Non-alcoholic fatty liver disease (NAFLD) is the most common form of liver disease all over the world due to the obesity pandemic; currently, therapeutic options for NAFLD are scarce, except for diet recommendations and physical activity. NAFLD is characterized by excessive accumulation of fat deposits (>5%) in the liver with subsequent inflammation and fibrosis. Studies in the literature show that insulin resistance (IR) may be considered as the key mechanism in the onset and progression of NAFLD. Using natural products, for example, spirulina, oleuropein, garlic, berberine, resveratrol, curcumin, ginseng, glycyrrhizin, coffee, cocoa powder, epigallocatechin-3-gallate, and bromelain, as an alternative approach in the treatment of NAFLD has drawn growing attention among physicians.
1. Introduction
Non-alcoholic fatty liver disease (NAFLD) is a complicated disease impacted by the complex interplay of genetic, epigenetic, and environmental factors
[1][2][1,2]. In addition, several lifestyle factors, such as sedentary lifestyle, westernized diet, and smoking, enhance NAFLD risk
[3].
Unfortunately, mechanisms inducing/worsening NAFLD/nonalcoholic steatohepatitis (NASH) are until now far from being completely clarified
[4]. Nevertheless, there are many lines of research that should be reckoned as highly plausible.
The excessive lipid storage in the hepatocytes of NAFLD patients is represented by triglycerides (TG). The augmented influx of fatty acids (FFAs) derived from the diet, associated with de novo lipogenesis (DNL), and FFAs liberated from the adipose tissue contribute to accumulating TG in the liver, although not in a similar entity. FFAs stored in the liver and secreted via lipoproteins in NAFLD patients originate approximately 60% from adipose tissue, 25% from DNL, and 15% from the diet
[5]. Accumulation of fat in the liver is associated with impaired insulin suppression of glucose production and serum FFAs
[6]. FFAs are liberated by subcutaneous and visceral adipose tissue under the action of cytokines, such as tumor necrosis factor-alpha (TNF-a), interleukin-6 (IL-6), and interleukin-1b (IL-1b)
[7], as well as leptin
[8], while adiponectin (APN) plays a protective role in these molecular signals in the sense that it decreases elevated FFAs by oxidizing them in muscle
[9][10][9,10] (
Figure 1).
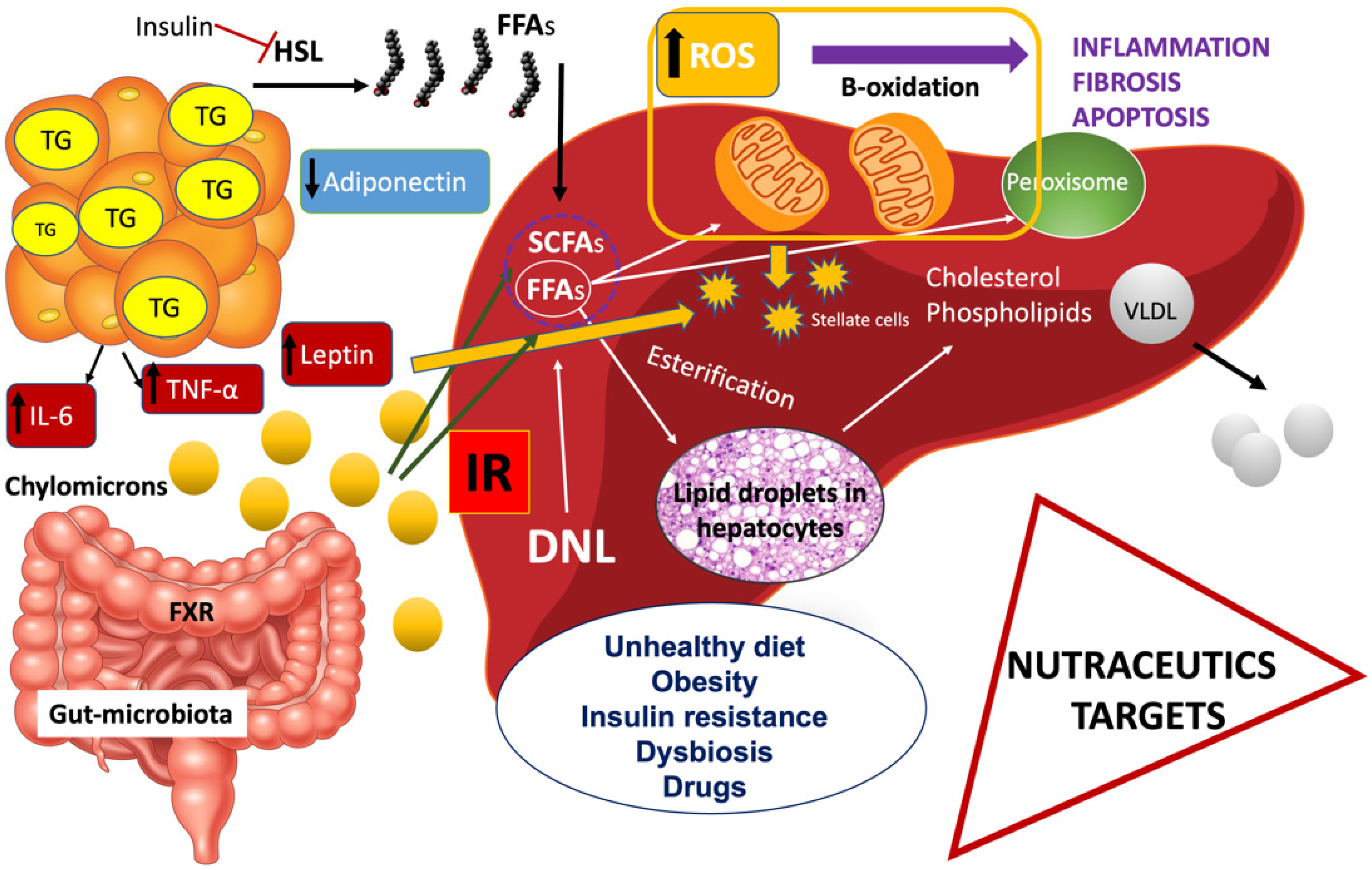
Figure 1. Principal pathophysiologic mechanisms in NAFLD. Insulin resistance (IR) is a multiorgan phenomenon. Additionally, adipose tissue and liver secrete proinflammatory cytokines. An unhealthy diet, obesity, insulin resistance, dysbiosis, and external factors such as drugs contribute to NAFLD progression.
Elevated concentrations of FFAs cause peripheral and hepatic insulin resistance (IR) by inhibiting insulin-stimulated peripheral glucose uptake. Two mechanisms are responsible: (a) a fat-related inhibition of glucose transport or phosphorylation and (b) a decrease in muscle glycogen synthase activity. Interestingly, FFAs stimulate insulin secretion
