vertical movement of the hyoid bone and larynx during 4. Prevalence of laryngeal penetration during 5. Prevalence of pharyngeal residue of bolus during swallowing reduced. |
[79] |
|
|
Capsaicinoid (150 μM) containing nectar |
Aged/stroke/neurodegenerative disease patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Prevalence of laryngeal penetration during 3. Prevalence of pharyngeal residue of bolus during swallowing reduced; 4. Bolus propulsion velocity during swallowing increased. |
[80] |
|
|
Capsiate (1–100 nM) into the pharyngeal region |
Patients with history of aspiration pneumonia presenting oropharyngeal dysphagia |
Acute |
Capsiate dose-dependently reduced the latency to trigger a |
[81] |
|
|
Capsaicinoid (10 μM) containing nectar bolus ingestion |
Aged patients presenting oropharyngeal dysphagia |
Chronic (three times/day, before meals for |
1. Laryngeal vestibule closure time during swallowing reduced; 2. Score of the penetration-aspiration scale lowered; 3. Amplitude of cortical sensorial response to pharyngeal electrical stimulation increased; 4. Latency to evoke cortical sensorial response to pharyngeal electrical stimulation decreased. |
[82] |
|
|
Capsaicin containing pickled cabbage (1.5 μg/10 g) ingestion |
Healthy participants |
Chronic (before every major meal/day for 20 days) |
Latency to trigger a swallow response reduced |
[83] |
|
|
Capsaicin containing lozenges (1.5 μg/lozenge) |
Aged patients with cerebrovascular diseases presenting |
Chronic (before every major meal/day for 4 weeks) |
Latency to trigger a swallow response reduced. |
[84] |
|
|
Capsaicin containing thin film food (0.75 μg/film) ingestion |
Aged patients presenting oropharyngeal dysphagia |
Chronic (before every major meal/day for 1 week) |
1. Duration of cervical esophageal opening during 2. Symptoms of oropharyngeal dysphagia reduced; 3. Substance P concentration in saliva increased in patients who showed improvement |
[85] |
|
|
Capsaicin (150 μM) containing nectar bolus ingestion along with cold thermal tactile stimulation |
Aged patients with history of stroke presenting oropharyngeal dysphagia |
Chronic (three times/day, before meals for |
Swallowing function improved assessed by swallowing |
[86] |
|
|
Capsaicinoid (10 μM) containing nectar bolus ingestion |
Aged patients presenting oropharyngeal dysphagia |
Chronic (three times/day, before meals for |
The swallowing safety improved evidenced by reduction of the prevalence of aspiration and lowering the score in |
[87] |
|
|
Capsaicin (0.5 g of 0.025%) containing ointment into the |
Aged patients presenting oropharyngeal dysphagia |
Acute and chronic (once daily for 7 days) |
Swallowing function improved. |
[88] |
|
|
TRPM8 |
Menthol solution (100 μm to 10 mM) into the pharyngeal region |
Aged patients presenting oropharyngeal dysphagia |
Acute |
Menthol dose-dependently reduced the latency to trigger a |
[89] |
|
Menthol (1 and 10 mM) containing nectar |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Prevalence of laryngeal penetration during |
[43] |
|
|
TRPA1 |
Cinnamaldehyde (756.6 μM) and zinc (70 μM) containing nectar bolus ingestion |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Upper esophageal opening time during 3. Score in penetration-aspiration scale lowered; 4. Frequency of safe 5. Latency of evoking cortical response to pharyngeal electrical stimulation shortened. |
[90] |
|
Citral (1.6 mM) containing nectar bolus ingestion |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Upper esophageal opening time during |
[90] |
|
|
TRPV1 and TRPA1 |
Piperine (150 μM and 1 mM) containing nectar |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Time required for maximum anterior extension of hyoid bone during 3. Score in penetration aspiration scale lowered; 4. Prevalence of laryngeal penetration during |
[91] |
|
Black pepper oil (a volatile compound) (100 μL for 1 min) to the nostrils with a paper stick |
Aged patients with cerebrovascular diseases presenting |
Acute |
Latency to trigger a swallow response for distilled water reduced. |
[92] |
|
|
Piperine (150 μM and 1 mM) containing nectar |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
1. Laryngeal vestibule closure time during 2. Prevalence of penetration during swallowing reduced; 3. Bolus propulsion velocity during swallowing increased. |
[43] |
|
|
Black pepper oil (a volatile compound) (100 μL for 1 min) to the nostrils with a paper stick |
Aged patients with cerebrovascular diseases presenting oropharyngeal dysphagia |
Chronic (three times/day, before meals for |
1. Latency to trigger a swallow response for distilled 2. Serum substance P 3. Regional cerebral blood flow in right orbitofrontal and left insular cortex increased. |
[92] |
|
|
Black pepper oil (a volatile compound) (100 μL for 1 min) to the nostrils with a paper stick |
Pediatric patients with severe neurological disorders often receiving tube feeding |
Chronic (three times/day, before meals for 3 months) |
1. The amount of oral intake of foods by the patients increased; 2. Swallowing-related movements increased. |
[93] |
|
|
TRPV1, TRPA1 |
Vanillin (a volatile compound), (flow rate 7 L/min for 200 ms) delivered ortho-and retro-nasally |
Healthy participants |
Acute |
The frequency of swallowing for continuous intraoral sweet stimuli (glucose) increased in case of retro-nasal delivery. |
[94] |
|
TRPA1 and TRPM8 |
Citral (1.6 mM) and isopulegol (1.3 mM) containing nectar |
Aged/stroke/neurodegenerative diseases patients presenting oropharyngeal dysphagia |
Acute |
Upper esophageal opening time during swallowing reduced. |
[90] |
|
ASICs and TRPV1 |
Citric acid (2.7% or 128 mM) containing liquid bolus ingestion |
Aged patients with neurological diseases presenting |
Acute |
Prevalence of aspiration and penetration during |
[95] |
|
Lemon juice containing barium liquid bolus (1:1) ingestion |
Patients with strokes and neurological diseases presenting oropharyngeal dysphagia |
Acute |
1. Swallow onset time reduced; 2. Time required to trigger the pharyngeal swallow (pharyngeal delay 3. Frequency of 4. Oropharyngeal swallow efficiency increased. |
[44] |
|
|
Lemon juice containing barium liquid bolus (1:1) ingestion |
Healthy participants and head and neck cancer patients |
Acute |
Pharyngeal transit time reduced. |
[96] |
|
|
Citric acid (80 mM) delivered on the tongue |
Healthy participants |
Acute |
1. Frequency of 2. Hemodynamic responses in the cortical swallowing-related areas prolonged. |
[97] |
|
|
Lemon juice application on the tongue along with nasal inhalation of lemon juice odor |
Healthy participants |
Acute |
Motor evoked potential from the submental muscles increased during volitional swallowing induced by transcranial magnetic stimulation. |
[98] |
|
|
Citric acid solution |
Healthy participants |
Acute |
Activity of submental muscle during swallowing increased. |
[99] |
|
|
Citric acid solution (2.7% or 128 mM) ingestion |
Healthy participants |
Acute |
1. Amplitude of anterior tongue-palate pressure during swallowing increased; 2. Activity of submental muscles during swallowing increased. |
[100] |
|
|
Lemon juice (10%) solution ingestion (4°C before delivery) |
Healthy participants and stroke patients with and without oropharyngeal dysphagia |
Acute |
1. Inter-swallow interval shortened in healthy participants of <60 years of age; 2. Inter-swallow interval unaffected in stroke patients; 3. Velocity and capacity of swallowing reduced both in healthy individuals and |
[101] |
|
|
Lemon juice delivered on tongue |
Healthy participants |
Acute |
1. Number of 2. Salivation increased; 3. Amount of salivation correlated with the number |
[102] |
|
|
Acetic acid (10 and 100 mM) applied on the posterior part of the tongue |
Healthy participants |
Acute |
Latency to trigger swallowing prolonged compared to that |
[103] |
|
|
Citric acid (2.7%) |
Healthy participants |
Acute |
Lingual pressure during |
[104] |
|
|
Citric acid (10%) |
Healthy participants |
Acute |
Speed of swallowing reduced compared to that of water. |
[105] |
|
|
Citric acid containing gelatin cubes (4.4 g of citric acid in 200 ml of gelatin) chewing |
Healthy participants |
Acute |
1. Oral preparation time during swallowing accelerated; 2. Amplitude of submental muscle activity during swallowing increased; 3. Duration of submental muscle activity during |
[106] |
|
|
Lemon water (50%) |
Healthy participants |
Acute |
1. Activity of submental muscles during swallowing increased; 2. Onset time of activation of the submental muscles |
[107] |
|
|
Lemon juice (a drop of 100% lemon juice in the anterior faucial pillar) + cold mechanical stimuli using a probe (around 8–9 °C) before swallowing of water |
Healthy participants |
Acute |
Latency to trigger |
[108] |
|
|
Lemon juice (1:16, mixed with water) ingestion |
Healthy participants |
Acute |
Onset time of activation of the submental and infrahyoid |
[109] |
References
- Rofes, L.; Arreola, V.; Romea, M.; Palomera, E.; Almirall, J.; Cabré, M.; Serra-Prat, M.; Clavé, P. Pathophysiology of oropharyngeal dysphagia in the frail elderly. Neurogastroenterol. Motil. 2010, 22.
- Carrión, S.; Cabré, M.; Monteis, R.; Roca, M.; Palomera, E.; Serra-Prat, M.; Rofes, L.; Clavé, P. Oropharyngeal dysphagia is a prevalent risk factor for malnutrition in a cohort of older patients admitted with an acute disease to a general hospital. Clin. Nutr. 2015, 34, 436–442.
- Cabre, M.; Serra-Prat, M.; Palomera, E.; Almirall, J.; Pallares, R.; Clavé, P. Prevalence and prognostic implications of dysphagia in elderly patients with pneumonia. Age Ageing 2009, 39, 39–45.
- Ebihara, S.; Sekiya, H.; Miyagi, M.; Ebihara, T.; Okazaki, T. Dysphagia, dystussia, and aspiration pneumonia in elderly people. J. Thorac. Dis. 2016, 8, 632–639.
- Cabré, M.; Serra-Prat, M.; Force, L.; Almirall, J.; Palomera, E.; Clavé, P. Oropharyngeal dysphagia is a risk factor for readmission for pneumonia in the very elderly persons: Observational prospective study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69A, 330–337.
- Manabe, T.; Teramoto, S.; Tamiya, N.; Okochi, J.; Hizawa, N. Risk Factors for Aspiration Pneumonia in Older Adults. PLoS ONE 2015, 10, e0140060.
- Clavé, P.; Rofes, L.; Arreola, V.; Almirall, J.; Cabré, M.; Campins, L.; García-Peris, P.; Speyer, R. Diagnosis and management of oropharyngeal dysphagia and its nutritional and respiratory complications in the elderly. Gastroenterol. Res. Pract. 2011, 2011, 13.
- Koidou, I.; Kollias, N.; Sdravou, K.; Grouios, G. Dysphagia: A Short Review of the Current State. Educ. Gerontol. 2013, 39, 812–827.
- Seaman, W.B. Pharyngeal and Upper Esophageal Dysphagia. JAMA J. Am. Med. Assoc. 1976, 235, 2643–2646.
- Spieker, M.R. Evaluating dysphagia. Am. Fam. Phys. 2000, 61, 3639–3648.
- Clavé, P.; Shaker, R. Dysphagia: Current reality and scope of the problem. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 259–270.
- Jaffer, N.M.; Ng, E.; Au, F.W.F.; Steele, C.M. Fluoroscopic evaluation of oropharyngeal dysphagia: Anatomic, technical, and common etiologic factors. Am. J. Roentgenol. 2015, 204, 49–58.
- Matsuo, K.; Palmer, J.B. Anatomy and Physiology of Feeding and Swallowing: Normal and Abnormal. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 691–707.
- Clavé, P.; De Kraa, M.; Arreola, V.; Girvent, M.; Farré, R.; Palomera, E.; Serra-Prat, M. The effect of bolus viscosity on swallowing function in neurogenic dysphagia. Aliment. Pharmacol. Ther. 2006, 24, 1385–1394.
- Lazarus, C.L. Effects of chemoradiotherapy on voice and swallowing. Curr. Opin. Otolaryngol. Head Neck Surg. 2009, 17, 172–178.
- Newman, R.; Vilardell, N.; Clavé, P.; Speyer, R. Effect of Bolus Viscosity on the Safety and Efficacy of Swallowing and the Kinematics of the Swallow Response in Patients with Oropharyngeal Dysphagia: White Paper by the European Society for Swallowing Disorders (ESSD). Dysphagia 2016, 31, 232–249.