[11] (
Figure 1).
2. Clinical Trials and Studies in Animal Models
Interestingly, there are several lines of research that have ascertained a likely therapeutic effect of natural products on NAFLD.
Many promising drug candidates are present in the current development pipeline that are of natural origin. Herein chose to select ongoing studies concerning natural products performed in both animal models of NAFLD and in patients suffering from NAFLD with the aim to show the utility of these compounds.
2.1. Alga Spirulina Maxima
Spirulina maxima is a cyanobacterium characterized by a gross content of proteins comprehending essential amino acids and by other factors, including the vitamin B complex associated with various minerals, as well as carotenoids, gamma-linolenic acid, and omega-3 and omega-6 fatty acids
[12][33]. A pilot study, implanted to determine the effects of Spirulina on 55 Cretan patients with NAFLD, orally supplemented with 6 g of this dietary supplement per day, showed at the end of the 6-month intervention period that the mean levels of AST, ALT, gamma-glutamyl-transpeptidase (gamma-GT), triglycerides (TG), LDL-C, total cholesterol (TC), and the ratio of TC to HDL-C were significantly decreased. More interestingly, a significant reduction in weight and HOMA-IR index was found. Unfortunately, no modifications in sonographic features were observed
[13][34]. Three Hispanic Mexican patients were treated with 4.5 g/day of spirulina maxima for 12 weeks; it is interesting that these patients showed a decrease in TG, TC, LDL-C, and TC/HDL ratio. Two of them showed a reduction in parenchyma heterogeneity when ultrasonography was performed, while the third patient showed a complete resolution of the “brilliant liver”, compared with before treatment with ultrasonography
[14][35].
2.2. Olive Oil
Olive oil has been reckoned to have a protective effect on the cardiovascular (CV) system, impacting obesity, type 2 diabetes mellitus (T2DM), and related metabolic disorders
[15][36].
A double-blinded RCT was conducted on 66 NAFLD patients, randomized into two groups, and 20 g/day of either olive oil or sunflower oil for 12 weeks was administered. A hypocaloric diet (nearly 500 kcal/d) was recommended to all participants. The following parameters were examined before and after intervention: fatty liver severity, liver enzymes, anthropometric parameters, blood pressure, serum lipid profile, glucose, insulin, malondialdehyde, total antioxidant capacity, and IL-6. Olive oil only decreased serum AST. Serum TG and fat mass significantly decreased after the ingestion of olive oil. Changes in fatty liver damage grade, as well as in skeletal muscle mass, were most important in subjects who were in the olive oil group, although the trials reported no modifications in body fat percentage
[16][37]. Indeed, the beneficial effects of the Mediterranean diet on human health have been mainly attributed to its high content of extra virgin olive oil
[17][38].
2.3. Garlic
In a recent RCT, 90 NAFLD patients were assigned to take either a garlic powder supplement (1600 mg) or a placebo for 12 weeks. At the end of the study, features of hepatic steatosis were significantly reduced in the treatment group, compared with the control group. Specifically, ALT, AST, and gamma-GT, but not ALP levels, significantly decreased, similar to TC, TG, and LDL-C, which also decreased in the treatment group, compared with the control group
[18][41]. The same NAFLD population, in a parallel study, revealed a reduction in HOMA-IR, as well as a significant increase in skeletal muscle mass, serum concentration of superoxide dismutase, and total antioxidant capacity in the treatment group
[19][42].
An insulin-resistant mouse (ddY-H), a mouse model of NAFLD, showed improved glucose intolerance and reduced hepatic TG accumulation when treated with garlic extract. Additionally, the intestinal microbiota pattern showed a better condition
[20][43].
2.4. Berberine
Berberine (BBR) is reckoned as an alkaloid extracted from plants such as European barberry, goldenseal, and goldthread
[21][44]. A parallel, open-labeled RCT was implanted enrolling patients from three investigation centers. In total, 184 patients suffering from NAFLD were studied and randomly received (1) lifestyle intervention (LSI), (2) LSI plus pioglitazone (PGZ) 15 mg qd, and (3) LSI plus BBR 0.5 g, respectively, for a period time of three months and a half. The authors, interestingly, offered evidence of hepatic BBR content and examined the expression of genes related to glucose and lipid metabolism in an animal model of NAFLD, to which BBR was successively administered. With respect to LSI, the combination of BBR plus LSI ended in a significant reduction in high-fat content (52.7% vs. 36.4%). To this effect followed a consistent recovery in body weight and an improvement in homeostasis model assessment of insulin resistance (HOMA-IR) and serum lipid profiles. BBR only was more functional than PGZ 15 mg qd in lessening body weight and ameliorating lipid profile. It is necessary to highlight the fact that adverse events, likely associated with BBR administration, were mild and affected mainly the digestive system
[22][45].
2.5. Resveratrol
Resveratrol is a polyphenolic compound naturally found in peanuts, grapes, red wine, and some berries. In a double-blind, placebo-controlled RCT, 60 subjects with NAFLD were given two placebo capsules (placebo group) or 300 mg resveratrol capsules (resveratrol group) twice daily for three months. Compared with the placebo group, resveratrol significantly decreased GPT, glucose, and LDL-C, TC, and HOMA-IR. In the resveratrol group, significant reductions in the levels of TNF-a, cytokeratin 18 fragments, and FGF-21 and elevation of APN level were observed
[23][48].
A crossover randomized double-blind study was led, including 44 youth adults, divided into a group intaking 250 mL of bayberry juice twice daily for 4 weeks, and a placebo control group. The first one showed decreased plasma levels of TNF-a and IL-8, proving inhibition in inflammatory and apoptotic response involved NAFLD. Additionally, an increased plasma antioxidant status and HDL-C level were detected
[24][49].
2.6. Curcumin
Curcumin (Cur) belongs to the Curcuma longa species and it is highly present in Zingiberaceae, a member of the ginger family, as well as the turmeric.
NAFLD patients with different grades of disease were enrolled in an RCT, and 1 g/day of Cur was administered for 8 weeks. Supplementation with Cur was associated with a significant reduction in body max index (BMI) and waist circumference in the curcumin and placebo groups. Ultrasound analysis displayed a significant improvement in 75.0% of patients treated with Cur respect to the 4.7% of the control group. Serum levels of ALT and AST significantly slowed down only in the Cur group.
The authors found the Cur administration significantly reduced TG, LDL-C, fasting blood glucose (FBG), HOMA-IR, body weight, and AST levels. However, the observed decrease in TC, HbA1c, ALT, and insulin levels by Cur was not significant
[25][50].
2.7. Ginseng
Many types of this herb are reckoned, but the most renowned ones are American ginseng (Panax quinquefolium) and Asian ginseng (Panax ginseng). In total, 80 patients with NAFLD were prospectively randomized to receive a three-week route of Korean red ginseng (KRG) or placebo. KRG was effective, in overweight patients with NAFLD, in restoring liver functional parameters, as well as in decreasing fat-related cytokines and molecules with antioxidant activity, whereas APN levels were increased
[26][52].