- Cook, I.J. Oropharyngeal Dysphagia. Gastroenterol. Clin. N. Am. 2009, 38, 411–431.
- Bulat, R.S.; Orlando, R.C. Oropharyngeal dysphagia. Curr. Treat. Options Gastroenterol. 2005, 8, 269–274.
- Shaker, R. Oropharyngeal Dysphagia. Gastroenterol. Hepatol. 2006, 2, 633–634.
- Daniels, S. Neurological disorders affecting oral, pharyngeal swallowing. GI Motil. Online 2006, 2210.
- de Souza Oliveira, A.R.; de Sousa Costa, A.G.; Morais, H.C.C.; Cavalcante, T.F.; de Oliveira Lopes, M.V.; de Araujo, T.L. Clinical factors predicting risk for aspiration and respiratory aspiration among patients with Stroke. Rev. Lat. Am. Enferm. 2015, 23, 216–224.
- Kreuzer, S.H.; Schima, W.; Schober, E.; Pokieser, P.; Kofler, G.; Lechner, G.; Denk, D.M. Complications after laryngeal surgery: Videofluoroscopic evaluation of 120 patients. Clin. Radiol. 2000, 55, 775–781.
- Wirth, R.; Dziewas, R.; Beck, A.M.; Clavé, P.; Hamdy, S.; Heppner, H.J.; Langmore, S.; Leischker, A.H.; Martino, R.; Pluschinski, P.; et al. Oropharyngeal dysphagia in older persons—From pathophysiology to adequate intervention: A review and summary of an international expert meeting. Clin. Interv. Aging 2016, 11, 189–208.
- Ortega, O.; Cabre, M.; Clave, P. Oropharyngeal dysphagia: Aetiology and effects of ageing. J. Gastroenterol. Hepatol. Res. 2014, 3, 1049–1054.
- Robbins, J.; Bridges, A.D.; Taylor, A. Oral, pharyngeal and esophageal motor function in aging. GI Motil. Online 2006, 1–21.
- Espinosa-Val, C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, risk factors, and complications of oropharyngeal dysphagia in older patients with dementia. Nutrients 2020, 12, 863.
- Lin, L.C.; Wu, S.C.; Chen, H.S.; Wang, T.G.; Chen, M.Y. Prevalence of impaired swallowing in institutionalized older people in Taiwan. J. Am. Geriatr. Soc. 2002, 50, 1118–1123.
- Bloem, B.R.; Lagaay, A.M.; Van Beek, W.; Haan, J.; Roos, R.A.C.; Wintzen, A.R. Prevalence of subjective dysphagia in community residents aged over 87. Br. Med. J. 1990, 300, 721–722.
- Serra-Prat, M.; Hinojosa, G.; Lõpez, D.; Juan, M.; Fabré, E.; Voss, D.S.; Calvo, M.; Marta, V.; Ribõ, L.; Palomera, E.; et al. Prevalence of oropharyngeal dysphagia and impaired safety and efficacy of swallow in independently living older persons. J. Am. Geriatr. Soc. 2011, 59, 186–187.
- Almirall, J.; Rofes, L.; Serra-Prat, M.; Icart, R.; Palomera, E.; Arreola, V.; Clavé, P. Oropharyngeal dysphagia is a risk factor for community-acquired pneumonia in the elderly. Eur. Respir. J. 2013, 41, 923–926.
- Wirth, R.; Dziewas, R. Dysphagia and pharmacotherapy in older adults. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 25–29.
- Dziewas, R.; Beck, A.M.; Clave, P.; Hamdy, S.; Heppner, H.J.; Langmore, S.E.; Leischker, A.; Martino, R.; Pluschinski, P.; Roesler, A.; et al. Recognizing the Importance of Dysphagia: Stumbling Blocks and Stepping Stones in the Twenty-First Century. Dysphagia 2017, 32, 78–82.
- Cohen, D.L.; Roffe, C.; Beavan, J.; Blackett, B.; Fairfield, C.A.; Hamdy, S.; Havard, D.; McFarlane, M.; McLauglin, C.; Randall, M.; et al. Post-stroke dysphagia: A review and design considerations for future trials. Int. J. Stroke 2016, 11, 399–411.
- Cabib, C.; Ortega, O.; Kumru, H.; Palomeras, E.; Vilardell, N.; Alvarez-Berdugo, D.; Muriana, D.; Rofes, L.; Terré, R.; Mearin, F.; et al. Neurorehabilitation strategies for poststroke oropharyngeal dysphagia: From compensation to the recovery of swallowing function. Ann. N. Y. Acad. Sci. 2016, 1380, 121–138.
- Ortega, O.; Martín, A.; Clavé, P. Diagnosis and Management of Oropharyngeal Dysphagia Among Older Persons, State of the Art. J. Am. Med. Dir. Assoc. 2017, 18, 576–582.
- Martino, R.; McCulloch, T. Therapeutic intervention in oropharyngeal dysphagia. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 665–679.
- Langmore, S.E.; Pisegna, J.M. Efficacy of exercises to rehabilitate dysphagia: A critique of the literature. Int. J. Speech. Lang. Pathol. 2015, 17, 222–229.
- Speyer, R.; Baijens, L.; Heijnen, M.; Zwijnenberg, I. Effects of therapy in oropharyngeal dysphagia by speech and language therapists: A systematic review. Dysphagia 2010, 25, 40–65.
- Rofes, L.; Arreola, V.; Martin, A.; Clavé, P. Natural capsaicinoids improve swallow response in older patients with oropharyngeal dysphagia. Gut 2013, 62, 1280–1287.
- Bisch, E.M.; Logemann, J.A.; Rademaker, A.W.; Kahrilas, P.J.; Lazarus, C.L. Pharyngeal effects of bolus volume, viscosity, and temperature in patients with dysphagia resulting from neurologic impairment and in normal subjects. J. Speech Hear. Res. 1994, 37, 1041–1049.
- Rofes, L.; Arreola, V.; Mukherjee, R.; Swanson, J.; Clavé, P. The effects of a xanthan gum-based thickener on the swallowing function of patients with dysphagia. Aliment. Pharmacol. Ther. 2014, 39, 1169–1179.
- Bhattacharyya, N.; Kotz, T.; Shapiro, J. The effect of bolus consistency on dysphagia in unilateral vocal cord paralysis. Otolaryngol. Head Neck Surg. 2003, 129, 632–636.
- Alvarez-Berdugo, D.; Rofes, L.; Arreola, V.; Martin, A.; Molina, L.; Clavé, P. A comparative study on the therapeutic effect of TRPV1, TRPA1, and TRPM8 agonists on swallowing dysfunction associated with aging and neurological diseases. Neurogastroenterol. Motil. 2018, 30.
- Logemann, J.A.; Pauloski, B.R.; Colangelo, L.; Lazarus, C.; Fujiu, M.; Kahrilas, P.J. Effects of a sour bolus on oropharyngeal swallowing measures in patients with neurogenic dysphagia. J. Speech Hear. Res. 1995, 38, 556–563.
- Mistry, S.; Michou, E.; Vasant, D.H.; Hamdy, S. Direct and Indirect Therapy: Neurostimulation for the Treatment of Dysphagia After Stroke; Springer: Heidelberg, Germany, 2011; pp. 519–538.
- Logemann, J.A. Treatment of Oral and Pharyngeal Dysphagia. Phys. Med. Rehabil. Clin. N. Am. 2008, 19, 803–816.
- Ashford, J.; McCabe, D.; Wheeler-Hegland, K.; Frymark, T.; Mullen, R.; Musson, N.; Schooling, T.; Hammond, C.S. Evidence-based systematic review: Oropharyngeal dysphagia behavioral treatments. Part III—Impact of dysphagia treatments on populations with neurological disorders. J. Rehabil. Res. Dev. 2009, 46, 195–204.
- Bath, P.M.; Lee, H.S.; Everton, L.F. Swallowing therapy for dysphagia in acute and subacute stroke. Cochrane Database Syst. Rev. 2018, 2018.
- Alvarez-Berdugo, D.; Tomsen, N.; Clavé, P. Sensory stimulation treatments for oropharyngeal dysphagia. In Medical Radiology; Springer: Berlin, Germany, 2019; pp. 763–779.
- Wang, Z.; Song, W.Q.; Wang, L. Application of noninvasive brain stimulation for post-stroke dysphagia rehabilitation. Kaohsiung J. Med. Sci. 2017, 33, 55–61.
- Simons, A.; Hamdy, S. The Use of Brain Stimulation in Dysphagia Management. Dysphagia 2017, 32, 209–215.
- Pisegna, J.M.; Kaneoka, A.; Pearson, W.G.; Kumar, S.; Langmore, S.E. Effects of non-invasive brain stimulation on post-stroke dysphagia: A systematic review and meta-analysis of randomized controlled trials. Clin. Neurophysiol. 2016, 127, 956–968.
- Yang, S.N.; Pyun, S.B.; Kim, H.J.; Ahn, H.S.; Rhyu, B.J. Effectiveness of Non-invasive Brain Stimulation in Dysphagia Subsequent to Stroke: A Systemic Review and Meta-analysis. Dysphagia 2015, 30, 383–391.
- Fraser, C.; Power, M.; Hamdy, S.; Rothwell, J.; Hobday, D.; Hollander, I.; Tyrell, P.; Hobson, A.; Williams, S.; Thompson, D. Driving plasticity in human adult motor cortex is associated with improved motor function after brain injury. Neuron 2002, 34, 831–840.
- Khedr, E.M.; Abo-Elfetoh, N.; Rothwell, J.C. Treatment of post-stroke dysphagia with repetitive transcranial magnetic stimulation. Acta Neurol. Scand. 2009, 119, 155–161.
- Papadopoulou, S.L.; Ploumis, A.; Exarchakos, G.; Theodorou, S.; Beris, A.; Fotopoulos, A. Versatility of repetitive transcranial magnetic stimulation in the treatment of poststroke dysphagia. J. Neurosci. Rural Pract. 2018, 9, 391–396.
- Doeltgen, S.H.; Huckabee, M.L. Swallowing neurorehabilitation: From the research laboratory to routine clinical application. Arch. Phys. Med. Rehabil. 2012, 93, 207–213.
- Rossi, S.; Hallett, M.; Rossini, P.M.; Pascual-Leone, A.; Avanzini, G.; Bestmann, S.; Berardelli, A.; Brewer, C.; Canli, T.; Cantello, R.; et al. Safety, ethical considerations, and application guidelines for the use of transcranial magnetic stimulation in clinical practice and research. Clin. Neurophysiol. 2009, 120, 2008–2039.
- Rofes, L.; Cola, P.C.; Clave, P. The effects of sensory stimulation on neurogenic oropharyngeal dysphagia. J. Gastroenterol. Hepatol. Res. 2014, 3, 1066–1072.
- Lowell, S.Y.; Poletto, C.J.; Knorr-Chung, B.R.; Reynolds, R.C.; Simonyan, K.; Ludlow, C.L. Sensory stimulation activates both motor and sensory components of the swallowing system. Neuroimage 2008, 42, 285–295.
- Steele, C.M.; Miller, A.J. Sensory input pathways and mechanisms in swallowing: A review. Dysphagia 2010, 25, 323–333.
- Hossain, M.Z.; Ando, H.; Unno, S.; Masuda, Y.; Kitagawa, J. Activation of TRPV1 and TRPM8 channels in the larynx and associated laryngopharyngeal regions facilitates the swallowing reflex. Int. J. Mol. Sci. 2018, 19, 4113.
- Tsujimura, T.; Udemgba, C.; Inoue, M.; Canning, B.J. Laryngeal and tracheal afferent nerve stimulation evokes swallowing in anaesthetized guinea pigs. J. Physiol. 2013, 591, 4667–4679.
- Tsujimura, T.; Sakai, S.; Suzuki, T.; Ujihara, I.; Tsuji, K.; Magara, J.; Canning, B.J.; Inoue, M. Central inhibition of initiation of swallowing by systemic administration of diazepam and baclofen in anaesthetized rats. Am. J. Physiol. Gastrointest. Liver Physiol. 2017, 312, G498–G507.
- Tsujimura, T.; Ueha, R.; Yoshihara, M.; Takei, E.; Nagoya, K.; Shiraishi, N.; Magara, J.; Inoue, M. Involvement of the epithelial sodium channel in initiation of mechanically evoked swallows in anaesthetized rats. J. Physiol. 2019, 597, 2949–2963.