2.8. Glycyrrhizin
Glycyrrhizin (GL) is the main bioactive element of licorice root. In a double-blind RCT, 66 NAFLD patients were enrolled and were separated into two groups: (i) treated group received 2 g aqueous licorice root extract per day for 2 months and (ii) placebo-control group. The authors found that GL administration significantly reduced ALT and AST serum levels, whereas the BMI did not significantly change in both groups
[27][53]. The most important GL-related side effects were: hypertension and hypokalemic-induced secondary disorders
[28][54].
2.9. Coffee
In a prospective, cross-sectional study, 1998 NAFLD patients were studied. Coffee drinking was categorized into no (0), moderate (1–2), and frequent (≥3) consumption (in cups/day). Most frequent coffee consumers (≥3 cups per day) had an inverse correlation with BMI, waist circumference, T2DM, liver enzymes, HOMA-IR, controlled attenuation parameter (CAP), and liver stiffness, in contrast with those who consumed 1–2 cups of coffee per day. In contrast, the female gender positively correlated with HDL-C
[29][56].
Coffee intake reduced hepatic fibrosis in NASH patients. A validated questionnaire was used to assess for a relationship between caffeine and four groups: ultrasound negative (controls), light steatosis/not-NASH, NASH stage 0–1, and NASH stage 2–4
[30][57].
2.10. Cocoa Powder
Recent studies revealed that the consumption of cocoa powder, derived from Theobroma cacao, has a positive correlation with reduced risk of CV and metabolic diseases. However, the mechanisms of its hepatoprotective role on NAFLD were investigated only in limited studies.
Dark chocolate consumption is associated with a decrease in lipid peroxidation. A total of 100 subjects with T2DM were enrolled in an RCT and randomly assigned to the cocoa group (
n = 50; received 10 g cocoa powder) or placebo group (
n = 50), for 6 weeks. Cocoa consumption aimed to show probable interactions with prostaglandin synthase-2 (PTGS-2/COX-2), and it significantly decreased TG, LDL-C, HDL-C, TNF-α, and IL-6
[31][59].
The key mechanism at the basis of clinical benefits of dark chocolate is represented by its polyphenolic compounds, through the ability to inhibit the activity of nicotinamide adenine dinucleotide phosphate-oxidase (NADPH), which is the major source of oxidative stress
[32][33][60,61].
2.11. Green Tea
Epigallocatechin-3-gallate (EGCG), the most abundant catechin in green tea, has antioxidant, anti-carcinogenic, anti-hypertensive, and anti-fibrotic properties
[34][65].
A double-blinded RCT has demonstrated that ingestion of a green tea beverage enriched with catechins with an EGCG -HFD reduced body weight (BW) in 126 obese adult patients. The patients were divided into the placebo, low-dose, and high-dose groups.
BW decreased significantly in the low-dose group and in the high-dose group
[35][66].
The gut microbiota and their metabolites abnormalities are increasingly indicated to be at the bases of NAFLD. In fact, gut microbes produce SCFAs, hydrogen peroxides, trimethylamine, and ammonia. In recent years, several metabolites produced by microbiota have been shown to control lipid, carbohydrate homeostasis, and energy homeostasis in both extrahepatic and hepatic tissues. Oral administration of EGCG in mice fed HFD has effects on the gut microbiota, serum bile acid profile, and gene expression. EGCG significantly improved liver steatosis and intestinal dysbiosis
[36][67].
2.12. Bromelain
Bromelain is extracted from stems of pineapples but is present in all parts of the fresh pineapple. As it is a concentrate of proteolytic enzymes, it may enhance anticoagulant activity (60). In an up-to-date study, HFD mice were treated or not with bromelain (20 mg/kg) for 12 weeks. Bromelain improved BW by ~30%, liver weight ~20%, and adipose tissue ~40%. The pathogenic mechanisms seem to be due to the reduced uptake of FFA by the intestinal wall and the better lipoprotein internalization. Moreover, the bromelain treatment increased bile acid metabolism, cholesterol clearance, the assembly and secretion of very-low-density lipoprotein (VLDL), and the β-oxidation of FFAs
[37][68].
3. Conclusions
Diet and lifestyle modification are the cornerstones of the therapy of NAFLD, although many drugs are on the verge of being licensed.
The authors presented both RCTs and lines of research on animal models suggestive of a possible therapeutical effect by natural products, even though conclusive evidence will be reached with larger sample size studies in different populations, mainly evaluating the possible AEs.