- Sugiyama, N.; Nishiyama, E.; Nishikawa, Y.; Sasamura, T.; Nakade, S.; Okawa, K.; Nagasawa, T.; Yuki, A. A novel animal model of dysphagia following stroke. Dysphagia 2014, 29, 61–67.
- Hossain, M.Z.; Ando, H.; Unno, S.; Nakamoto, T.; Kitagawa, J. Functional involvement of acid-sensing ion channel 3 in the swallowing reflex in rats. Neurogastroenterol. Motil. 2020, 32.
- Kajii, Y.; Shingai, T.; Kitagawa, J.I.; Takahashi, Y.; Taguchi, Y.; Noda, T.; Yamada, Y. Sour taste stimulation facilitates reflex swallowing from the pharynx and larynx in the rat. Physiol. Behav. 2002, 77, 321–325.
- Ebihara, T.; Sekizawa, K.; Nakazawa, H.; Sasaki, H. Capsaicin and swallowing reflex. Lancet 1993, 341, 432. Wirth, R.; Dziewas, R. Dysphagia and pharmacotherapy in older adults. Curr. Opin. Clin. Nutr. Metab. Care 2019, 22, 25–29.
- Yamasaki, M.; Ebihara, S.; Ebihara, T.; Yamanda, S.; Arai, H.; Kohzuki, M. Effects of capsiate on the triggering of the swallowing reflex in elderly patients with aspiration pneumonia. Geriatr. Gerontol. Int. 2010, 10, 107–109. Masilamoney, M.; Dowse, R. Knowledge and practice of healthcare professionals relating to oral medicine use in swallowing-impaired patients: A scoping review. Int. J. Pharm. Pract. 2018, 26, 199–209.
- Tomsen, N.; Ortega, O.; Rofes, L.; Arreola, V.; Martin, A.; Mundet, L.; Clavé, P. Acute and subacute effects of oropharyngeal sensory stimulation with TRPV1 agonists in older patients with oropharyngeal dysphagia: A biomechanical and neurophysiological randomized pilot study. Therap. Adv. Gastroenterol. 2019, 12. Premkumar, L.S. Transient receptor potential channels as targets for phytochemicals. ACS Chem. Neurosci. 2014, 5, 1117–1130.
- Shin, S.; Shutoh, N.; Tonai, M.; Ogata, N. The Effect of Capsaicin-Containing Food on the Swallowing Response. Dysphagia 2016, 31, 146–153.Sasaki, R.; Sato, T.; Yajima, T.; Kano, M.; Suzuki, T.; Ichikawa, H. The Distribution of TRPV1 and TRPV2 in the rat pharynx. Cell. Mol. Neurobiol. 2013, 33, 707–714, doi:10.1007/s10571-013-9938-3.
- Ebihara, T.; Takahashi, H.; Ebihara, S.; Okazaki, T.; Sasaki, T.; Watando, A.; Nemoto, M.; Sasaki, H. Capsaicin troche for swallowing dysfunction in older people. J. Am. Geriatr. Soc. 2005, 53, 824–828. Sato, D.; Sato, T.; Urata, Y.; Okajima, T.; Kawamura, S.; Kurita, M.; Takahashi, K.; Nanno, M.; Watahiki, A.; Kokubun, S.; et al. Distribution of TRPVs, P2X3, and parvalbumin in the human nodose ganglion. Cell. Mol. Neurobiol. 2014, 34, 851–858, doi:10.1007/s10571-014-0062-9.
- Nakato, R.; Manabe, N.; Shimizu, S.; Hanayama, K.; Shiotani, A.; Hata, J.; Haruma, K. Effects of Capsaicin on Older Patients with Oropharyngeal Dysphagia: A Double-Blind, Placebo-Controlled, Crossover Study. Digestion 2017, 95, 210–220. Yajima, T.; Sato, T.; Shimazaki, K.; Ichikawa, H. Transient receptor potential melastatin-3 in the rat sensory ganglia of the trigeminal, glossopharyngeal and vagus nerves. J. Chem. Neuroanat. 2019, 96, 116–125, doi:10.1016/j.jchemneu.2019.01.005.
- Wang, Z.; Wu, L.; Fang, Q.; Shen, M.; Zhang, L.; Liu, X. Effects of capsaicin on swallowing function in stroke patients with dysphagia: A randomized controlled trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 1744–1751. Zhao, H.; Sprunger, L.K.; Simasko, S.M. Expression of transient receptor potential channels and two-pore potassium channels in subtypes of vagal afferent neurons in rat. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 298, G212, doi:10.1152/ajpgi.00396.2009.
- Ortega, O.; Rofes, L.; Martin, A.; Arreola, V.; López, I.; Clavé, P. A Comparative Study Between Two Sensory Stimulation Strategies After Two Weeks Treatment on Older Patients with Oropharyngeal Dysphagia. Dysphagia 2016, 31, 706–716. Alvarez-Berdugo, D.; Tomsen, N.; Clavé, P. Sensory stimulation treatments for oropharyngeal dysphagia. In Medical Radiology; Springer: Berlin, Germany, 2019; Volume 0, pp. 763–779.
- Kondo, E.; Jinnouchi, O.; Ohnishi, H.; Kawata, I.; Nakano, S.; Goda, M.; Kitamura, Y.; Abe, K.; Hoshikawa, H.; Okamoto, H.; et al. Effects of aural stimulation with capsaicin ointment on swallowing function in elderly patients with non-obstructive dysphagia. Clin. Interv. Aging 2014, 9, 1661–1667. Ortega, O.; Rofes, L.; Martin, A.; Arreola, V.; López, I.; Clavé, P. A Comparative Study Between Two Sensory Stimulation Strategies After Two Weeks Treatment on Older Patients with Oropharyngeal Dysphagia. Dysphagia 2016, 31, 706–716, doi:10.1007/s00455-016-9736-4.
- Ebihara, T.; Ebihara, S.; Watando, A.; Okazaki, T.; Asada, M.; Ohrui, T.; Yamaya, M.; Arai, H. Effects of menthol on the triggering of the swallowing reflex in elderly patients with dysphagia. Br. J. Clin. Pharmacol. 2006, 62, 369–371. Ebihara, T.; Sekizawa, K.; Nakazawa, H.; Sasaki, H. Capsaicin and swallowing reflex. Lancet 1993, 341, 432.
- Tomsen, N.; Alvarez-Berdugo, D.; Rofes, L.; Ortega, O.; Arreola, V.; Nascimento, W.; Martin, A.; Cabib, C.; Bolivar-Prados, M.; Mundet, L.; et al. A randomized clinical trial on the acute therapeutic effect of TRPA1 and TRPM8 agonists in patients with oropharyngeal dysphagia. Neurogastroenterol. Motil. 2020, 32. Rofes, L.; Arreola, V.; Martin, A.; Clavé, P. Natural capsaicinoids improve swallow response in older patients with oropharyngeal dysphagia. Gut 2013, 62, 1280–1287, doi:10.1136/gutjnl-2011-300753.
- Rofes, L.; Arreola, V.; Martin, A.; Clavé, P. Effect of oral piperine on the swallow response of patients with oropharyngeal dysphagia. J. Gastroenterol. 2014, 49, 1517–1523. Alvarez-Berdugo, D.; Rofes, L.; Arreola, V.; Martin, A.; Molina, L.; Clavé, P. A comparative study on the therapeutic effect of TRPV1, TRPA1, and TRPM8 agonists on swallowing dysfunction associated with aging and neurological diseases. Neurogastroenterol. Motil. 2018, 30, doi:10.1111/nmo.13185.
- Ebihara, T.; Ebihara, S.; Maruyama, M.; Kobayashi, M.; Itou, A.; Arai, H.; Sasaki, H. A randomized trial of olfactory stimulation using black pepper oil in older people with swallowing dysfunction. J. Am. Geriatr. Soc. 2006, 54, 1401–1406. Yamasaki, M.; Ebihara, S.; Ebihara, T.; Yamanda, S.; Arai, H.; Kohzuki, M. Effects of capsiate on the triggering of the swallowing reflex in elderly patients with aspiration pneumonia. Geriatr. Gerontol. Int. 2010, 10, 107–109.
- Munakata, M.; Kobayashi, K.; Niisato-Nezu, J.; Tanaka, S.; Kakisaka, Y.; Ebihara, T.; Ebihara, S.; Haginoya, K.; Tsuchiya, S.T.; Onuma, A. Olfactory stimulation using black pepper oil facilitates oral feeding in pediatric patients receiving long-term enteral nutrition. Tohoku J. Exp. Med. 2008, 214, 327–332. Tomsen, N.; Ortega, O.; Rofes, L.; Arreola, V.; Martin, A.; Mundet, L.; Clavé, P. Acute and subacute effects of oropharyngeal sensory stimulation with TRPV1 agonists in older patients with oropharyngeal dysphagia: A biomechanical and neurophysiological randomized pilot study. Therap. Adv. Gastroenterol. 2019, 12, doi:10.1177/1756284819842043.
- Welge-Lüssen, A.; Ebnöther, M.; Wolfensberger, M.; Hummel, T. Swallowing is differentially influenced by retronasal compared with orthonasal stimulation in combination with gustatory stimuli. Chem. Senses 2009, 34, 499–502. Shin, S.; Shutoh, N.; Tonai, M.; Ogata, N. The Effect of Capsaicin-Containing Food on the Swallowing Response. Dysphagia 2016, 31, 146–153, doi:10.1007/s00455-015-9668-4.
- Pelletier, C.A.; Lawless, H.T. Effect of citric acid and citric acid-sucrose mixtures on swallowing in neurogenic oropharyngeal dysphagia. Dysphagia 2003, 18, 231–241. Ebihara, T.; Takahashi, H.; Ebihara, S.; Okazaki, T.; Sasaki, T.; Watando, A.; Nemoto, M.; Sasaki, H. Capsaicin troche for swallowing dysfunction in older people. J. Am. Geriatr. Soc. 2005, 53, 824–828, doi:10.1111/j.1532-5415.2005.53261.x.
- Roa Pauloski, B.; Logemann, J.A.; Rademaker, A.W.; Lundy, D.; Sullivan, P.A.; Newman, L.A.; Lazarus, C.; Bacon, M. Effects of enhanced bolus flavors on oropharyngeal swallow in patients treated for head and neck cancer. Head Neck 2013, 35, 1124–1131.Nakato, R.; Manabe, N.; Shimizu, S.; Hanayama, K.; Shiotani, A.; Hata, J.; Haruma, K. Effects of Capsaicin on Older Patients with Oropharyngeal Dysphagia: A Double-Blind, Placebo-Controlled, Crossover Study. Digestion 2017, 95, 210–220, doi:10.1159/000463382.
- Mulheren, R.W.; Kamarunas, E.; Ludlow, C.L. Sour taste increases swallowing and prolongs hemodynamic responses in the cortical swallowing network. J. Neurophysiol. 2016, 116, 2033–2042. Wang, Z.; Wu, L.; Fang, Q.; Shen, M.; Zhang, L.; Liu, X. Effects of capsaicin on swallowing function in stroke patients with dysphagia: A randomized controlled trial. J. Stroke Cerebrovasc. Dis. 2019, 28, 1744–1751.
- Abdul Wahab, N.; Jones, R.D.; Huckabee, M.L. Effects of olfactory and gustatory stimuli on neural excitability for swallowing. Physiol. Behav. 2010, 101, 568–575. Ortega, O.; Rofes, L.; Martin, A.; Arreola, V.; López, I.; Clavé, P. A Comparative Study Between Two Sensory Stimulation Strategies After Two Weeks Treatment on Older Patients with Oropharyngeal Dysphagia. Dysphagia 2016, 31, 706–716.
- Miura, Y.; Morita, Y.; Koizumi, H.; Shingai, T. Effects of taste solutions, carbonation, and cold stimulus on the power frequency content of swallowing submental surface electromyography. Chem. Senses 2009, 34, 325–331. Kondo, E.; Jinnouchi, O.; Ohnishi, H.; Kawata, I.; Nakano, S.; Goda, M.; Kitamura, Y.; Abe, K.; Hoshikawa, H.; Okamoto, H.; et al. Effects of aural stimulation with capsaicin ointment on swallowing function in elderly patients with non-obstructive dysphagia. Clin. Interv. Aging 2014, 9, 1661–1667.
- Pelletier, C.A.; Steele, C.M. Influence of the perceived taste intensity of chemesthetic stimuli on swallowing parameters given age and genetic taste differences in healthy adult women. J. SpeechLang. Hear. Res. 2014, 57, 46–56. Ebihara, T.; Ebihara, S.; Watando, A.; Okazaki, T.; Asada, M.; Ohrui, T.; Yamaya, M.; Arai, H. Effects of menthol on the triggering of the swallowing reflex in elderly patients with dysphagia. Br. J. Clin. Pharmacol. 2006, 62, 369–371.
- Hamdy, S.; Jilani, S.; Price, V.; Parker, C.; Hall, N.; Power, M. Modulation of human swallowing behaviour by thermal and chemical stimulation in health and after brain injury. Neurogastroenterol. Motil. 2003, 15, 69–77. Tomsen, N.; Alvarez-Berdugo, D.; Rofes, L.; Ortega, O.; Arreola, V.; Nascimento, W.; Martin, A.; Cabib, C.; Bolivar-Prados, M.; Mundet, L.; et al. A randomized clinical trial on the acute therapeutic effect of TRPA1 and TRPM8 agonists in patients with oropharyngeal dysphagia. Neurogastroenterol. Motil. 2020, 32.
- Nederkoorn, C.; Smulders, F.T.Y.; Jansen, A. Recording of swallowing events using electromyography as a non-invasive measurement of salivation. Appetite 1999, 33, 361–369. Rofes, L.; Arreola, V.; Martin, A.; Clavé, P. Effect of oral piperine on the swallow response of patients with oropharyngeal dysphagia. J. Gastroenterol. 2014, 49, 1517–1523.
- Shingai, T.; Miyaoka, Y.; Ikarashi, R.; Shimada, K. Swallowing reflex elicited by water and taste solutions in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1989, 256. Ebihara, T.; Ebihara, S.; Maruyama, M.; Kobayashi, M.; Itou, A.; Arai, H.; Sasaki, H. A randomized trial of olfactory stimulation using black pepper oil in older people with swallowing dysfunction. J. Am. Geriatr. Soc. 2006, 54, 1401–1406.
- Pelletier, C.A.; Dhanaraj, G.E. The effect of taste and palatability on lingual swallowing pressure. Dysphagia 2006, 21, 121–128. Munakata, M.; Kobayashi, K.; Niisato-Nezu, J.; Tanaka, S.; Kakisaka, Y.; Ebihara, T.; Ebihara, S.; Haginoya, K.; Tsuchiya, S.T.; Onuma, A. Olfactory stimulation using black pepper oil facilitates oral feeding in pediatric patients receiving long-term enteral nutrition. Tohoku J. Exp. Med. 2008, 214, 327–332.
- Chee, C.; Arshad, S.; Singh, S.; Mistry, S.; Hamdy, S. The influence of chemical gustatory stimuli and oral anaesthesia on healthy human pharyngeal swallowing. Chem. Senses 2005, 30, 393–400. Welge-Lüssen, A.; Ebnöther, M.; Wolfensberger, M.; Hummel, T. Swallowing is differentially influenced by retronasal compared with orthonasal stimulation in combination with gustatory stimuli. Chem. Senses 2009, 34, 499–502.
- Leow, L.P.; Huckabee, M.L.; Sharma, S.; Tooley, T.P. The influence of taste on swallowing apnea, oral preparation time, and duration and amplitude of submental muscle contraction. Chem. Senses 2007, 32, 119–128.Pelletier, C.A.; Lawless, H.T. Effect of citric acid and citric acid-sucrose mixtures on swallowing in neurogenic oropharyngeal dysphagia. Dysphagia 2003, 18, 231–241.
- Palmer, P.M.; McCulloch, T.M.; Jaffe, D.; Neel, A.T. Effects of a sour bolus on the intramuscular electromyographic (EMG) activity of muscles in the submental region. Dysphagia 2005, 20, 210–217. Roa Pauloski, B.; Logemann, J.A.; Rademaker, A.W.; Lundy, D.; Sullivan, P.A.; Newman, L.A.; Lazarus, C.; Bacon, M. Effects of enhanced bolus flavors on oropharyngeal swallow in patients treated for head and neck cancer. Head Neck 2013, 35, 1124–1131.
- Sciortino, K.F.; Liss, J.M.; Case, J.L.; Gerritsen, K.G.; Katz, R.C. Effects of mechanical, cold, gustatory, and combined stimulation to the human anterior faucial pillars. Dysphagia 2003, 18, 16–26. Mulheren, R.W.; Kamarunas, E.; Ludlow, C.L. Sour taste increases swallowing and prolongs hemodynamic responses in the cortical swallowing network. J. Neurophysiol. 2016, 116, 2033–2042.
- Ding, R.; Logemann, J.A.; Larson, C.R.; Rademaker, A.W. The effects of taste and consistency on swallow physiology in younger and older healthy individuals: A surface electromyographic study. J. Speech Lang. Hear. Res. 2003, 46, 977–989. Abdul Wahab, N.; Jones, R.D.; Huckabee, M.L. Effects of olfactory and gustatory stimuli on neural excitability for swallowing. Physiol. Behav. 2010, 101, 568–575.
- Masilamoney, M.; Dowse, R. Knowledge and practice of healthcare professionals relating to oral medicine use in swallowing-impaired patients: A scoping review. Int. J. Pharm. Pract. 2018, 26, 199–209. Miura, Y.; Morita, Y.; Koizumi, H.; Shingai, T. Effects of taste solutions, carbonation, and cold stimulus on the power frequency content of swallowing submental surface electromyography. Chem. Senses 2009, 34, 325–331.
- Premkumar, L.S. Transient receptor potential channels as targets for phytochemicals. ACS Chem. Neurosci. 2014, 5, 1117–1130. Pelletier, C.A.; Steele, C.M. Influence of the perceived taste intensity of chemesthetic stimuli on swallowing parameters given age and genetic taste differences in healthy adult women. J. SpeechLang. Hear. Res. 2014, 57, 46–56.
- Sasaki, R.; Sato, T.; Yajima, T.; Kano, M.; Suzuki, T.; Ichikawa, H. The Distribution of TRPV1 and TRPV2 in the rat pharynx. Cell. Mol. Neurobiol. 2013, 33, 707–714. Hamdy, S.; Jilani, S.; Price, V.; Parker, C.; Hall, N.; Power, M. Modulation of human swallowing behaviour by thermal and chemical stimulation in health and after brain injury. Neurogastroenterol. Motil. 2003, 15, 69–77.
- Sato, D.; Sato, T.; Urata, Y.; Okajima, T.; Kawamura, S.; Kurita, M.; Takahashi, K.; Nanno, M.; Watahiki, A.; Kokubun, S.; et al. Distribution of TRPVs, P2X3, and parvalbumin in the human nodose ganglion. Cell. Mol. Neurobiol. 2014, 34, 851–858. Nederkoorn, C.; Smulders, F.T.Y.; Jansen, A. Recording of swallowing events using electromyography as a non-invasive measurement of salivation. Appetite 1999, 33, 361–369.
- Yajima, T.; Sato, T.; Shimazaki, K.; Ichikawa, H. Transient receptor potential melastatin-3 in the rat sensory ganglia of the trigeminal, glossopharyngeal and vagus nerves. J. Chem. Neuroanat. 2019, 96, 116–125.Shingai, T.; Miyaoka, Y.; Ikarashi, R.; Shimada, K. Swallowing reflex elicited by water and taste solutions in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 1989, 256.
- Zhao, H.; Sprunger, L.K.; Simasko, S.M. Expression of transient receptor potential channels and two-pore potassium channels in subtypes of vagal afferent neurons in rat. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 298, G212. Pelletier, C.A.; Dhanaraj, G.E. The effect of taste and palatability on lingual swallowing pressure. Dysphagia 2006, 21, 121–128.
- Chee, C.; Arshad, S.; Singh, S.; Mistry, S.; Hamdy, S. The influence of chemical gustatory stimuli and oral anaesthesia on healthy human pharyngeal swallowing. Chem. Senses 2005, 30, 393–400.
- Leow, L.P.; Huckabee, M.L.; Sharma, S.; Tooley, T.P. The influence of taste on swallowing apnea, oral preparation time, and duration and amplitude of submental muscle contraction. Chem. Senses 2007, 32, 119–128.
- Palmer, P.M.; McCulloch, T.M.; Jaffe, D.; Neel, A.T. Effects of a sour bolus on the intramuscular electromyographic (EMG) activity of muscles in the submental region. Dysphagia 2005, 20, 210–217.
- Sciortino, K.F.; Liss, J.M.; Case, J.L.; Gerritsen, K.G.; Katz, R.C. Effects of mechanical, cold, gustatory, and combined stimulation to the human anterior faucial pillars. Dysphagia 2003, 18, 16–26.
- Ding, R.; Logemann, J.A.; Larson, C.R.; Rademaker, A.W. The effects of taste and consistency on swallow physiology in younger and older healthy individuals: A surface electromyographic study. J. Speech Lang. Hear. Res. 2003, 46, 977–989.
- Yajima, T.; Sato, T.; Shimazaki, K.; Ichikawa, H. Transient receptor potential melastatin-3 in the rat sensory ganglia of the trigeminal, glossopharyngeal and vagus nerves. J. Chem. Neuroanat. 2019, 96, 116–125, doi:10.1016/j.jchemneu.2019.01.005.
- Zhao, H.; Sprunger, L.K.; Simasko, S.M. Expression of transient receptor potential channels and two-pore potassium channels in subtypes of vagal afferent neurons in rat. Am. J. Physiol. Gastrointest. Liver Physiol. 2010, 298, G212, doi:10.1152/ajpgi.00396.2009.
- Alvarez-Berdugo, D.; Tomsen, N.; Clavé, P. Sensory stimulation treatments for oropharyngeal dysphagia. In Medical Radiology; Springer: Berlin, Germany, 2019; Volume 0, pp. 763–779.
- Ortega, O.; Rofes, L.; Martin, A.; Arreola, V.; López, I.; Clavé, P. A Comparative Study Between Two Sensory Stimulation Strategies After Two Weeks Treatment on Older Patients with Oropharyngeal Dysphagia. Dysphagia 2016, 31, 706–716, doi:10.1007/s00455-016-9736-4.
- Ebihara, T.; Sekizawa, K.; Nakazawa, H.; Sasaki, H. Capsaicin and swallowing reflex. Lancet 1993, 341, 432.
- Rofes, L.; Arreola, V.; Martin, A.; Clavé, P. Natural capsaicinoids improve swallow response in older patients with oropharyngeal dysphagia. Gut 2013, 62, 1280–1287, doi:10.1136/gutjnl-2011-300753.
- Alvarez-Berdugo, D.; Rofes, L.; Arreola, V.; Martin, A.; Molina, L.; Clavé, P. A comparative study on the therapeutic effect of TRPV1, TRPA1, and TRPM8 agonists on swallowing dysfunction associated with aging and neurological diseases. Neurogastroenterol. Motil. 2018, 30, doi:10.1111/nmo.13185.
- Yamasaki, M.; Ebihara, S.; Ebihara, T.; Yamanda, S.; Arai, H.; Kohzuki, M. Effects of capsiate on the triggering of the swallowing reflex in elderly patients with aspiration pneumonia. Geriatr. Gerontol. Int. 2010, 10, 107–109.
- Tomsen, N.; Ortega, O.; Rofes, L.; Arreola, V.; Martin, A.; Mundet, L.; Clavé, P. Acute and subacute effects of oropharyngeal sensory stimulation with TRPV1 agonists in older patients with oropharyngeal dysphagia: A biomechanical and neurophysiological randomized pilot study. Therap. Adv. Gastroenterol. 2019, 12, doi:10.1177/1756284819842043.
- Shin, S.; Shutoh, N.; Tonai, M.; Ogata, N. The Effect of Capsaicin-Containing Food on the Swallowing Response. Dysphagia 2016, 31, 146–153, doi:10.1007/s00455-015-9668-4.
- Ebihara, T.; Takahashi, H.; Ebihara, S.; Okazaki, T.; Sasaki, T.; Watando, A.; Nemoto, M.; Sasaki, H. Capsaicin troche for swallowing dysfunction in older people. J. Am. Geriatr. Soc. 2005, 53, 824–828, doi:10.1111/j.1532-5415.2005.53261.x.
- Nakato, R.; Manabe, N.; Shimizu, S.; Hanayama, K.; Shiotani, A.; Hata, J.; Haruma, K. Effects of Capsaicin on Older Patients with Oropharyngeal Dysphagia: A Double-Blind, Placebo-Controlled, Crossover Study. Digestion 2017, 95, 210–220, doi:10.1159/000463382.